
Remember me
In this issue of Hepatology International, Wang et al. conducted a randomized, open-label, early-phase ‘proof of concept’ human clinical trial to establish early safety, tolerability, and non-inferiority (compared to HSA) of rHA produced in Pichia pastoris cultured in bioreactors, in patients with cirrhotic ascites who were randomly assigned to receive rHA or HSA at a dose of 10, 20, or 30 g/day [13]. Each group had 12 participants: 9 receiving rHA and 3 receiving HSA as positive control. Treatment continued for 14 days or until serum albumin levels reached 35 g/L, followed by a 28-day follow-up. The incidence of adverse events was similar between the rHA and HSA groups (44.4% vs. 44.4%).
The results demonstrate that rHA exhibits a safety profile comparable to plasma-derived human serum albumin (HSA). rHA was well tolerated and did not elicit detectable anti-drug antibodies. This observation is quite important as certain recombinant albumins—particularly those derived from rice and Pichia pastoris—have exhibited glycosylation patterns that may provoke immune responses. This includes non-enzymatic modifications of lysine and arginine residues. Notably, elevated antibody titers targeting the mannan component of Pichia pastoris have been detected in normal human serum, likely due to structural similarities with Candida albicans proteins that promote cross-reactivity. Further, there were distinct differences in glycosylation patterns: HSA exhibited a relatively high glycosylation frequency at serine 232 (17.4%–33.0%), whereas rHA displayed low-level mannosylation at serine 489, not exceeding 5.0%. The study participants were limited and there were differences in etiologies between groups, which could have impacted the outcome. It would have been helpful if the investigators had added data on the dynamic changes of albumin levels over time. The impact on short- and long-term coagulation parameters, mean arterial pressure, pulmonary, renal, neurological and endocrine functions across multiple centers—encompassing diverse ethnic groups and etiologies—need to be systematically evaluated in future trials. Interestingly, this isn’t the first instance of yeast-derived recombinant human serum albumin (rHSA) being evaluated for human use. As early as 2008, a product called Medway—an rHSA synthesized from Pichia pastoris—was approved in Japan for treating hypoalbuminemia. However, it was subsequently withdrawn following revelations of data falsification [14].
In another recent trial, the same group of investigators tried human albumin produced in rice plant (Oryza sativa) grains (OsrHSA)—the first rice-derived recombinant protein trial used for intravenously in humans [15]. This was a more comprehensive study where 220 patients (decompensated hepatic cirrhosis with ascites and a serum albumin level ≤ 30 g/L) received OsrHSA (n = 175) or HSA (n = 45). They found that rice-derived HSA is non-inferior to plasma-derived HSA in efficacy and safety. No clinically significant high titers of anti-host cell (rice) or anti-drug antibodies were found in patients. As far as production costs and scalability are concerned, rice-derived human albumin has an edge over yeast-derived because large-scale cultivation of rHSA-expressing rice can be achieved with lesser capital investment and cost of production. Paddy can be grown in open fields while growing yeast requires specialized bioreactors and sterile environment. The isolation of rHSA from rice grains is also technically simpler than from yeast. As a result, rice-derived rHSA presents a compelling opportunity for recombinant albumin manufacturing.
Future of albumin therapy: The neonatal Fc receptor (FcRn) protects albumin from lysosomal degradation by recycling it back into circulation. Engineering albumin to prolong its circulating half-life for example with increased affinity for FcRn (especially at acidic pH) showed prolonged half-life [16]. Addition of PASylation domains (Proline, Alanine, Serine repeats) can also prolong its half-life [17]. PAS sequence increases the hydrodynamic volume of the protein, which reduces renal clearance by slowing filtration through the kidneys, enhances stability in serum and avoids immunogenicity and organ accumulation seen with PEGylation.
An emerging therapeutic avenue involves albumin gene therapy, wherein appropriate human tissues—beyond the liver—could be genetically modified via viral or non-viral vectors to produce physiological levels of albumin. However, this approach remains highly challenging due to albumin’s high turnover and short functional half-life in cirrhosis. Moreover, our current understanding of the negative feedback mechanisms governing albumin homeostasis is still rudimentary, underscoring the need for further molecular and regulatory insights. Cirrhosis tissue environment is characterized by high oxidative stress. This can be solved by incorporating mutations that stabilize disulfide bonds, reduce oxidation-prone residues, or enhance domain–domain interactions that can improve resistance to degradation and prolong half-life.
