
Remember me
A 46-years-old male with recurrent depressive disorder was admitted after two previous inpatient stays. After clinical stability for several years under escitalopram, the patient relapsed, and the dosage was unsuccessfully increased. Outpatient attempts, including advanced antidepressant therapy trials (escitalopram, sertraline, venlafaxine, mirtazapine, agomelatine, vortioxetine, bupropion) and combination with adjuvant antipsychotics (aripiprazole, quetiapine, olanzapine) under adequate treatment duration and drug monitoring, failed.
On admission, the patient’s current medication was bupropion extended-release (XR) and olanzapine; later, trazodone was added. Nonetheless, the patient reported severe depressive symptoms, with a Montgomery–Åsberg Depression Rating Scale (MADRS) score of 39 points. Next, intranasal application of esketamine was initiated, stopped due to dissociative side effects and poor antidepressant effect, and ECT was considered.
Preliminary examinations prior to ECT, including routinely performed brain magnetic resonance imaging, electroencephalogram (EEG), electrocardiogram (ECG), and blood laboratory studies were unremarkable, with no reported history of traumatic brain injuries or seizures. Before starting the ECT course, olanzapine was tapered and discontinued. Concomitant medications included 150 mg bupropion XR with plasma levels within the therapeutic range and 150 mg trazodone. A series of ECT treatments was started using a Thymatron System IV device (Somatics LLC; Lake Bluff, IL, USA) with 45% of the nominal charge, right unilateral electrode position, the cuff method to record electromyography (EMG), and anesthesia using 400 mg thiopental (5.6 mg/kg) and 70 mg suxamethonium (1 mg/kg). The optimal anesthesia depth before ECT stimulation was assessed with Narcotrend (MT MonitorTechnik GmbH & Co. KG., Hannover, Germany), an EEG-based monitoring device [9]. After initially sufficient seizures under these settings, subsequent stimulations quality criteria decreased, leading consequently to a stepwise augmentation of charge, switch to bitemporal electrode application from the eighth treatment onwards, and extended administration of 0.5 mg flumazenil to lower the seizure threshold. Since at the ninth ECT, no sufficient seizure could be achieved, it was decided to switch from thiopental to etomidate.
At the tenth treatment, 20 mg etomidate (0.3 mg/kg) was applied without using flumazenil, and an ECT in bitemporal electrode application with 150% of the nominal charge was planned. Clinical signs with preserved spontaneous respiration showed inadequate anesthesia depth after induction with etomidate, therefore the muscle relaxant was not administered. Contrastingly, Narcotrend monitored a value under E30, corresponding to a deep general anesthesia [9]. A few minutes post-etomidate, a spontaneous generalized tonic-clonic seizure occurred, with twisting of the bulbs, flexion of the upper extremities, salivation, and masseter spasm. During this spontaneous seizure, anesthesia was deepened with etomidate 10 mg and suxamethonium 80 mg due to absent protective reflexes and inadequate ventilation. Following propofol 40 mg, convulsive activity ceased, and lorazepam was no longer required. No ECT stimulus was applied in this session.
