
Remember me
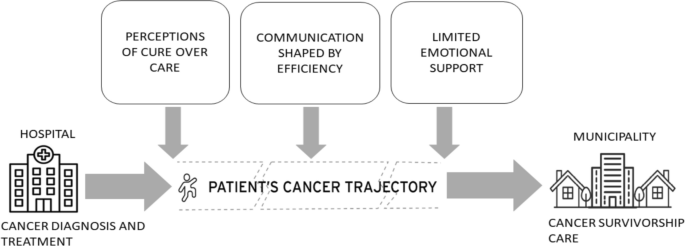

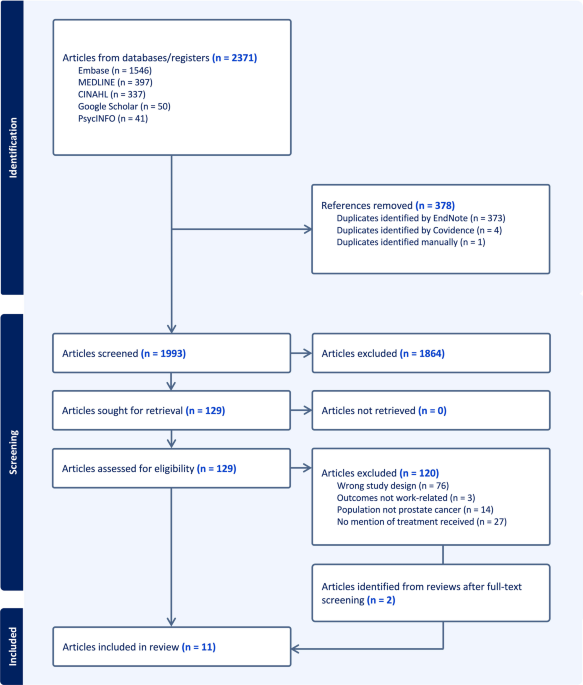
The analysis explored the experiences of patients with colorectal cancer, focusing on their interactions with healthcare professionals. Three interrelated themes emerged: cure over care, highlighting how biomedical priorities often overshadowed emotional support; communication shaped by efficiency, showing how time constraints and fragmented care reduced patients’ sense of being acknowledged; and limited emotional support, reflecting feelings of abandonment, particularly during the transition from active treatment to life after cancer. Figure 1 provides an integrative overview of how these themes interact across the cancer trajectory, illustrating how structural and interactional factors jointly shape patients’ experiences of needs assessment and their transition to survivorship care.
Fig. 1
Impact of key themes on the colorectal cancer care trajectory. The figure illustrates how the three interrelated themes “cure over care,” “communication shaped by efficiency,” and “limited emotional support” affect patients’ cancer trajectory. Based on field observations and focus group interviews in the outpatient clinical setting following colon cancer surgery, it was evident that interactions around needs assessments were often shaped by structural and efficiency-driven priorities. This contributed to a fragmented care pathway, where limited emotional support complicated the assessment of patients’ needs across the entire trajectory, from hospital-based diagnosis and treatment to follow-up and survivorship support in the local community
Perceptions on cure over careAcross observations and interviews, a dominant structural focus on biomedical outcomes over psychosocial care emerged clearly. This emphasis was manifested not only in the patients’ narratives but also in the daily routines and discourses of the healthcare professionals.
The healthcare professionals followed routines guided by checklists and standardized procedures. The encounters with patients were typically brief, task-oriented, and centered on specific clinical issues, such as information on lab results, surgery and treatment, or on treating isolated symptoms. The patients were moved efficiently through a predefined process with minimal dialogue about their broader situation or emotional needs. The focus was mainly on ensuring surgical success, which could result in patients being considered cancer-free, whereas there was less emphasis on supporting the person holistically.
The healthcare professionals appeared to work in a highly structured manner with a clear focus on documentation and task completion. The structural focus left a strong impression on the patients. From the patients’ perspective, the structural focus overshadowed other issues. One participant shared:
ID number 8:
…because in my case, everything just happened so fast – I mean really fast. You knew nothing, right? You leave here, and then the following Monday you find out you have cancer, and then you’re having surgery, and everything is just spinning. I mean, the nurses at the department were great – you really can’t point a finger at anything – but maybe it would have been nice if there had been someone who knew a bit more… someone who could, what’s the word, spend half an hour or an hour just stopping by to talk about what was going on, because you have no idea! Everything is just moving ahead at full speed, and you can’t keep up at all! So, it might have been nice… someone saying, “This is what’s happening now, and yes, you might expect this or that”, you know?
The structured, task-oriented approach left little room for the meaning-making processes that patients undergo in transitioning from an “ordinary person” to a “cancer survivor.” The lack of emotional scaffolding during and after surgery disrupted the patients’ identity reconstruction and reinforced a sense of emotional isolation. The patients struggled to interpret what it meant to be “done” with treatment when no one addressed their internal experience or psychosocial adaptation.
