
Remember me
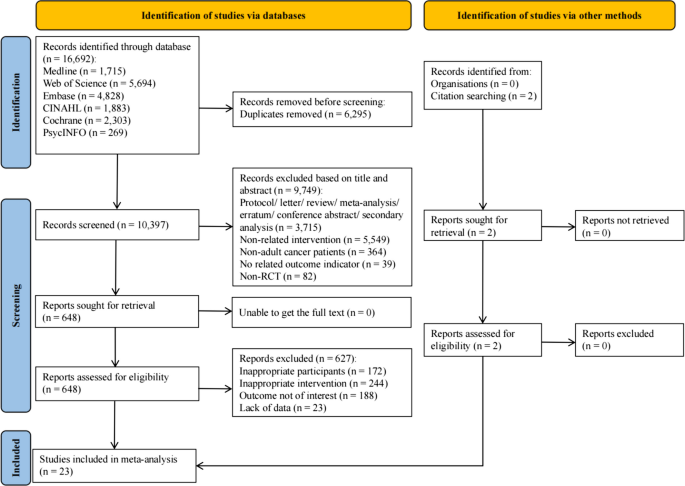

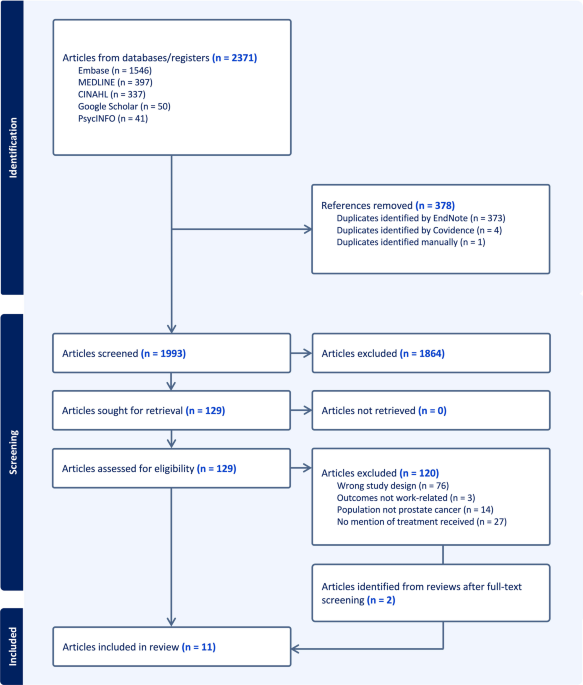
Figure 1 shows the Prisma flowchart. A total of 3,288 records were identified. After removing duplicates, 2,854 records were independently screened by title and abstract by two reviewers (NC & AC). Of these, 48 full-text articles were assessed for eligibility, resulting in 25 papers describing 22 studies (three of the included papers [21,22,23] used the same sample of participants in the papers) in the final review. Key characteristics of the included papers are provided in Table 1. Sixteen of the included papers were quantitative [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39], and nine were qualitative [21,22,23, 40,41,42,43,44,45]. Five quantitative papers were cross-sectional, and eleven used secondary data analysis. The qualitative papers included six that used one-to-one interviews, one that used focus groups, and two that involved content analysis of patient health records. The studies were conducted across five countries: the United States (n = 13), South Korea (n = 8), Germany (n = 2), Australia (n = 1), and the United Kingdom (n = 1). Sample sizes ranged from 18 to 58,886 participants, with a total combined sample of 117,070 individuals. The age of participants ranged from 18 to 86 years. Gender-specific data on participants were not reported in four quantitative studies [34,35,36, 39]. The remaining quantitative papers reported a gender breakdown, comprising 18,075 male and 8,811 female participants. Among the qualitative papers, five included only female participants (n = 99) [21,22,23, 40, 45], while the remaining four included both male (n = 37) and female (n = 44) participants [41,42,43,44].
Fig. 1
Prisma flow chart of articles screened, assessed and included in the review
Table 1 Characteristics of included studiesA wide range of cancers was examined across papers. Fifteen papers included breast cancer, the most common cancer examined across the papers [21,22,23,24,25,26,27,28, 30, 31, 39,40,41,42, 45], followed by eight papers examining gastric, stomach, and colorectal cancers [26, 33, 36, 39, 41,42,43, 45] and prostate cancer, with seven papers [25, 26, 32, 38, 41,42,43]. Other cancers examined included gynaecological [26, 29, 41, 42, 45], lung [26, 37, 39], skin [25, 26, 45] and bladder [26, 45] cancers.
The types of PDs examined also varied across papers, with multiple sclerosis and polio being most commonly examined [21,22,23, 26, 27, 40,41,42,43,44,45]. Twelve of the included studies defined PD using broad or functional terms, such as mobility impairment, chronic difficulty walking, or the use of assistive devices, without specifying diagnostic categories [24, 25, 28,29,30, 33,34,35,36,37,38,39].
Quality AssessmentThe quality appraisal of the included papers is outlined in Supplemental File 2. Ten of the quantitative papers met 100% of the criteria [25, 29, 31, 33,34,35,36,37,38,39], one met 80% [30] due to not meeting the criteria for point 4.3 ‘Is the risk of nonresponse bias low?, and five [24, 26,27,28, 32] met 60% of the criteria also for not meeting the criteria for point 4.3 and also point 4.2 ‘Is the sample representative of the target population? All the qualitative papers met 100% of the criteria for quality appraisal.
Thematic CategoriesFollowing the convergent synthesis of the data, seven key themes emerged: 1) Disparities in access to curative cancer treatment; 2) Personal and hygiene needs not being met; 3) Being overlooked: Dismissal of pain and physical comfort; 4) Unmet emotional and psychological needs; 5) Healthcare environments inaccessibility; 6) Lack of understanding of disabilities and implicit bias and 7) Bridging the gaps through self-advocacy and social support. Table 2 provides an overview of results.
Table 2 Overview of findings across all included studiesTheme 1: Disparities in Access to Curative Cancer TreatmentsAcross the 25 included papers, 16 specifically investigated disparities in access to curative cancer treatments for individuals with disabilities [21, 22, 24, 28,29,30,31,32,33,34,35,36,37,38,39,40] and found that individuals with a PD were less likely to receive curative cancer treatments and or surgery compared to their non-disabled peers. One study [39] also reported that individuals with PDs were less likely to receive cancer treatment in high-volume hospitals, which are typically associated with better clinical outcomes compared to lower-volume centres. As cancer treatment is informed by cancer type [
Comments (0)