Data Source
De-identified data from the Veterans Health Administration (VHA) Corporate Data Warehouse (CDW) between January 1, 2006 and December 31, 2023 were used. VHA CDW data comprise electronic records from the largest integrated healthcare system in the USA, with over 1300 care sites serving over nine million veterans and their dependents annually [16].
Ethics Approval
The study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.
Sample Selection
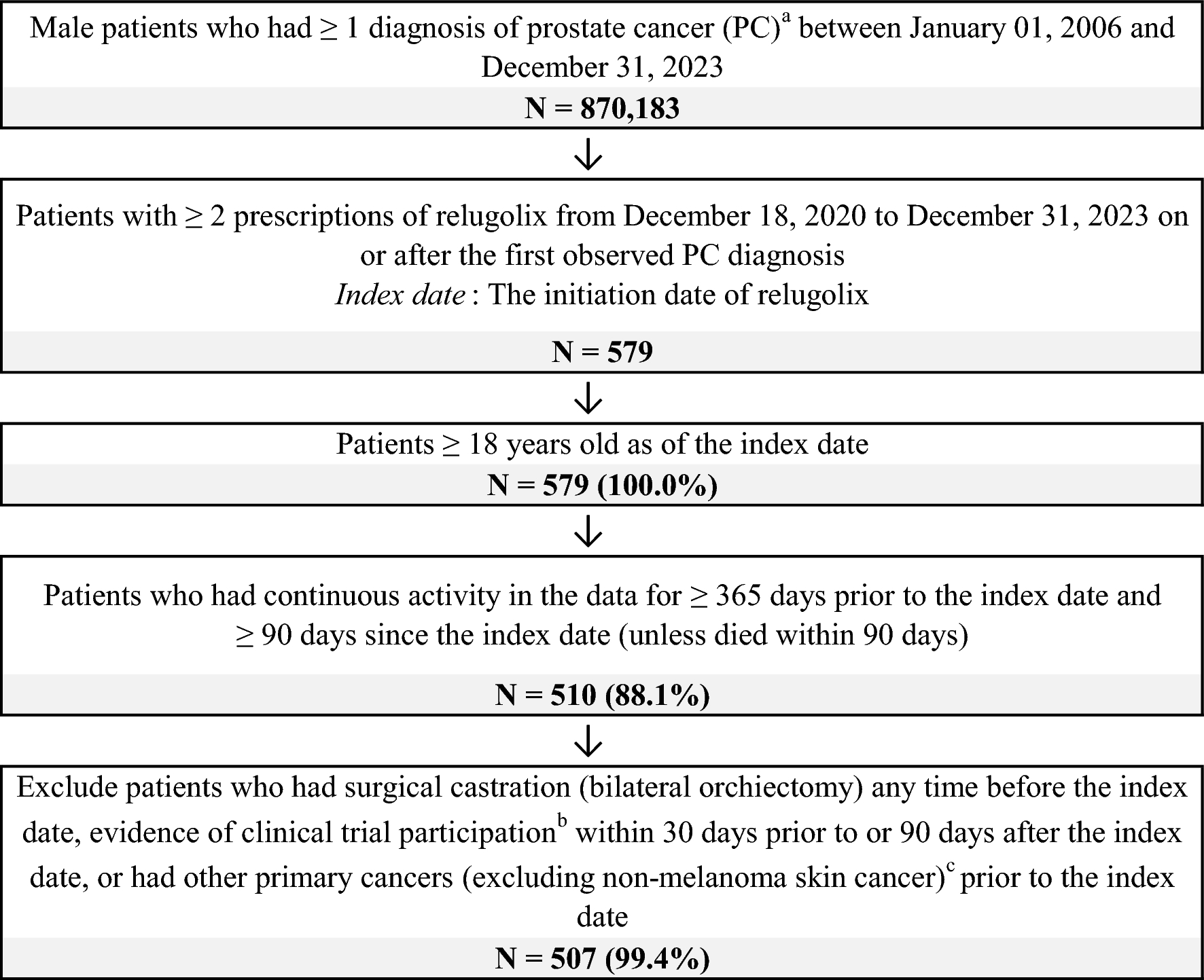
Male adults (≥ 18 years old) with ≥ 1 diagnosis of PC (International Classification of Diseases, 10th Revision, Clinical Modification code C61) who initiated relugolix were selected for the study. Patients were required to have ≥ 2 prescriptions of relugolix, and the initiation date of the first relugolix prescription (defined as the index date) was required to be on or after the first observed PC diagnosis and the relugolix approval date (i.e., December 18, 2020). Patients were also required to have continuous activity in the data for ≥ 365 days prior to the index date (i.e., the baseline period) and ≥ 90 days after the index date (unless they died within 90 days). Patients who had evidence of surgical castration (bilateral orchiectomy) any time before the index date, participated in a clinical trial within 30 days prior to the index date or within 90 days after the index date, or had other primary cancers (excluding non-melanoma skin cancer) prior to the index date were excluded from the study. The follow-up period spanned from the index date to the earliest of death, end of continuous eligibility, or end of data availability. Analyses included all patients meeting the eligibility criteria, with separate assessments and comparisons between Black and non-Hispanic White patients. Patients of other races (i.e., Hispanic, other, or unknown) were included in the overall sample but not in the race-stratified analyses because of the small sample sizes.
