Design
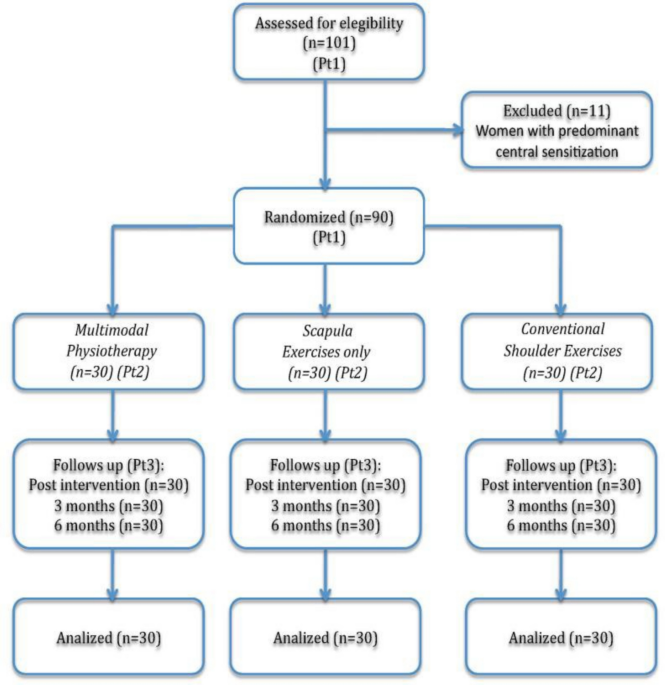
We conducted a single-center, randomized, assessor-blinded, three-armed parallel-group clinical trial of women with persistent pain following breast cancer treatment at the Physiotherapy in Women’s Health Research Unit at the University of Alcalá, Madrid, Spain, between April 2016 and April 2022. The study was conducted according to the Declaration of Helsinki and is reported according to the CONSORT guidelines.
Trial registration: ClinicalTrials.gov, NCT02735668, registered 14 April 2016.
Participants
Participants were recruited at Príncipe de Asturias University Hospital, Alcalá de Henares, Madrid, Spain, through the Department of Gynecology and Obstetrics. Eligibility screening and confirmation of the inclusion and exclusion criteria were performed by a physiotherapist (PT1) who was not involved in the delivery of the interventions or outcome assessment. Eligible women with PPBCT (treated by either surgery and/or radiotherapy and/or chemotherapy) experiencing pain for at least 6 months were invited to participate in the study. In addition, women receiving endocrine therapy during the study were also included. The established exclusion criteria were as follows: shoulder pain prior to breast cancer treatment, bilateral breast cancer, predominant nociplastic pain identified according to the clinical classification guidelines for predominant neuropathic, nociceptive, or nociplastic pain described by Leysen et al. [21], active axillary web syndrome at the time of study inclusion [22], active lymphedema requiring treatment [23], any contraindications for conservative or invasive physiotherapy (infection, fever, metastasis, locoregional recurrence, wounds in the area of the puncture, metal allergy, or fear of needles), neurological disorders, current prescribed or regular intake of analgesic or anti-inflammatory drugs, that could alter the response of the nervous system, shoulder abduction range of motion less than 90°, and cognitive impairment preventing understanding of the study procedures or providing informed consent.
Sample size estimation
With a sample size of 30 participants per group, we estimated 80% power to detect a between-group difference of 2.21 cm in the change of pain intensity measured with a Visual Analog Scale (VAS), and 90% power to detect a difference of 2.55 cm between treatments, assuming a standard deviation of the change of 3 cm. These values were defined a priori as plausible between-group differences in pain intensity, adopting a conservative approach in the absence of directly comparable previous trials. The calculation was performed using a standard t-test with a significance level of α = 0.05. The sample size calculation was performed using R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
Randomization and blinding
Following written informed consent, an equal number of women were randomly allocated using a computer-generated randomization sequence (EPIDAT version 3.1 Xunta de Galicia, Spain, 2010) to one of the three groups: (1) multimodal physiotherapy, (2) scapular exercises, or (3) conventional shoulder exercises. Randomization was also conducted by PT1.
Assessment and data collection
Outcome measurement time points: Each group received a 6-week intervention consisting of one physiotherapy session per week (six sessions in total). Outcome measures were evaluated at baseline (A0), immediately after the intervention (A1), and at follow-up assessments 3 months (A2) and 6 months (A3) after the intervention (A1). A second physiotherapist (PT2) performed all outcome assessments and remained blinded to group allocation. Participants were instructed not to disclose their treatment allocation to the assessor.
