
Remember me
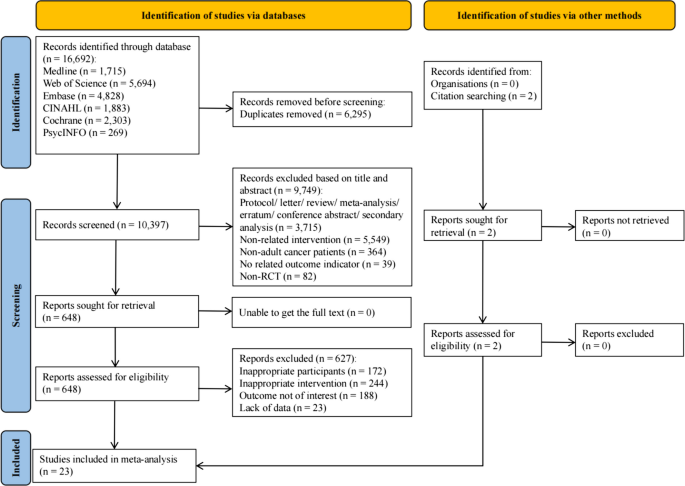

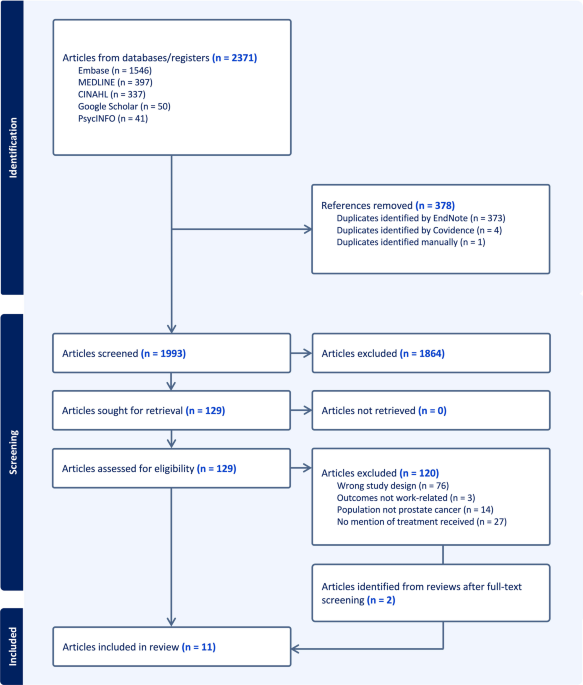
After removal of duplicates, 1993 records were screened at the title and abstract level. A total of 129 full-text articles were assessed for eligibility, of which 120 were excluded (Fig. 1), most commonly due to incorrect study design, lack of relevant work-related outcomes, or population not restricted to prostate cancer (e.g. studies including mixed cancer populations without extractable prostate cancer-specific data). An additional two articles were identified through reference list screening, resulting in 11 studies included in the review [9,10,11, 18,19,20,21,22,23,24,25]. These studies reported qualitative data on the work-related experiences of 302 men who had undergone treatment for prostate cancer (Table 1). Most were conducted in the UK (n = 4), the USA (n = 3), or Canada (n = 2), with one study each from Australia and Sweden. Work-related experiences were the focus of 5/11 studies, while the remaining studies examined topics such as everyday life following treatment, adjustment strategies, and financial difficulties. Two studies only included men treated with radical prostatectomy (RP), one only those who received external beam radiation therapy (EBRT), while most samples included men who received various treatments including RP, radiotherapy, hormone therapy, chemotherapy, and/or active surveillance (AS)/watchful waiting (WW). Occupation was reported in 5/11 studies, generally in broad terms such as white-collar vs. blue-collar or professional vs. manager.
Fig. 1
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram
Table 1 Characteristics of the 11 included studies exploring work-related experiences among men treated for prostate cancerRisk of bias assessmentOf the 11 included studies, nine were rated at moderate risk of bias, and two at low risk (Supplementary Table 6). No studies were assessed at high risk of bias. There was universally low risk of bias across most categories (Supplementary Fig. 1). However, only two studies clearly articulated a philosophical perspective, only one included a cultural or theoretical location statement, and none addressed the influence of the researchers on the research or vice-versa. Additionally, several studies did not clearly report ethics approval.