Study MeasuresBaseline Characteristics
Patient demographics, baseline disease characteristics, treatment history, and comorbidities (National Cancer Institute [NCI] Charlson Comorbidity Index [CCI] and relevant individual comorbidities) were described during the baseline period.
Treatment Patterns
Based on the systemic PC treatments received within 30 days before and 90 days after the index date, relugolix treatment patterns were categorized into relugolix monotherapy, relugolix + non-steroidal anti-androgen (NSAA) only, relugolix + androgen receptor pathway inhibitor (ARPI) ± NSAA, relugolix + chemotherapy ± NSAA, relugolix + ARPI + chemotherapy ± NSAA, and relugolix + other PC treatment. Discontinuation of relugolix, switching to a different ADT, and adding on a systemic PC treatment were assessed during the follow-up period. Discontinuation of relugolix was defined as a treatment gap of ≥ 90 days, the initiation of another ADT (i.e., degarelix, goserelin, histrelin, leuprolide, and triptorelin), or death during the follow-up period, whichever occurred first. Switching to a different ADT was defined as the initiation of an ADT different from relugolix during the follow-up period. Adding on a systemic PC treatment was defined as the initiation of an ARPI, NSAA, chemotherapy, immunotherapy, poly(ADP-ribose) polymerase (PARP) inhibitor, radiopharmaceutical therapy, or systemic ketoconazole 90 days after the index date while maintaining continuous relugolix use.
Adherence to relugolix, measured by medication processing ratio (MPR) and proportion of days covered (PDC; formulas and illustrated examples are provided in Supplemental Fig. S1), were assessed during the first 3, 6, 9, and 12 months following the index date for patients with continuous relugolix use during each specified time interval. MPR was calculated by dividing the total number of days of relugolix supply by the number of days in the respective time interval, without forward-shifting overlapping prescriptions. MPR was capped at 100% if the estimate exceeded 100%. PDC was calculated by dividing the total number of non-overlapping days covered by relugolix by the number of days in the respective time interval, with overlapping prescriptions shifted forward. PDC, by design, was ≤ 100%.
PSA Responses
PSA responses during relugolix treatment, defined as (1) ≥ 50% reduction in PSA from baseline, (2) ≥ 90% reduction in PSA from baseline, and (3) nadir PSA < 0.2 ng/mL, were assessed among ADT-naïve patients (i.e., no records of any systemic ADT prior to the index date). Baseline PSA measure was defined as the PSA measure closest to the index date within 180 days prior to the index date. Patients without a baseline PSA measure or a PSA measure during the period of continuous relugolix use were excluded from the PSA response analysis.
Statistical Analysis
All analyses were conducted in the overall sample and by race (i.e., Black and White patients). Means, standard deviations, medians, and interquartile ranges were estimated for continuous variables. Counts and percentages were estimated for categorical variables. Standardized mean differences (SMDs) were calculated for the unadjusted comparisons of baseline characteristics between Black and White patients. SMDs > 10% were considered statistically significant. A Kaplan–Meier analysis was conducted to describe time to treatment changes. Unadjusted and adjusted Cox proportional hazards regression models estimated the hazard ratios (HR) and corresponding 95% confidence intervals (CI) of treatment changes comparing Black and White patients. The adjusted variables were selected on the basis of clinical input, their prevalence in the data, and SMDs > 10% and included age at index, index year, region, baseline PSA, baseline testosterone, treatment history (i.e., pain medication, chronic oral corticosteroid, ADT), metastatic disease status, and baseline comorbidities (i.e., NCI CCI, hypertension, diabetes, major adverse cardiovascular events, depression, congestive heart failure, sexual dysfunction, cognitive impairment, and urinary tract infections). Unadjusted and adjusted generalized linear models were conducted to compare the adherence to relugolix between Black and White patients, accounting for the same variables used in the adjusted Cox proportional hazards regressions. Unadjusted comparisons of the proportions of patients achieving PSA response between Black and White patients were conducted using chi-squared tests (adjusted comparisons were not conducted because of the small sample sizes). All analyses were conducted using SAS software, version [9.4] (SAS Institute Inc., Cary, NC, USA).
Ethics Approval
The study was considered exempt from institutional review board (IRB) review and informed consent under 45 CFR § 46.104(d)(4), as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.

Comments (0)