This paper evaluated our 15-year experience with centralization of specialized colorectal cancer service with progressive adoption of MIS at a tertiary care hospital. The phased introduction of laparoscopic and subsequently robotic approaches was undertaken alongside the structured development of the unit, including dedicated multidisciplinary pathways, standardized operative training, and continuous outcome monitoring.
Beyond reaffirming the value of specialized colorectal pathways, our contribution is a pragmatic framework for stepwise MIS adoption. By sequencing simulation and proctored cases, setting explicit credentialing thresholds, codifying escalation/conversion policies, and auditing KPIs in a live registry, we observed increased MIS use alongside improvements in oncologic and perioperative outcomes. We provide phase definitions, credentialing criteria, and KPIs so that developing units can adapt the model to their resources and case-mix.
This dedicated process of unit development enabled a safe and significant transition from open to minimally invasive techniques. Our findings showed that the unit transformation was associated with progressive improvements in oncologic quality, enhanced operative efficiency, and a steady decrease in postoperative complications, confirming the critical role of specialization and institutional growth in achieving high-quality outcomes.
Over the past few decades, colorectal surgery has undergone a significant shift from open procedures toward less invasive alternatives, including laparoscopic and robotic surgery [12]. This evolution has been driven by the well-established advantages of laparoscopic surgery, such as reduced postoperative pain, decreased opioid requirements, shorter hospital stays, and faster recovery of bowel function. Robotic surgery, emerging more recently, offers enhanced three-dimensional visualization, improved ergonomics, and the ability to overcome some of the technical limitations of traditional laparoscopy [13,14,15].
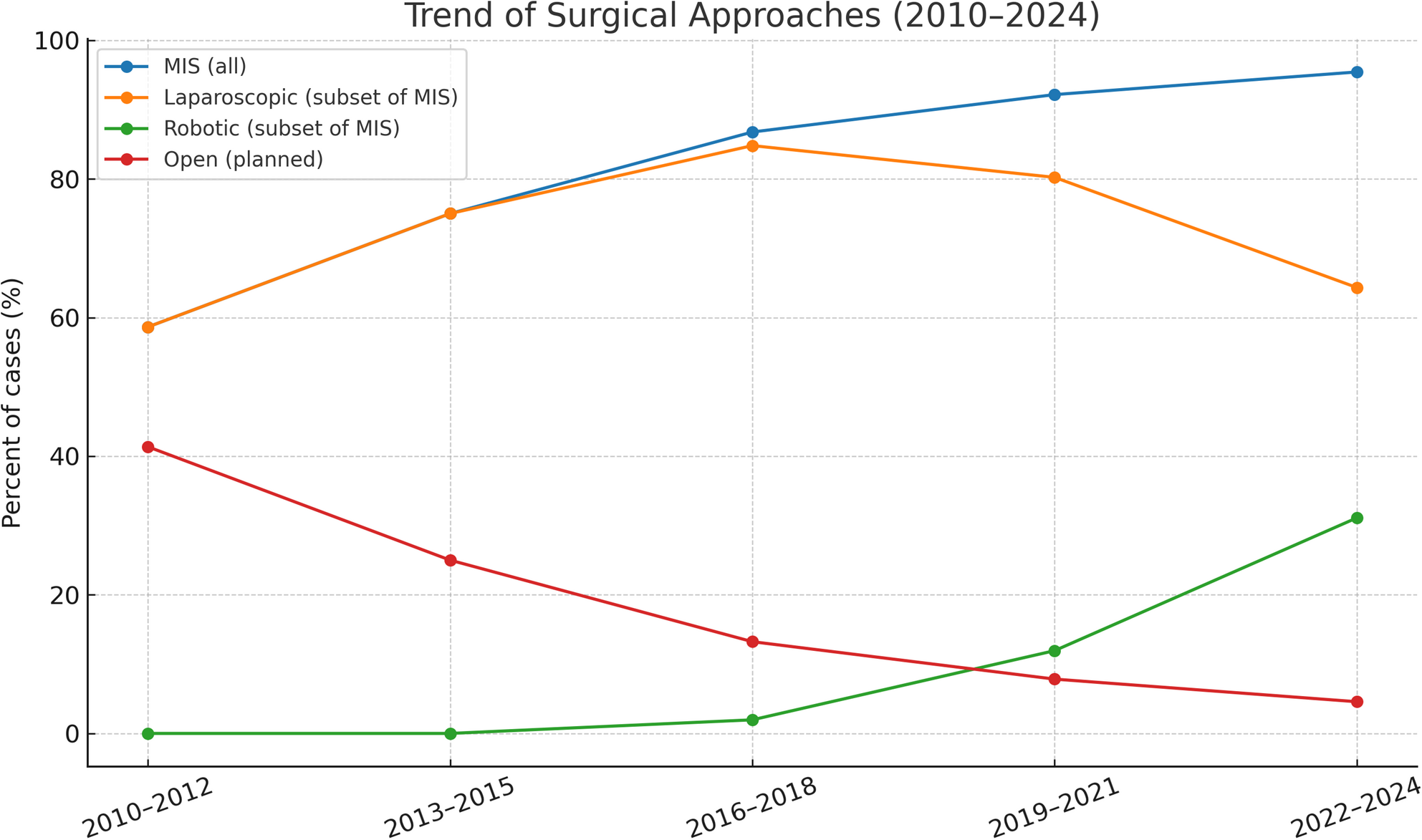
In our colorectal unit, we observed a significant increase in the adoption of MIS over the open surgery throughout the study period, reaching 93% in the most recent 3-year interval. This trend aligns global patterns and is consistent with the findings from the recent study by Azevedo et al., who reported a 90% adoption rate of MIS among 661 patients undergoing colorectal cancer resection at the Champalimaud Foundation in Portugal between 2012 and 2023 [13].