Primary outcome
Participants reported their current pain intensity using a 10-cm VAS consisting of a 10 cm horizontal with the descriptors “no pain” on the left and “worst imaginable pain” on the right. The validity and reliability of the VAS have been widely reported. We considered a minimal clinically important difference (MCID) of 1.4 cm, based on studies in patients with rotator cuff-related shoulder pain [24].
Secondary outcomes
The Shoulder Pain and Disability Index (SPADI) is a self-administered questionnaire used to measure pain and disability associated with shoulder disorders. The SPADI contains 13 items that measure two domains: a 5-item subscale that assesses pain and an 8-item subscale that measures disability. SPADI is reliable, valid, and responsive for assessing shoulder pain and disability in Spanish women following breast cancer treatment [25]. A MCID of 17 points has been reported for patients with shoulder pain and disability [26].
Health-related quality of life was measured with the Functional Assessment of Cancer Therapy-Breast (FACT-B) Spanish version 4. FACT-Bv4 is a 44-item questionnaire designed to measure multidimensional HRQoL in women with breast cancer. Higher scores indicate better quality of life. FACT-Bv4 demonstrates ease of administration, brevity, reliability, validity, and sensitivity to change [27]. A MCID of 7–8 points has been reported in women with breast cancer [28].
In addition to the patient-reported outcome measures, the presence of MPS (active MTrP) was assessed in shoulder and axio-scapular muscles according to the criteria of Simons et al. [16], guided by each participant’s clinical pain distribution. Moreover, surface electromyography (sEMG) was used to measure the amplitude of the upper trapezius, lower trapezius, serratus anterior, infraspinatus and middle deltoid muscles during arm elevation performed in the scapular plane [29]. Bipolar Ag/AgCl electrodes (KendallTM 100 Series Foram Electrodes, Covidien, MA, USA) were used and positioned according to the recommendations of Cram and Kasman [30]. EMG data were acquired with a five-channel data recording system PowerLab 15 T (ADinstrument, Oxford, UK) at a sampling frequency of 2000 Hz [29] and processed using LabChart 7 software. The EMG signal was amplified with a gain of 1000, filtered (10–500 Hz), rectified, and smoothed, and the root mean square (RMS) was calculated [29]. A baseline recording was performed with the participant at rest (90° of arm elevation in the scapular plane). Participants then performed three repetitions of a 5-s isometric contraction at 90° of arm elevation in the scapular plane, with 5-s of rest between trials. The amplitude of activation was defined as the average RMS expressed as a percentage relative to baseline activity (RMS%).
Additional variables
At the baseline assessment (A0), demographic and identification data were collected including age, body mass index, and breast cancer therapies. Additional assessments included evaluation of scapular dyskinesis, static scapular position, scapular motor control, pain characteristics, and neural tissue mechanosensitivity.
Scapular dyskinesis
Scapular dyskinesis was assessed by evaluating the position of the scapula during shoulder flexion and abduction. Participants were classified as either pattern 1 (tilting), pattern 2 (winging), pattern 3 (dysrhythmia), pattern 4 (normal scapulohumeral rhythm), or pattern 5 (mixed pattern) [31].
Position of the scapula at rest
The position of the scapula was observed with the participant standing to determine possible alterations in the static orientation of the scapula. The scapula was considered to have excessive anterior tilt when the lower angle of the scapula was prominent dorsally [32], excessive internal rotation when the medial border of the scapula was prominent [32], excessive elevation when the superior angle of the scapula and/or the lateral edge of the acromion were located superiorly relative to the spinous process of the second thoracic vertebra [33], insufficient upward rotation when the medial border of the scapula was not parallel to the line of spinous processes of that same level or with a slight upward rotation (approximately 5°) [33], and excessive abduction when the distance between the root of the scapular spine and the spinous process of the corresponding vertebra exceeded 7.5 cm (Lennie test) [34].
Kinetic medial rotation test
This test was performed to assess control of the scapular muscles. The participant was positioned supine with the shoulder abducted to 90° and the elbow flexed to 90°. The participant’s shoulder was placed in 60° of internal rotation, and the participant was asked to maintain this position while keeping the scapula in a neutral position. The test was considered positive when the scapular moved into anterior tilt, downward rotation, or elevation [32].