Thematic synthesis resultsTen descriptive themes were developed inductively and integrated into six analytical themes (Table 2): (1) return-to-work timing and trajectories; (2) financial pressures and economic trade-offs; (3) support systems; (4) treatment side effects and stigma; (5) adjustments and adaptations; and (6) work identity, values, and priorities. Direct quotes from study participants are indicated in italics using quotation marks; quotes from study authors are presented in italics without quotation marks.
Table 2 Analytic and descriptive themes on work and prostate cancer survivorshipReturn-to-work timing and trajectoriesMen described highly variable pathways back to work following prostate cancer treatment. For some, the impact was minimal: “I missed a few days initially when I had the treatment, but other than that it doesn’t affect my ability to do my job” [10]. Others, meanwhile, experienced longer absences than expected: “For the second surgery, the recovery was much more difficult than they led me to believe. They were saying I can go back to work in like a week or two, that [ended up] being more like six weeks” [10]. For some, continuing to work was not a matter of choice but of circumstance, particularly among those who were self-employed: “If you were to ask me if I were employed by someone would I be back at work. I guess if I wasn’t self-employed, I wouldn’t be at work. But I am self-employed, and I always have been, so when I get a cold or sore throat my first thought isn’t ‘I’ll stay in bed today’. I’ve got to go to work” [9]. Others highlighted the necessity of keeping business activity alive even during recovery: “If I stop work that means marketing isn’t done which means work doesn’t come in. It’s not as if I had a choice of diving into work” [21].
Some men described intermittent or staggered participation in work, often linked to changing demands of treatment: “I did the [first] work for about eighteen months. I took a break for about six months and then I got the opportunity to [do the second work] … I’d had a break from the hormone therapy at the time I started [the second work], so I was sort of feeling a lot better… When I finished the project and I’d had to go back on the medication that I felt like I really sort of hit the wall and went into a bit of a slump” [21]. Others reported a gradual expansion of workload over time, such as one who noted that initially he “could only work for a few hours a day”, but later, when surgical wounds healed, “I started working eight or more hours a day” [25]. These narratives also emphasised the ongoing process of evaluating one’s own capacity: “I was feeling stronger by the fifth or sixth week (after returning to work) and I thought I could start working on the larger projects. But I didn’t tell my clients and decided to wait until I was totally certain that I could handle the work” [25].
Work, however, was rarely discussed in pre-treatment consultations, leaving some men unprepared for the trajectory ahead: “No [discussion about work], not really, it was only advised to take it a bit easier with the lifting until things had healed properly” [21]. Others expressed frustration at the lack of information about treatment side effects and their implications for work: “I don’t feel like I was adequately informed around the impacts of treatment, particularly the hormone therapy … It affects your cognitive function so I felt like I couldn’t [work]” [21].
Financial pressures and economic trade-offsThe financial burden of prostate cancer treatment was shaped by employment type, access to benefits, and household responsibilities. While some men were able to manage costs through paid leave or employee assistance programmes, others faced significant economic strain. Those with adequate leave described relief: “I was very fortunate that I had plenty of leave time” [10], and employer-provided health insurance could protect against major financial hardship: “I’ve maintained a job that provides me health insurance, which is the reason I could get the care that I did. Having health insurance, I have not had to suffer from this financially, hardly at all” [10].
Men in commission-based or self-employed roles experienced more immediate financial consequences: “I have the type of job where I get paid a base salary and commission, so obviously during the period of time that I wasn’t working, I wasn’t selling anything, so the commission side of my income went down” [10]. Self-employed men often faced direct income loss: “No work no pay… there’s not really any sick leave or annual leave, it comes out of my pocket either way” [21], and some had to close businesses due to sudden health deterioration, with ripple effects for their households: “So I sold my business, which is helpful having that money in the bank, but basically that was before retirement… So, my wife ended up working for longer than she really would’ve had to” [20]. Financial pressures also influenced the urgency to return to work, sometimes overriding readiness or recovery considerations: “I have a family, a mortgage and people to pay. I just had to come back [to work]” [25].
