This study demonstrated a strong correlation between fECV, calculated from 3-minute equilibrium phase PCD-CT images, and the mALBI grade, indicating its utility in assessing liver function. Furthermore, significant variations in fECV reflecting the mALBI grade were observed across different liver segments.
Previous studies using DECT have also shown a strong correlation between fECV and liver function or fibrosis stage [4,5,6,7,8,9]. The fECV represents both the extravascular extracellular space and the intravascular space. With fibrosis progression, collagen fiber synthesis expands the extravascular extracellular space. Since fibrosis primarily affects the extravascular compartment, increases in fECV associated with fibrosis are mainly driven by changes in this space. Normalization using hematocrit and aortic iodine density helps minimize the contribution of the intravascular space to the fECV calculation [5].
Prior research has indicated that fibrosis progression may be more pronounced in the medial segment (S4) of the left lobe and the anterior segments (S5, S8) of the right lobe compared to other segments [4]. Morphological changes associated with liver cirrhosis often involve atrophy of the right lobe (primarily S5–S8) and the medial segment (S4), accompanied by hypertrophy of the caudate lobe (S1) and the lateral segment (S2, S3) [22, 23]. As fibrosis progresses, it leads to an expansion of the extravascular extracellular space and a relative reduction of the intravascular space within the affected tissue. This suggests that fibrosis might progress earlier in regions prone to atrophy, leading to an earlier increase in fECV in these areas. To substantiate this hypothesis, future research is needed to quantitatively measure the volume of each segment and directly verify the correlation between the degree of atrophy and fECV values. Consistent with this hypothesis, our study found that in mALBI grade 2a, fECV was significantly higher in S4, S5, and S8 compared to other segments. In the more advanced mALBI grades 2b and 3, where fibrosis has likely progressed throughout the liver causing global functional decline, significant differences in fECV among segments were no longer observed. The lack of significant inter-segmental fECV differences in mALBI grades 2b and 3 is likely because fibrosis had progressed throughout the entire liver parenchyma, leading to a comprehensive decline in liver function that obscured the relative differences between segments. This suggests that fECV in specific segments may be a sensitive indicator for particular stages of liver function decline.
These findings highlight the importance of considering segmental variations in fECV relative to the mALBI grade. Notably, the fECV values of potentially atrophic areas—specifically the medial (S4) and anterior (S5, S8) segments—were significantly higher in mALBI grade 2a, demonstrating their usefulness in detecting early-stage liver function decline. ROC analysis further supported this, showing that S4, S5, and S8 yielded the highest AUCs (0.968, 0.948, and 0.932, respectively) for differentiating mALBI grade 1 from grade 2a or higher. This segmental pattern is also visually evident in representative cases, as shown in Fig. 6. In particular, the fECV map of the mALBI grade 2a patient (Fig. 6B) clearly demonstrates elevated values in the medial segment (S4), supporting the notion that early fibrosis-related functional decline may be regionally accentuated. These findings suggest that fECV in these regions may serve as sensitive biomarkers for early disease progression. In contrast, while the AUCs for the posterior segments (S6, S7) were relatively lower in early-stage prediction, only these segments exhibited statistically significant increases in fECV across all consecutive mALBI grades. This trend indicates that fECV in S6 and S7 may be better suited for evaluating the stepwise progression of hepatic functional impairment. However, we acknowledge that comprehensive stratification of liver disease severity may require whole-liver assessment, and further validation is needed to establish the prognostic value of segmental fECV. Taken together, our results imply that fECV provides complementary clinical value depending on the hepatic segment evaluated—serving both as an early detection tool (S4, S5, S8) and a staging marker for disease severity (S6, S7). The ability to examine fECV in each liver segment highlights an advantage of CT. Liver biopsy is limited to specific regions, and its invasiveness precludes multi-segment evaluation [24, 25]. Elastography techniques (ultrasound or MRI) are often restricted, primarily to the right lobe, due to technical challenges and artifact susceptibility, making comprehensive whole-liver assessment difficult [26, 27]. CT, however, offers advantages such as rapid acquisition, relative ease of performance, and reduced motion artifacts, enabling segmental fECV evaluation. It is important to position the clinical utility of segmental fECV not as a replacement for, but as a complement to established blood-based markers such as the mALBI grade. While mALBI provides a reliable and cost-effective measure of current liver function, fECV offers insight into the underlying structural pathology—namely fibrosis—that drives future, irreversible decline. Its potential lies in serving as an early predictive biomarker. Moreover, because contrast-enhanced CT is routinely performed for indications such as HCC surveillance, fECV can be calculated opportunistically without additional cost or radiation exposure. Unlike global blood tests, segmental fECV enables mapping of spatial heterogeneity, which may refine clinical decision-making—for example, by guiding biopsy to the most fibrotic regions or informing preoperative planning for hepatic resections and locoregional therapies.