In our study, there was a significant reduction in LOS days. The mean LOS was 6.4 days for MIS compared with 8.4 days for open surgery, decreasing to 5.5 days in the most recent period. Our findings align with published literature, reflecting the impact of unit specialization and structured MIS adoption. The COLOR II trial reported median stays of 8 days for laparoscopic versus 9 days for open surgery, the ACOSOG Z6051 trial found means of 7.3 versus 7.0 days, and the ROLARR trial reported 8 days for both approaches. Specialized centers often achieve even shorter stays. Such as, a large Italian colorectal unit reported median LOS 6 days for laparoscopic resections (vs. 9 days open) [16]. A recent U.S. center found mean LOS 4.35 days after minimally-invasive rectal surgery (vs. 8.48 days for open) [17]. Moreover, these findings align closely with the Azevedo et al. study, which reported a median length of stay of 6.7 days. Krieg et al., documented a mean hospital stay of 11 days among 4,525 colorectal cancer patients undergoing MIS across 36 hospitals in Germany [18].
The maturation and specialization of our colorectal service were central to the outcomes reported. Beginning with the formal establishment of a centralized colorectal unit in 2010, the team introduced an institutional MDT in 2011 (restructured to a dedicated colorectal MDT in 2018) and phased a structured MIS and robotic adoption pathway (first robotic case was 2017). These programmatic milestones, combined with standardized operative modules, stepwise proctoring, and continuous outcome audit, coincided with a progressive shift from open to minimally invasive surgery (51.2% → 93.6%) and a marked reduction in conversions (7.4% → 1.8%). Moreover, oncologic quality improved in parallel, as R0 increase from 87.6% to 96.0%; and ≥ 12 nodes from 88.8% to 96.9%.
A multivariable models showed that calendar time/unit experience (per 3-year step) was the dominant predictor of R0 and node adequacy, supporting a systems-level rather than technique-specific explanation for these findings. At the same time, MIS adoption provides consistent efficiency benefits, up to 2-day reduction in length of stay, without compromising safety. Together, these findings highlight that safe MIS implementation depends less on isolated technology and more on institutional design, centralization, sustained subspecialization, and structured training were key enablers of high-quality, efficient colorectal cancer care in our unit.
We observed a rising rate of R0 resections over the study period, with an overall R0 rate of 92%, indicating a high level of oncologic adequacy across our cohort. While this finding reflects the successful transition from open to minimally invasive techniques without loss of surgical quality, our multivariable analyses indicate that these findings were more strongly associated with the unit maturation and specialization than with surgical approach, after adjustment there was no independent difference in R0 rates between open and MIS procedures. These results are consistent with those reported by Azevedo et al., who observed a 95% R0 resection rate in their cohort, and are supported by major randomized controlled trials in both colon and rectal cancer, such as the COLOR II and ACOSOG trials [13, 19,20,21,22,23].
A major concern during the transition to MIS is the potential for increased perioperative complications during the learning curve and training phases. Interestingly, our study demonstrated a notable decline in complication rate, presented as CD ≥ 3, throughout the study period with an overall rate of 9.9%. This is lower than previously published articles, including the ACOSOG trial that reported severe complications (CD ≥ 3) in up to 22% of patients undergoing laparoscopic resection [22], and also lower than ALaCaRT trial [23]. Our results are comparable to those of Azevedo et al., who reported a 11% rate of CD ≥ 3 complications [13].
Regarding the anastomotic leak, we observed a progressive decline in leakage rates over time, reaching 2.1% in the final study period. However, the trend didn’t reach statistical significance (P = 0.14). The overall rate is 2.7% which is appropriate in comparison to previously published data, including 4.2% in Azevedo et al., 8.5% in the CLASICC trial, 11% in the ROLARR trial, and 12% in the COLOR II trial [13, 19,20,21]. The incidence of anastomotic leak is multifactorial and influenced by perioperative chemotherapy, tumor characteristics, the type and location of the anastomosis, use of diverting stomas, surgeon experience, patient comorbidities, and quality of postoperative care.
Strength and limitations
The strengths of our study are its Large, contemporary cohort (N = 1,142) spanning 15 years, enabling robust temporal analyses, additionally the prospectively maintained database with predefined outcomes improved data completeness. The clear implementation timeline (centralized unit, MDT, robotics) allowed phase-wise evaluation of adoption. Lastly multivariable adjustment for case-mix (age, sex, BMI, ASA, site, procedure).
The limitations included the retrospective, single-center design that may limit generalizability, the period (“time/experience”) may also capture secular improvements (Anesthesia, peri-operative oncology). Moreover, potential selection bias and unmeasured confounding (e.g., tumor stage, neoadjuvant therapy, anastomotic level/diversion, comorbidities). We studied only the short-term outcomes, and for best understanding long-term oncologic and functional outcomes need to be assessed.
Future directions
Incorporate tumor stage and neoadjuvant variables; perform rectal-only stratifications; consider mixed-effects models with surgeon clustering; add sensitivity analyses by intended approach; and report long-term oncologic and functional outcomes as the program matures.

Comments (0)