Pain characteristics
Pain characteristics were recorded and classified according to the Guidelines for the Clinical Classification of Predominant Neuropathic or Nociceptive Pain described by Leysen et al. [21].
Neural tissue mechanosensitivity
Neural tissue mechanosensitivity was assessed using the Upper Limb Neural Tension Test (ULNT1). The test was performed with the participant in the supine position, following the standardized sequence: step 1: scapular stabilization; step 2: shoulder abduction (90°); step 3: wrist and finger extension; step 4: forearm supination; step 5: shoulder external rotation of the shoulder (70/90°); step 6: elbow extension. A neural sensitization maneuver was then performed by adding contralateral cervical side-bending. To be considered a positive neurodynamic test, symptoms had to be reproduced or exacerbated and further increased by the sensitization maneuver. If symptoms did not increase during the sensitization maneuver, a confirmatory neural desensitization maneuver consisting of ipsilateral neck side-bending was performed. If symptoms decreased during the desensitization maneuver, the test was considered positive, indicating that symptoms could be attributed, at least in part, to neural tissue involvement [35].
Intervention
All interventions were performed by a physiotherapist (PT3) with more than 10 years of experience in these techniques. This physiotherapist was the only study member aware of group allocation. All groups received standardized patient education consisting of six individual one-to-one sessions of 30 min each. The content included the following: (1) basic knowledge about pain neurophysiology, movement impairments, cancer-related fatigue, and lymphedema related to oncological treatments; (2) individualized pain mitigation and management strategies according to each participant’s contributing and aggravating factors; (3) individualized strategies to support exercise continuation, including the use of an exercise diary, self-management strategies, self-monitoring, and recognition of signs and symptoms; and (4) healthy lifestyle habits [36].
Multimodal physiotherapy programScapular exercises
Based on the evaluation of scapular dyskinesis and the kinetic medial rotation test, as well as the individual characteristics of each participant, individualized scapular exercises were prescribed using a motor control approach [32, 37, 38] with emphasis on achieving a neutral scapular orientation [32] (Supplementary data A).
Deep dry needling
Based on the assessment of active MTrPs, deep dry needling was performed according to previously described sterile procedures including standard aseptic technique, using sterile disposable needles [16]. Active MTrPs were identified following the criteria of Simons et al., including a palpable taut band, a hypersensitive tender spot, reproduction of the patient’s familiar pain, and referred pain consistent with the clinical presentation [16]. Muscle selection was guided by each participant’s pain distribution.
A deep dry needling technique was applied using sterile disposable needles. The needle was inserted into the MTrP, and multiple rapid insertions were performed to elicit local twitch responses, typically obtaining 4–5 responses per point when tolerated by the participant. Immediately after needle withdrawal, hemostatic compression and passive stretching were applied to the treated muscle.
The number of treated points per session was individualized according to clinical findings. Dry needling was applied once per session when indicated, within the six-session intervention period. Safety criteria were strictly followed, including prior screening for contraindications such as active lymphedema requiring treatment, infection, metastasis, or local tissue compromise. The procedure was performed by an experienced physiotherapist, and participants were continuously monitored to ensure that the intervention remained within a tolerable and safe range.
Neurodynamic techniques
When the ULNT1 was positive, neurodynamic techniques were included, which consisted of longitudinal nerve gliding techniques based on the ULNT1. With the participant in the supine position, the following standardized sequence was performed: step 1: scapular stabilization; step 2: shoulder abduction (90°); step 3: wrist and fingers extension; step 4: forearm supination; step 5: shoulder external rotation (70/90°); and step 6: elbow extension. Mobilization was by alternately decreasing contralateral cervical side-bending while increasing shoulder abduction, and vice versa, for approximately 90 s. The physiotherapist continuously monitored the participant to ensure that the technique remained pain-free. If pain occurred, shoulder abduction was reduced to remain within a non-painful range [39]. Sessions in this group lasted approximately 55 to 60 min.
Scapular exercises
This group performed individualized scapular exercises following the same criteria described for the multimodal physiotherapy group and as outlined in Supplementary data A [32, 37, 38]. Session duration was approximately 35 to 40 min.
Conventional shoulder exercises
Flexibility and strengthening exercises of the shoulder muscles, commonly used in the management of shoulder pain disorders, were performed, including shoulder joint mobilization exercises, isometric exercises, and resisted exercises using elastic bands (Supplementary data B) [40]. The sessions in this group also lasted approximately 35 to 40 min.