Traditionally, fECV measurement required both non-contrast and equilibrium phase images, introducing potential misalignment issues; DECT largely resolved this problem [28, 29]. Conventional EID-based DECT systems utilize various approaches (dual-source, rapid kV-switching, dual-layer detectors) for spectral separation. However, these methods inherently involve significant overlap between the energy spectra, limiting the accuracy of energy discrimination [30]. PCD-CT, employing a single X-ray tube and a photon-counting detector, directly measures the energy of each incoming photon. This fundamentally different approach avoids energy spectra overlap. Consequently, PCD-CT offers improved energy discrimination performance compared to DECT, which is advantageous for accurate material decomposition, including iodine quantification [10,11,12]. A key practical advantage is that PCD-CT can acquire spectral data during routine scanning protocols, allowing retrospective spectral analysis whenever needed. Moreover, spectral analysis can be performed reliably even under high-speed or low-dose acquisition settings, which is especially advantageous for pediatric or critically ill patients.
Although studies on fECV measurement using PCD-CT are currently limited due to its recent clinical introduction, our study successfully performed detailed segmental fECV analysis using this technology. The correlation strength and stratification capability observed between PCD-CT-derived fECV and mALBI grade in our study were comparable to those reported in previous DECT studies [4]. While specific imaging parameters and equilibrium phase timing differed from prior research, the accuracy of hepatic iodine quantification in the equilibrium phase appears similar between DECT and PCD-CT. However, PCD-CT provides notable workflow benefits, facilitating straightforward fECV calculation within routine clinical practice. Additionally, the inherent lower noise characteristics of PCD-CT, particularly relevant at potentially lower doses used in clinical practice, likely contribute to the accurate calculation of fECV. While a prior study by Ozaki et al. demonstrated segmental fECV differences in chronic liver disease using 5-minute delayed DECT [4], our study expands this framework by incorporating PCD-CT with a shorter (3-minute) equilibrium phase. This approach not only reflects practical imaging work-flows but also enables retrospective spectral reconstruction, allowing flexible application without protocol modification. Moreover, by investigating the prognostic impact of segment-specific fECV on future mALBI grade deterioration, our study provides novel insight that was not addressed in previous DECT-based evaluations.
Our choice of a 3-minute delay for the equilibrium phase imaging warrants justification, as it is shorter than the 5 to 10-minute delay used in many other DECT-based fECV studies. Our rationale was threefold. First, our primary goal was to validate a protocol that aligns with our institution’s routine dynamic liver CT imaging, thereby maximizing the potential for direct clinical translation and future retrospective analyses. Second, while the optimal timing remains debated [4,5,6,7,8,9], key studies have reported no significant difference in the correlation with fibrosis grade between 3-minute and 5-minute or 10-minute images [7, 31], suggesting that a 3-minute delay is sufficient to achieve contrast equilibrium. Third, our own results internally validate this approach, as the fECV derived from 3-minute images showed a strong correlation with mALBI grade and excellent diagnostic performance. While our retrospective design did not allow for a direct comparison with later time points, these factors combined support that our 3-minute protocol is both practical and effective for routine clinical application.