ID number 2:
I was told I was a free man. But it left me with a hollow, empty feeling. When I walked out of there – of course, if I could, I would have lifted a little off the ground. But I felt empty… You walk away and then think: what now? I know I’m supposed to have a scope examination next year, and then again in five years…
Meanwhile, the healthcare professionals, constrained by structural demands, rarely had the time, the space, or the systems in place to engage with the patients beyond clinical tasks. Moreover, although it was beneficial for multiple specialties and sectors to be involved in the patient’s cancer trajectory, there was room for improved coordination. Thus, the hospital provided no or limited information about the cancer survivorship care that was available through the local community setting. One patient stated:
ID number 4:
If I hadn’t spoken to you, I think I would’ve felt much more on my own. However, because I talked to you and was referred to cancer survivorship care, I felt stronger. I think having had cancer is such a huge and horrible thing. And then they just say, “Well, now it’s gone – poof” (makes a sound and a hand gesture like someone being pushed along). “We’ll see you in a year”. And you’re left standing there with all the uncertainty and anxiety.
Ultimately, this theme illustrated how a healthcare system structured around cure can inadvertently neglect care. Although it is essential to prioritize measurable biomedical outcomes, doing so leaves a gap in the emotional and relational support, particularly at critical transition points, which compromises the holistic well-being of patients navigating the cancer trajectory and neglects the benefits of cancer survivorship care.
Perceptions of communication shaped by efficiencyIn general, the patients had a positive view of the communication at the hospital; however, many observed that the healthcare professionals appeared extremely busy during outpatient appointments. The intense pace of work was evident even before the consultations began. The patients described seeing healthcare professionals pass by with hurried steps, often without making eye contact or offering a greeting, while they were waiting in the outpatient area. Rather than reacting negatively, many patients expressed sympathy for the healthcare professionals, noting how overwhelmed they seemed and acknowledging the pressures of the healthcare system.
Despite this understanding, many experienced the outpatient setting as impersonal and rushed. One common concern was the healthcare professionals’ failure to review the patient’s medical records before the appointment, which led to feelings of being undervalued or unseen. One participant explained:
ID number 4:
Yeah and when I’ve been called in for scans and things like that, it’s been fine. But I’ve also been called in for outpatient consultations every time, so they could explain the results to me… but that part has been a bit inconsistent…. I’ve been told different things, and… well, when you show up and start explaining how you’re experiencing it – they say, “oh, I haven’t read that” – and then they have to read my medical record. There’s been a lack of preparation. I know things are busy. Yes, there’s a lot you can go in and read in a medical record, right? And they might miss something if they don’t read all of it! So yeah…
These communication issues were further illustrated by observations documenting that the healthcare professionals often turned their backs on patients or focused on their computers during the interactions. Although it was presumably unintentional, such physical disengagement symbolically conveyed a lack of interest.
These micro-interactions played a central role in shaping the patients’ perceptions of their place within the healthcare system. When the professionals appeared unprepared or failed to acknowledge the patients’ emotional or informational needs, it disrupted their sense of connection and mutual understanding.
ID number 5:
I felt completely alone in all of it. The doctors and nurses were kind, but they never really asked how I was doing mentally. It was only about the physical issues. However, I wasn’t prepared for how hard it would hit me afterwards. I thought I had the surgery, and then everything would be fine – but I completely broke down. I really sank into a dark place, and I thought… I wasn’t prepared for that! It would have been nice to hear other healthcare professionals say, “well, that’s very normal,” and then I could have thought – okay, that makes sense...
Many participants expressed a strong need for support in navigating life after cancer. In outpatient settings, the focus often remained on biomedical outcomes and clinical follow-up; however, the patients longed for a more holistic attention to their emotional, physical, and practical needs. Several patients reported that cancer survivorship care was rarely introduced unless they themselves brought it up. One patient stated:
ID number 3:
Well, maybe it should have been the staff in the outpatient clinic who was responsible for referring you further into the system, now that I think about it. Because otherwise, no one does anything! You’re left to handle it on your own. It might be a good idea if they took a moment to explain what kind of cancer survivorship care options are available – or simply asked how you’re doing… It’s a bit difficult when you come in for that consultation, because at that point you’re just focused on getting the results from the surgery. So, you don’t even think about what comes next. I think you really need someone to guide you for that next step afterwards. But I’m not even sure it’s their responsibility, right? Because they’re so busy. The next patient is already waiting to get their results. That’s why it’s much better to be picked up afterwards by someone like you. That’s my personal experience.