Post-treatment exercise and adherence
After completing the supervised intervention, participants in all groups were encouraged to continue performing their prescribed exercises three times per week until the 6-month follow-up. Exercise adherence was monitored using an exercise diary completed by the participants. During this follow-up period, participants were able to contact the research team if they had any doubts or issues related to the program.
To better understand the factors that could facilitate or hinder adherence to home exercises, a qualitative study was embedded within the clinical trial. A descriptive qualitative design was used, combining focus groups and individual interviews [41]. The study followed the Standards for Reporting Qualitative Research (SRQR) guidelines [42] and the COREQ checklist [43].
Qualitative interviews
Semi-structured individual and group interviews were conducted from a phenomenological perspective to explore participants’ experiences of performing home-based exercises after the intervention.
Individual interviews were conducted first, followed by group interviews with different participants, in order to obtain additional perspectives and richer data [44]. From May 2020 to November 2020, participants who attended the A3 assessment (6-month follow-up) were invited to participate.
Prior to the start of the interviews, an interview guide was developed by a group of three physiotherapists specialized in women’s health, a medical doctor specialized in pain management, and a gynecologist specialized in breast cancer treatment. PT4 conducted individual interviews, while PT5, a physiotherapist specialized in women’s health who was not involved in the clinical trial, conducted group interviews.
The interviews were conducted at the Physiotherapy in Women’s Health Research Unit, University of Alcalá, Madrid, Spain, and audio-recorded with participants’ permission.
Data analysisQuantitative statistical analysis
To evaluate the effects of the intervention on the continuous outcomes (VAS, SPADI, FACT-Bv4, RMS%) at assessment t, we used a separate multiple linear regression model adjusted by baseline (Eq. 1). This approach was chosen as it allows an efficient comparison of between-group differences at each follow-up time point while adjusting for baseline values, providing a straightforward interpretation of treatment effects.
$$(Y_-Yi0)\:=\:\beta1tGi1\:+\:\beta2tGi2\:+\:\beta3tGi3\:+\:\beta4t\ast C(Yi0)\:+\:e_$$
(1)
where Yij is the value of the outcome for individual “i” at assessment “t” (t = 0 at baseline, t = 1 after post-intervention, t = 2 at 3-month follow-up, and t = 3 at 6-month follow-up) and C(Yi0) is value of Yi0 centered on its mean. Gik is binary variable that takes value Gik = 1 when participant “i” belongs to group “k,” coding k = 1 for Multimodal Physiotherapy, k = 2 for Scapular Exercises only, and k = 3 for Conventional Shoulder Exercises. βkt is the mean change in Y in group “k” from assessment 0 to “t” in a “typical” individual with baseline measurement of Y equal to the mean (Yi0 = Mean(Yi0)). β4t captures the regression to the mean, and eit is a random individual error with normal distribution eit~N (0, σe). We did linear hypothesis tests to compare changes between the groups ((β1t = β2t), (β1t = β3t), (β2t = β3t)).
In addition, between-group effect sizes were quantified using Cohen’s d, calculated as the difference between the expected mean differences divided by the standard deviation of the model errors.
To evaluate the effects of the intervention on the binary outcome of myofascial pain syndrome, we used a linear model for proportions depending on group and assessment and the interaction between the two (Eq. 2).
$$_=\sum___+ \sum___+\sum____+_$$
(2)
where Yit is the outcome for individual “i” in assessment “t,” and Vit and Gik are binary variables that take values Gik = 1 when participant “i” belongs to group “k” and Vit = 1 in assessment “t.” Using appropriate combinations of the β coefficients, we can estimate the proportion of participants with the outcome in each group at each assessment. We found that this linear model would estimate correctly the observed proportions while logistic models often fail to converge due to the extreme distribution of the outcome in some assessments.
All statistical analyses were performed using R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
Qualitative analysis
Four researchers manually transcribed the recorded interviews. Each transcript was assigned a code according to the intervention group, type of interview (individual or group), and participant order.
A triangulation process was carried out in which three researchers independently analyzed the transcripts. Through an iterative process, the researchers identified initial codes, discussed their meaning, and subsequently organized them into themes.
Coding and data management were conducted using ATLAS.ti version 6.1 software (Scientific Software Development GmbH, Berlin, Germany).


Comments (0)