Support systemsSupport systems emerged as central to men’s recovery and return to work. Employers were often described as going beyond formal entitlements to demonstrate loyalty and care, particularly for longstanding staff: “I’ve been with [company] for 35 years, but I was in a status where I didn’t have benefits. [The administrator] said, ‘So, what we’re going to do is we’re going to pay you for all your time off anyway. We just feel that’s the right thing to do’. And took it out of the [company’s] budget. So, I got great support from everybody” [10]. Others reported colleagues stepping in when health needs interfered with work: “We were able to work around the times when I had my immune system down, I was able to get support from other people within the group” [21]. Supportive reintegration into the workplace was also highlighted as meaningful: “When I walked in, of course everyone was delighted to see me, I was welcomed back, and I was only there for two hours or so, and they joked, and things slowly built up” [24]. Access to occupational health staff provided another avenue of reassurance: “The occupational health nurse is a lovely person altogether. She told me that if I ever needed anyone to talk to, I was to go down to her” [24]. For many, disclosure of their diagnosis, though initially daunting, became the gateway to greater understanding and support: “Once you let people know, you get a lot more support” [21].
Families played an equally pivotal role, providing emotional encouragement, assuming household responsibilities, and adjusting routines to protect men’s recovery. Several described their partners’ patience and determination: “My wife from the first day, for the first second was, ‘we’re going to beat this’. She had a very strong attitude about it. She’s been very, very patient with me” [20]. Community cancer services were also identified as “a big help” [21] in navigating financial supports, though some men felt that in local cancer support groups, work-related issues or information were rarely discussed [21]. Additionally, some reported frustration with disability job providers, describing “extremely … no support from them” in accessing meaningful assistance [21].
Treatment side effects and stigmaTreatment side effects, particularly incontinence, shaped men’s experiences of returning to work and often carried a stigma that was more disruptive than the cancer itself. Coping strategies were sometimes invisible to colleagues, but privately burdensome: “I had a catheter for six months, so that affected me at the time. I was able to work. I was working. My work schedule was as regular as ever. I just had a bag on my ankle, which nobody knew about” [10]. For others, the need to manage pads or bags in social contexts highlighted a sense of social difference compared to colleagues: “If you can imagine two or three blokes in a meeting, you take your comfort break, everyone trots off for a pee. They’re all going to these appalling looking urinals that blokes use. I’ve got to trot into a cubicle and change a pad. It’s kind of socially abnormal” [9].
Other physical effects of treatment also interfered with both cognitive and manual work. Fatigue was frequently described as impairing decision-making capacity: “The fatigue [is] like that, it’s not just physical, because it affects your mental processes as well. After a while you find you can’t think clearly, so you’re not in the right space for making proper management decisions” [21]. Surgical wounds and dizziness also restricted tasks requiring strength or balance: “I was concerned with lifting heavy objects because of the (surgical) wound. So, I couldn’t do that until it healed completely. But I also felt dizzy at times. That ruled out any work that required (climbing) the ladder or reaching high-up unless there was someone to help me” [25].
Stigma extended beyond bodily symptoms to concerns about social perception and employability: “You are thrown back into it and you wonder how you will be received, whether people will say ‘Here he comes, he’s been loafing off for three months’” [9]. Others experienced overt reactions that made them feel different or stigmatised: “When you get around the individuals, their mouth drops … their eyes get big, and they look at you. I’ll say, ‘Yeah, okay, I’ve got cancer. And I’ve dealt with that issue’. Let’s get over the… shock, [I’m] not damaged goods. I often felt like that when individuals would talk to me and look at me sometimes” [11].
Adjustments and adaptationsMen described a range of adjustments to accommodate treatment-related effects while maintaining work participation. Some arranged shifts around treatment schedules: “I’m on shifts but I arranged with work so I could go in and stay on the morning shifts so I would go in to work for 6 o’clock, finish at 10 o’clock, come home get changed go to … and have the treatment” [18]. Keeping employers informed allowed work to be scheduled around medical needs: “I kept them up to date on the whole process … so it was all discussed with my boss, and they scheduled things around me” [21]. For self-employed men, control over hours was essential to accommodate recovery, while practical modifications included changing delivery routes: “I was on a van route, but it was a long day, and I asked to be put on a shorter route” [24].