The high diagnostic performance of segmental fECV, particularly in segments S4, S5, and S8, for detecting early-stage (mALBI grade 2a) liver function decline has several potential clinical implications. First, it could refine prognostication and surveillance strategies. Patients with elevated fECV in these specific segments, even with otherwise reassuring global liver function tests, could be identified as a higher-risk population. This would allow for a more personalized surveillance schedule, with more frequent follow-up including elastography or blood markers, to detect progression to cirrhosis or hepatocellular carcinoma earlier. Second, segmental fECV could aid in treatment stratification. It might help identify candidates who would benefit most from early initiation of antifibrotic therapies or more aggressive management of the underlying etiology. From a clinical workflow perspective, segmental fECV could be implemented as an opportunistic screening tool. Since many patients with chronic liver disease undergo abdominal CT for various reasons, a protocol including a 3-minute equilibrium phase could provide valuable functional information without requiring a separate examination. The results could be presented as a quantitative ‘fECV map,’ offering an intuitive visual assessment of hepatic heterogeneity that complements the standard anatomical report. However, these potential applications are currently speculative and require validation in future prospective studies to confirm their clinical utility and impact on patient outcomes.
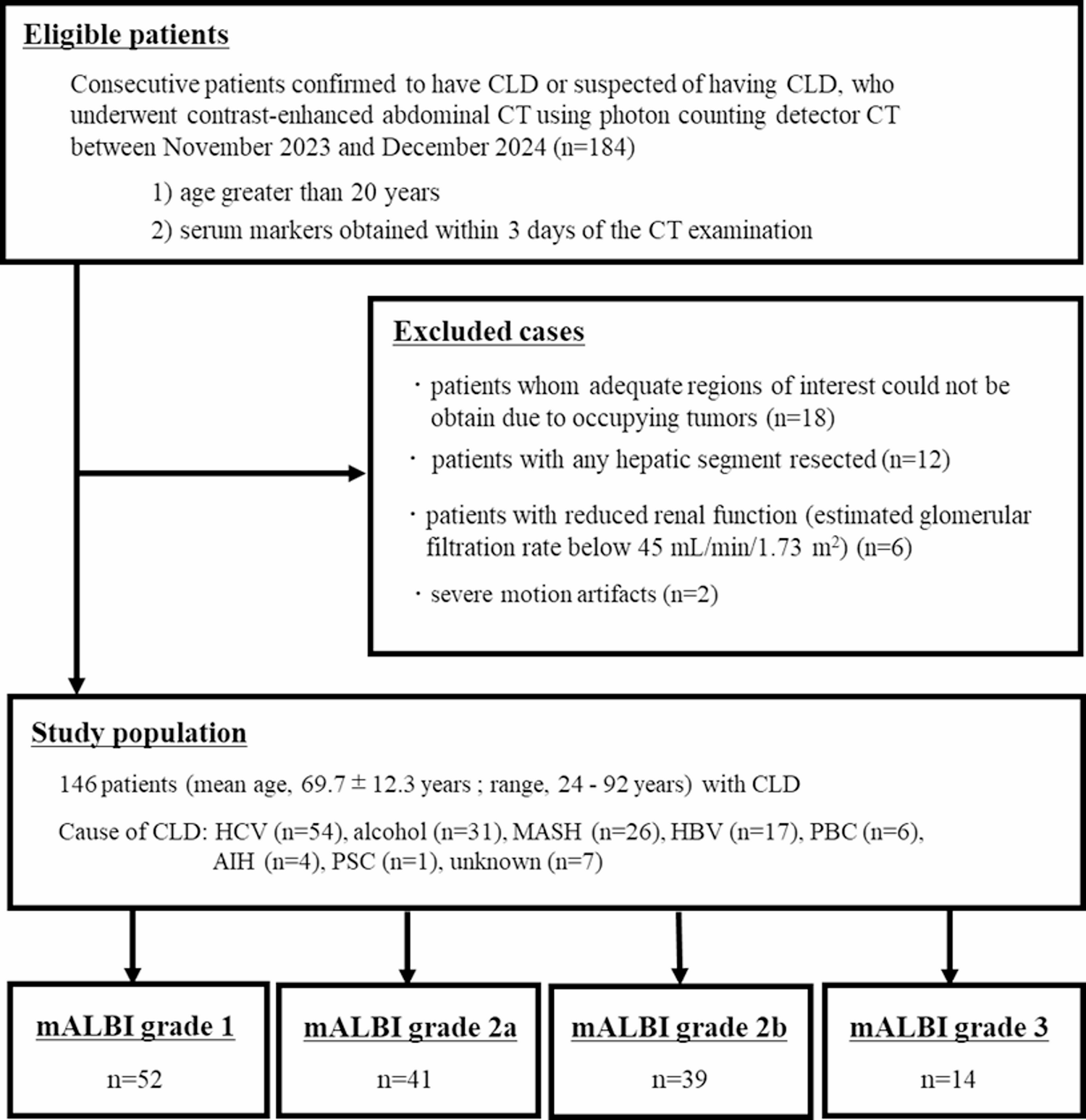
This study has several limitations. First, as a retrospective, single-center study, the generalizability of our findings is inherently limited. The results may be subject to selection bias and influenced by our institution’s specific patient demographics and clinical protocols. Furthermore, while the total cohort consisted of 146 patients, the subgroup of patients with the most severe liver impairment (mALBI grade 3) was small, with only 14 individuals. This limited sample size reduces the statistical power for this subgroup and may affect the robustness of our conclusions regarding advanced-stage liver disease. Therefore, our findings should be considered preliminary, and their validity needs to be confirmed by larger, multi-center prospective studies to ensure broader applicability. Second, we used the mALBI grade as the reference standard for liver function decline instead of liver biopsy, which is the gold standard for fibrosis assessment, consistent with some previous studies [4]. While liver biopsy is the gold standard for fibrosis assessment, our primary objective was to evaluate the utility of segmental fECV in predicting liver function, for which the mALBI grade is a well-validated and clinically relevant marker. This choice was also practical, reflecting clinical scenarios where an invasive procedure like biopsy is not always feasible, especially in a retrospective setting. Nonetheless, this represents a significant limitation. The fECV is