
Remember me
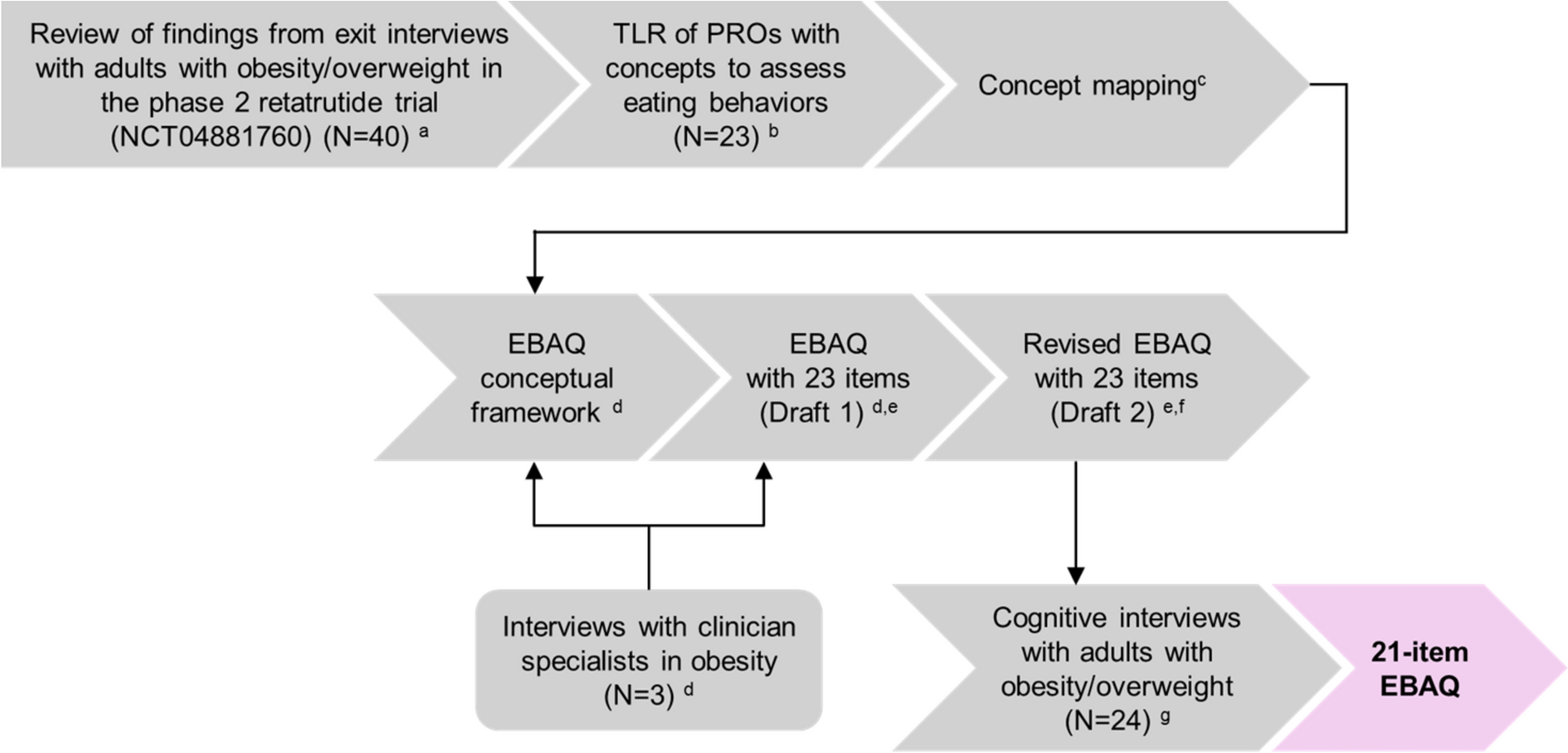
Forty adults (mean age 48.5 years) from the phase 2 trial of retatrutide versus placebo participated in the exit interviews [29]. The demographic and clinical characteristics of participants as well as the findings from the exit interview study have been reported previously [29]. Briefly, 19 appetite and eating behavior concepts emerged during the exit interviews, including concepts such as hunger and satiety, eating patterns (eating frequency, portion size), food choices and preferences, cognitive restraint or eating control, thoughts or sensations related to eating cravings, and emotional eating (Fig. S1).
Twenty-three PRO measures were identified in the TLR (Supplemental Appendix and Table S1) [30]. Appetite and eating behavior concepts (n = 19) that emerged during exit interviews with patients from the phase 2 trial of retatrutide were mapped against concepts in the 23 PRO measures identified in the TLR (Fig. S1) [29, 30]. Only a subset of concepts (≤ 10) identified in the exit interviews were captured by each existing PRO measure (Table S1 and Fig. S1). Eating behavior concepts that were underrepresented in the PRO measures identified in the TLR included concepts such as ‘eating between meals’ (1 of 23 PRO measures); ‘thoughts about food’ (3 of 23 PRO measures); as well as ‘feeling hungry less often’, ‘eating small portions’, and ‘eating less often’ (4 of 23 PRO measures). Further, none of the PRO measures identified in the TLR included concepts such as ‘satisfaction after eating’ and ‘duration of fullness’. The Three-Factor Eating Questionnaire captured the highest number of concepts (n = 10) identified in the exit interviews, followed by the Food Cravings Questionnaire, the Yale Food Addiction Scale, and the Adult Eating Behaviour Questionnaire (n = 8 for each). Thirteen eating behavior concepts were identified in the PRO measures that had not been explored in the exit interviews.