Adaptations often involved modifying the type of work undertaken. Post-surgical fatigue or physical limitations led some men to pursue less technical tasks or shift into different areas of the business. This allowed them to remain productive while managing their capabilities: “I didn’t think I could do the technical stuff as well as I used to, and I didn’t want to take it easy when everybody else was working hard. So, I pondered about doing something else instead” [25]. Opportunities to take on new responsibilities also supported ongoing engagement: “I couldn’t work in the (machining) shop. Luckily, the owner was looking to expand the business … So, I told the owner I could do some marketing and help out that way. That’s how I began to learn about promoting our company and incorporated marketing into my job description” [25].
Supportive workplaces were valued for providing flexibility and understanding. Survivors emphasised the importance of employers adapting responsibilities to side effects and allowing “breathing room” or “a space to recover” while at work [11]. Few men expressed a desire to change jobs, reflecting sustained interest in their role, a belief that they were too old to change or that it would be difficult to obtain a new job following a cancer diagnosis [9].
Work identity, values, and prioritiesWork held multifaceted significance for men following prostate cancer treatment. For some, it was central to their identity: “The only way I know how to live my life is if I work and my work is my life” [9]. Work also represented a sense of normality and continuity: “I think work has a highly influentially symbolic role for a lot of people and it’s very closely associated with people’s sense of identity and worth … Certainly in my own case, I knew from the outset that I wanted this to be the shortest hiccup in my working life” [9]. In this context, work could be therapeutic, offering a distraction from the illness and a challenge that prevented rumination: “I think work was very therapeutic. I mean if I’d sat at home contemplating how terrible life was. That would be awful. I was very lucky to have, you know, a challenging job that kept me going” [9]. Even during treatment, work served as a coping mechanism: “I was going to work [during treatment]. I finished my external beam radiotherapy nine to nine‐fifteen [in the morning] and at ten o’clock, I am [working]. That was the way I could cope” [22].
For others, work was framed more pragmatically, as “a necessary evil” [21] or a role sustained primarily for financial reasons, prompting reassessment of priorities: “We never listen to our bodies. I learned the hard way. Now, I take half a day off to see the doctor, even if it is for a minor thing” [25]. Following treatment, many men also reflected on life beyond work, expressing a desire to enjoy retirement: “I don’t want to work forever. I’m not one of those people. I want to enjoy life. There are things that I’d like to do while I’m still able. I’d have no problems in retiring soon” [25], and focus on family: “I thought about this for a long time and felt that I should retire if the conditions (at work) were right. Instead, I could spend more time with my family” [25].
These experiences illustrate how prostate cancer prompted a recalibration of priorities, balancing work commitments with health, family, and personal goals. Men emphasised positive attitudes: “Surgery makes you see things differently. You are the same person up here (points at his head), but the body has changed. Up here (points at head), you wanna do the things you did, but your body says: ‘Nope. You can’t’. So, you work around that. You prioritize doing the things you can do and look for a happy medium” [25] and determination as central to navigating post-surgical challenges: “I didn’t give up. I kept telling myself: ‘I can’t let it win’” [25]. Work, whether central to identity or sustained for practical reasons, remained a critical domain through which men negotiated recovery, resilience, and life post-treatment.
Patterns across treatment types, age groups, and employment typesSome tentative patterns were observable across the included studies. Narratives concerning incontinence and its impact on workplace stigma were most prominent among men who had undergone radical prostatectomy [9,10,11, 25]. Fatigue and cognitive difficulties were described by treatment, with hormone therapy specifically linked to cognitive impacts on work in some accounts [21]. Self-employed men consistently described greater financial pressure and earlier-than-desired return to work compared with salaried employees, who more often had access to paid leave and graduated return arrangements [9, 21, 25]. Older men and those nearing retirement more commonly framed prostate cancer as prompting a reprioritisation toward health and family [20, 21, 25], whereas younger men more frequently emphasised work as central to identity and breadwinner roles [9, 23]. These observations should be interpreted as exploratory, given the heterogeneity of the included studies and the limited stratification of findings in primary reports.
Comments (0)