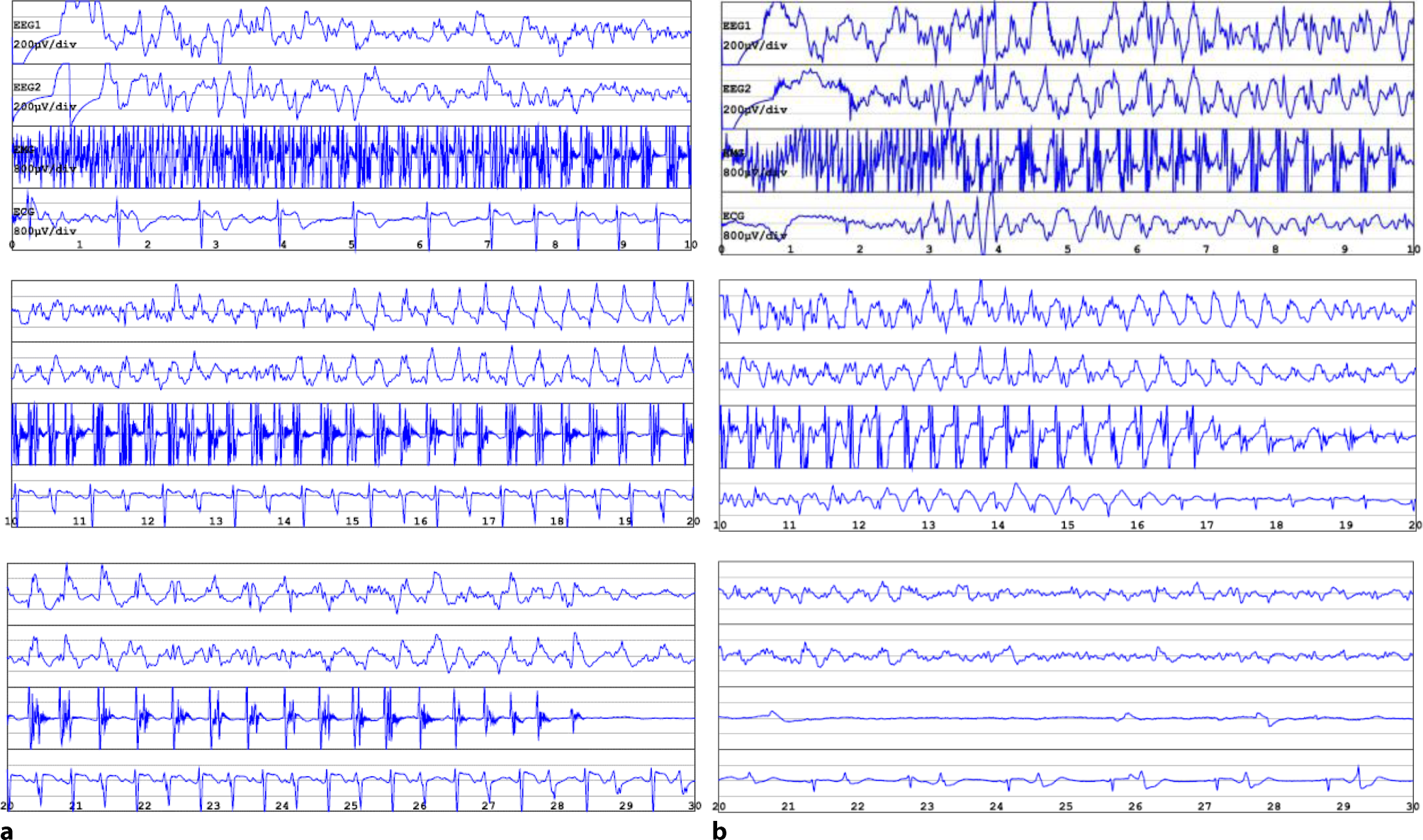
During the spontaneous seizure, recordings of the EEG, ECG, and EMG were collected (Fig. 1a) and exported to GPD (Genie Patient Database; Elektrika Inc.), a software for digital export of ECT data. The patient recovered without complications, without any subjective symptoms or clinical signs suggestive of neurological dysfunction. A follow-up EEG a few hours later revealed a moderate diffuse cerebral dysfunction consistent with the previous epileptic seizure, with occasional diffuse alternating side-emphasized delta/theta activity and intermittently slowed basal rhythm.
Fig. 1
Electroconvulsive therapy (ECT) reports from two different treatment sessions. a Spontaneous generalized tonic-clonic seizure after administration of etomidate, 20 mg: intermittent spike activity on the background of low beta and theta activity turning into spike epileptic activity of low amplitude, slow frequency, and transition to medium amplitude (15 to 20 s), medium frequency, with clear seizure termination (second 29) and poor suppression. b Induced seizure with 140% energy setting and anesthetic thiopental, 400 mg: intermittent spike activity turns into spike epileptic activity of medium amplitude, medium frequency, with less clear seizure termination and poor suppression. EEG 1 and 2 electroencephalogram in right and left channel, respectively. x‑axis time in seconds, y‑axis amplitude in µV. EMG electromyogram. ECG electrocardiogram
The subsequent two ECT treatments, switched back to thiopental 400 mg, showed adequate ECT-induced seizures (Fig. 1b). After 12 treatments, the ECT course was discontinued due to insufficient response, documented by a MADRS score of 21 points, indicating clinical improvement but an inadequate response to ECT. Bupropion XR was increased to 300 mg.
Comments (0)