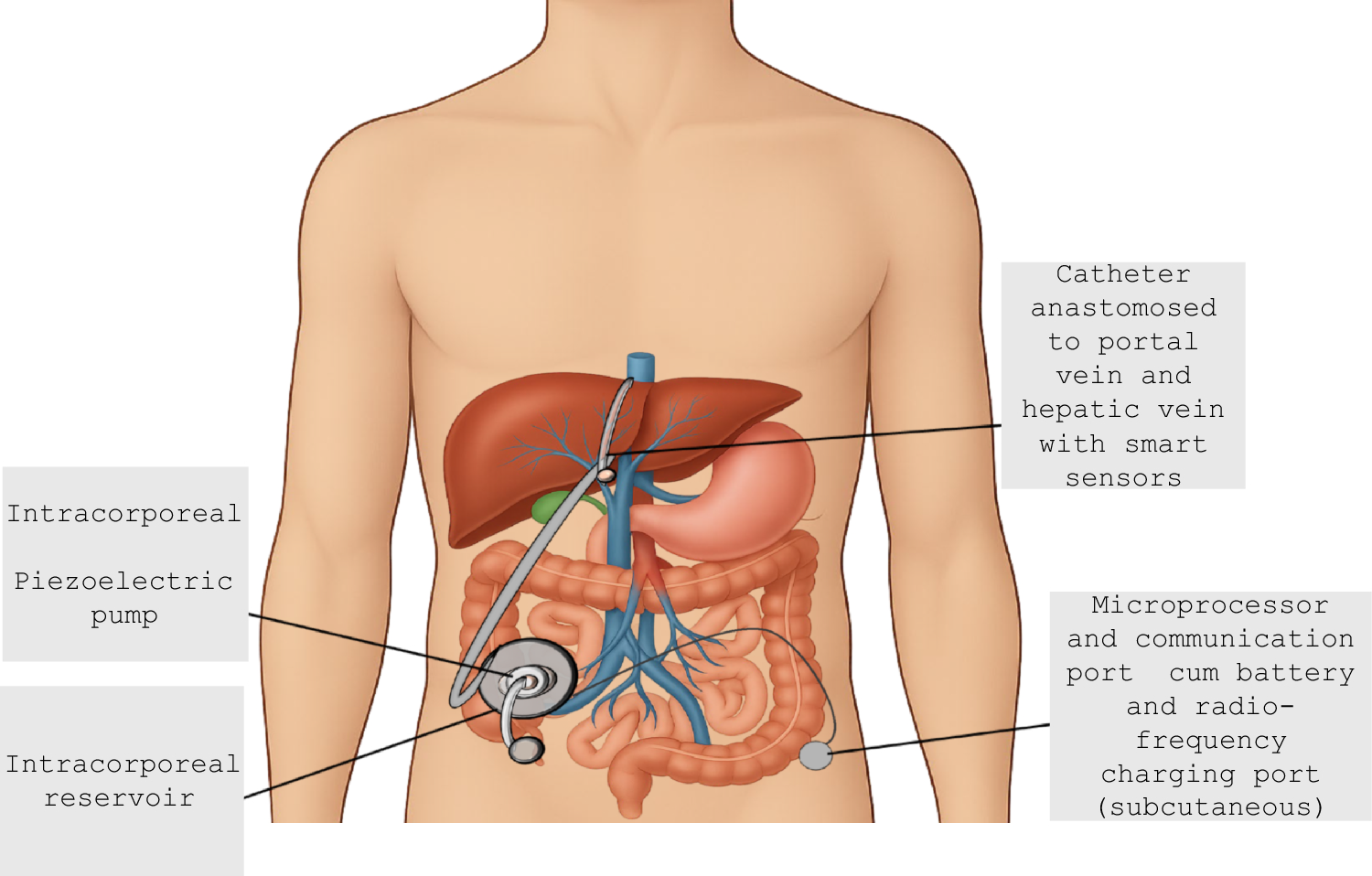
Albumin therapy beyond albumin: Liver produces several vital proteins besides albumin which are also depleted in cirrhosis. By conjugating these molecules to albumin, we might be able to improve their circulating half-life [16]. Supplementing regular albumin infusions with these albumin pre-conjugated therapeutic molecules (or other vital proteins) in optimal amounts could be the future. Weekly infusions are highly inconvenient and require hospitalization; besides being non-physiological. Portable or implantable ‘smart’ albumin infusion pumps could be a solution (Fig. 1). Technological precedents exist in the form of FDA-approved programmable protein/peptide infusion platforms [18]—for example, continuous subcutaneous insulin infusion devices for type 1 diabetes, subcutaneous immunoglobulin delivery systems for primary immunodeficiencies, and ambulatory infusion pumps for prostacyclin analogs, such as epoprostenol and treprostinil. The adaptation of these delivery paradigms to high-dose albumin administration represents a logical and potentially transformative step in the long-term management of cirrhosis. To conclude, next-gen albumin therapy together with advances in dialysis techniques and controlled nutrition could improve the survival of cirrhosis patients by decades!
Fig. 1
A conceptual smart albumin pump is implanted in the pelvic cavity, featuring a reservoir with a fill port for weekly replenishment of recombinant human serum albumin (rHSA). The outflow system includes two outlets: one directed to the portal vein and the other to the hepatic vein. The portal outlet can accommodate rHSA of slightly lower purity, leveraging hepatic clearance mechanisms, while the hepatic vein outlet delivers high-purity albumin directly into systemic circulation. Integrated smart sensors also monitor pressure differentials between the portal and hepatic veins, enabling dynamic regulation of portal pressure and ascites formation through controlled porto-systemic shunting
Comments (0)