Notably, many patients expressed uncertainty about the needs assessment prior to the cancer survivorship care. Several patients recalled that they had been contacted on the phone following their postoperative appointment and that they had not realized that this conversation was meant to assess their needs. Although needs assessments were intended to be conducted routinely as part of follow-up care, patients often did not perceive these interactions as formal or systematic assessments of their broader survivorship needs. In several cases, the conversations primarily focused on physical symptoms, bowel function, pain management, or practical treatment-related issues. Consequently, patients did not necessarily interpret these encounters as opportunities to discuss emotional, psychosocial, or existential concerns related to life after cancer. Some remembered receiving a need assessment form during their outpatient appointment but did not link it to a systematic needs assessment process. In these previous interactions, the focus had largely been on physical symptoms such as bowel movement frequency, stoma-related issues, or pain needs, which are prioritized by healthcare professionals as relevant to the cancer trajectory. These were not always the needs that the patients themselves felt were most urgent or for which they experienced an emotional need for support.
In sum, this theme illustrated how efficiency-driven communication limited the opportunities for emotional connection and individualized care. Although the information was often clear, the outpatient interactions felt rushed and impersonal, which left patients unsupported in navigating life after treatment. Many were unaware that needs assessments had taken place or misunderstood the purpose, as the focus remained on clinical symptoms rather than the patients’ own concerns. The constrained approach to communication risked overlooking the broader emotional and practical needs of cancer survivors.
Perceptions of limited emotional supportOne striking theme across the patients’ experiences was a pervasive sense of emotional isolation, particularly in the transition from active treatment to life after cancer. Although most of the patients felt well cared for medically, they consistently described a lack of emotional care and support during their hospitalization and an even more profound void following the conclusion of treatment.
The participants often described the experience of having to navigate the cancer trajectory largely on their own. Several noted that their emotional needs were not always fully acknowledged by the healthcare professionals, whose primary focus tended to be on the biomedical outcomes. This dynamic was also observed directly. During follow-up appointments, some patients became visibly emotional after difficult discussions. Although the clinical environment prioritized efficiency and task completion, a few healthcare professionals responded with subtle expressions of empathy, such as sustained eye contact or a reassuring touch. Nonetheless, the structured routines of clinical care appeared to offer limited opportunities for emotional connection.
The hospital functioned as a stage on which the patients’ enacted roles of illness, dependency, and recovery, affirmed through structured interactions with the healthcare professionals. When these interactions ended abruptly, the social and symbolic scaffolding that had upheld the patient identity dissolved as well. The sudden lack of follow-up or emotional inquiry left many patients in a liminal space: They were no longer patients but were not yet fully recovered or “whole.” The sense of abandonment was intensified by fears of recurrence and uncertainty about the future. As another participant shared:
ID number 1:
I thought I would feel relieved when the treatment was over, but instead I just felt abandoned. Suddenly there were no follow-up appointments, no one to talk to – it felt like I was left to figure everything out on my own. I think it feels quite overwhelming. It seems like you hear a lot and read about so many people who have had cancer. I know several people with the same type of cancer, and then it comes back a few years later. They get cancer again. I find myself thinking a lot about that – “what if it comes back in a few years?” Did they really get everything when they removed it? That’s definitely something that lingers inside me... the thought of it coming back!
These ongoing anxieties were not merely private but reflected a lack of external validation or interactional space to process postoperative fears. Without shared meaning-making, the participants internalized solitude and insecurity as key features of survivorship. One participant explained:
ID number 2:
I think it feels very overwhelming. You hear a lot and read about so many people who’ve had cancer. I know several people with the same type of cancer, and then a few years later it comes back. They get cancer again. That’s something I think a lot about – “what if it comes back in a few years?” Did they really get everything when they removed it? That’s definitely something that sits with me… the fear that it might come back. And I also find it difficult that there’s such a long time between the follow-up exams – a scan now, and then not until five years from now before the colonoscopy. I had my final consultation last week, and no one even asked how I was really doing.
Furthermore, many participants mentioned that although their families had the best intentions, they were not equipped to provide emotional support, partly because they also lacked guidance or help from the healthcare system. One patient described:
ID number 4:
My family tried to be there for me, but they didn’t fully understand, and they also didn’t receive any help in dealing with it.
This limited the patients’ ability to share their needs openly, which deepened their sense of emotional isolation. Importantly, some patients noted that brief interventions offered meaningful moments of mutual recognition that helped restore the symbolic coherence to the patients’ postoperative identities. For many, even small gestures of empathy from a healthcare professional carried significant emotional weight and contributed to a sense of being seen, supported, and emotionally met during a vulnerable phase of recovery. As another participant shared:
ID number 4:
With you, it was more about the person – about how the whole process had been and what I needed to feel like myself again, in a way. I thought it was a good conversation, and you were very empathetic in the way you approached me as a patient. I was also contacted by cancer rehabilitation the following week, and that was because you had reached out to them. So, I thought that was really great.
Ultimately, this theme revealed that the transition from treatment to everyday life after cancer was marked by emotional isolation and a lack of psychological support. Although the patients felt physically cared for, many struggled to make sense of their experiences without spaces for dialogue or validation of their emotional needs. The abrupt ending of structured care left the patients in a liminal state as no longer ill but not yet whole, which amplified their fears of recurrence and uncertainty about the future. Although they were rare, moments of genuine emotional recognition were deeply valued and helped re-establish a sense of coherence and support.
Comments (0)