Clinician InterviewsClinician specialists in obesity (N = 3) confirmed the relevance of the eating behavior concepts included in the EBAQ (draft 1 with 23 items) (Table S2). All clinicians reported that hunger, satiety, and food preferences were key aspects of appetite and eating behavior that were likely to be impacted by treatment with OMMs. Nine out of 11 concepts included in draft 1 of the EBAQ were rated as “Important” or “Very important” by all the clinicians. The clinicians also suggested revisions to improve the content, clarity, and cohesion of concepts in the EBAQ, such as including the concept of ‘cravings’ under the ‘internal triggers’ domain and including ‘stress’ as a concept.
On the basis of findings from the translatability assessment, minor changes were made to the wording of the instructions and 14 of the items in the EBAQ.
Cognitive InterviewsParticipantsTwenty-four participants (mean age 46.3 years; BMI 38.4 kg/m2) completed the cognitive interviews to evaluate the EBAQ (draft 2 with 23 items) (Table 1). Most participants were female (n = 15, 63%) and most identified as not Hispanic or Latino (n = 15, 63%). Many participants were white (n = 10, 44%) and almost a third were Black/African American (n = 7, 30%).
Table 1 Sociodemographic and health characteristics of participantsParticipants reported having used exercise (n = 21, 91%), diet (n = 20, 87%), and medication (n = 9, 39%) to manage their weight in the past (Table 1). At the time of the interviews, more than two-thirds of the participants reported using diet (n = 16, 70%) and more than half reported using exercise (n = 14, 61%) to manage their weight. A third of the participants reported that they were receiving OMMs (n = 8, 33%). The most frequently reported obesity-related complications were hypertension (n = 9, 39%), anxiety (n = 7, 30%), and arthritis (n = 5, 22%) (Table S3).
Most participants (n = 23, 96%) reported being in good health, with high EQ-VAS and index scores (mean [standard deviation], 79.0 [13.3] and 0.9 [0.1], respectively) (Table S4). Participants (n = 23, 96%) reported craving-related eating behaviors as measured by the FCQ-T-r (mean score 36.1, range 18.0–64.0) (Table S5). Most participants selected the response option “Never” or “Rarely” for most FCQ-T-r items, suggesting that they did not experience or infrequently experienced craving-related behaviors.
Participants’ Appetite and Eating ExperienceAll 24 participants answered questions regarding their appetite and eating experiences. Most participants reported having two to three meals a day (n = 17) and eating snacks between or after meals (n = 17). Most participants (n = 20) reported experiencing cravings for specific foods (e.g., sweet or sugary foods or drinks, fried food). One-third of the participants (n = 9) stated that they found it difficult to control their eating habits.
Participants receiving OMMs (n = 8) mentioned having fewer cravings (n = 3), eating small portions (n = 2), being able to control their eating habits (n = 2), restraining themselves from eating when full (n = 1), and resisting eating between meals even when food was available (n = 1).
Overall Impression of the EBAQAll 24 participants provided positive feedback on the EBAQ (draft 2 with 23 items). Several participants (n = 10) made recommendations for improving the EBAQ. When asked about the EBAQ section considered most relevant to them, 11 participants selected ‘triggers’, 8 participants selected ‘eating control’, and 6 participants selected ‘appetite’.
InstructionsAll 24 participants reported that they could easily understand the instructions for completing the EBAQ (Table 2).
Table 2 Cognitive interview results for the EBAQ (N = 24)Recall PeriodAll 24 participants reported that they understood the recall period (‘past 7 days’) to mean the previous 7 days (“the past week”, “the previous 7 days from today”, “the last 7 days”, “from this day going back 7 days”) (Table 2). Most participants (n = 20) felt that the recall period of 7 days was appropriate and that they were able to remember the previous 7 days well enough to answer the questions in the EBAQ.
Response OptionsTwenty-three participants reported that the response options were clear to them, and that the options were appropriate (Table 2). Overall, participants used a good range of response options for the items in the EBAQ (Table S6). Only item 21 (‘Needing food for comfort’) showed a floor effect, with ≥ 25% of participants responding “Never”.
Domains and ItemsMost participants reported that the domain headers proposed for the ‘appetite’ (n = 24), ‘eating control’ (n = 24), and ‘triggers’ (n = 22) domains were appropriate, clear, and self-explanatory.
At least 79% (n ≥ 19) of the participants reported that each item in the ‘appetite’ domain was clear and easy to understand, and at least 88% of the participants (n ≥ 21) reported that each item was relevant to them (Table 2). Two out of five participants in round 1 of the cognitive interviews stated that they found item 7 (‘Choosing healthy foods’) and item 8 (‘Preferring healthy foods’) to be similar. Fifteen out of 19 participants in rounds 2 and 3 of the interviews also reported that they found items 7 and 8 to be similar. Participants who were asked (n = 21) reported that they considered item 8 (‘Preferring healthy foods’) (n = 8 of 21) and item 3 (‘Fullness after eating a small amount of food’) (n = 7 of 21) as the most important items in the ‘appetite’ domain.
Nineteen or more participants (≥ 79%) reported that each item in the ‘eating control’ domain was clear and easy to understand (Table 2). At least 75% of the participants (n ≥ 18) reported that each item included in the ‘eating control’ domain was relevant to them. Four participants did not demonstrate a clear understanding of item 10 (‘Appetite was controlled’), providing different interpretations of this item. Participants who were asked (n = 20) reported item 12 (‘Eating when not hungry’) (n = 8 of 20) and item 15 (‘Guilty after eating’) (n = 7 of 20) as the most important items in the ‘eating control’ domain.
Twenty-three or more participants (≥ 96%) reported that each item in the ‘triggers’ domain was clear and easy to understand (Table 2). Fifteen or more participants (≥ 65%) reported that each item in the ‘triggers’ domain was relevant to them. One participant out of five in round 1 of the cognitive interviews mentioned that drinking behavior was missing from the EBAQ. When asked if sugary drinks should be added to item 16 (‘Cravings for sweet or sugary foods’), 17 out of 19 participants in rounds 2 and 3 of the interviews stated that it would be appropriate to include sugary drinks in the item. Nine out of 19 participants in rounds 2 and 3 of the cognitive interviews reported that item 16 (‘Cravings for sweet or sugary foods’), item 17 (‘Cravings for fatty or fried foods’), and item 18 (‘Cravings for certain foods’) were similar, with some participants suggesting exclusion of item 18. Participants who were asked (n = 21) most frequently reported item 20 (‘Eating because of emotions’) (n = 14 of 21) and item 23 (‘Eating because stressed’) (n = 9 of 21) as the most important items in the ‘triggers’ domain.
Participants who received OMMs (N = 8) more frequently endorsed EBAQ items that were reflective of outcomes that could be beneficial for weight management (e.g., eating small amounts of food, high level of eating control) and less frequently endorsed items reflective of outcomes that could hinder weight management efforts (e.g., eating snacks between meals, eating in response to thoughts about food items, cravings for food) than participants who had not received OMMs (N = 16) (Table S6). Differences between the two participant groups were most marked for EBAQ items included ‘Fullness after eating a small amount of food’, ‘Quickly satisfied while eating’, ‘Eating small portions’, ‘In control of eating habits’, ‘Eating in response to thoughts about food’, ‘Thinking about eating’, and ‘Eating when bored’.
Summary of Revisions to the EBAQ Following Cognitive InterviewsDraft 2 of the EBAQ (23 items) was refined on the basis of findings from the cognitive interviews. Two items that were deemed similar to other items were removed from the EBAQ, resulting in a 21-item measure. The excluded items were item 7 (‘Choosing healthy foods’) as it was deemed redundant with item 8 (‘Preferring healthy foods’), and item 18 (‘Cravings for certain foods’) as it was deemed redundant with item 16 (‘Cravings for sweet or sugary foods’) and item 17 (‘Cravings for fatty or fried foods’). Item 11 (‘Avoid eating between meals even when food was available’) was revised to ‘Resist eating between meals even when food was available’, as participants preferred the description ‘resist eating’ over ‘avoid eating’ as it was easier to understand. Item 16 (‘Cravings for sweet or sugary foods’) was revised to ‘Cravings for sweet or sugary foods or drinks’, as several participants reported experiencing cravings for sugary drinks. The study team revised the header for the ‘triggers’ domain to ‘triggers for eating’ to ensure it was clear that the triggers were in relation to eating. Despite a few participants stating difficulty in understanding item 4 (‘Quickly satisfied while eating’), item 10 (‘Appetite was controlled’), or item 13 (‘Eating in response to thoughts about food’), no changes were made to these items as most participants understood the items and were able to select a response. Also, there were no clear suggestions from participants for better, alternative wording.
The revised version of the EBAQ included 21 items across three domains and evaluated eight appetite and eating behavior concepts relevant to obesity and treatment for obesity (Fig. 2).
Fig. 2
Conceptual framework for the 21-item Eating Behavior and Appetite Questionnaire (EBAQ). The EBAQ includes 21 items evaluating 8 appetite and appetite concepts associated with obesity or treatment for obesity. For each EBAQ item, there are five response options (0 = “never”, 1 = “rarely”, 2 = “sometimes”, 3 = “often”, and 4 = “always”). Participants are asked to choose one response per item that best describes how they felt in the previous 7 days. EBAQ Eating Behavior and Appetite Questionnaire
Comments (0)