believed to directly reflect the expansion of the extracellular matrix, which is a key histological feature of fibrosis. In contrast, the mALBI grade is a surrogate marker that primarily reflects liver function through albumin and bilirubin levels. Although liver function and the degree of fibrosis are closely related, they are not interchangeable. A discordance can exist where significant fibrosis is present with preserved liver function, or vice versa. Therefore, our findings demonstrate a correlation between segmental fECV and a functional score, but the direct relationship with the underlying histologic stage of fibrosis requires further investigation. Future prospective studies that include direct comparison with liver histology or other established non-invasive fibrosis markers, such as elastography, are necessary to validate the utility of segmental fECV in accurately staging fibrosis and predicting clinical outcomes. Furthermore, while a subset of our cohort had undergone liver biopsy, the significant temporal gap between the biopsy and the CT scan, along with non-standardized histological reporting, precluded a meaningful correlation analysis. A direct comparison with contemporaneous histological data remains a critical goal for future research. Third, this study has several limitations regarding potential confounding factors. Our study population was heterogeneous, including patients with chronic liver disease of various etiologies (e.g., viral, alcoholic, and metabolic). We did not perform a subgroup analysis based on etiology, as the number of patients in each category was insufficient for a statistically meaningful comparison. This heterogeneity is a significant limitation, as the underlying pathophysiology of fibrosis can differ between etiologies and may contribute to variability in fECV. Furthermore, we did not systematically account for other important confounders known to influence fECV values, such as hepatic steatosis, iron overload, active hepatitis, and ascites. These conditions can alter tissue density, vascular permeability, and contrast agent distribution, thereby affecting the accuracy of fECV measurements. For instance, severe steatosis may reduce the baseline attenuation of the liver parenchyma, while active inflammation could increase extracellular fluid. Due to the retrospective nature of our study, a systematic analysis of these factors was not feasible, and their potential influence on our findings cannot be excluded. Future prospective studies are therefore essential; they should incorporate these variables and utilize combined imaging techniques, biochemical markers, or histopathologic validation to better isolate the impact of each confounder and refine the diagnostic utility of segmental fECV. Fourth, fECV values were normalized to aortic iodine density, which may vary with cardiac output and systemic circulation. Although this method is widely used in previous studies [4,5,6,7,8,9] and offers practical reproducibility, it may introduce confounding. We did not perform a sensitivity analysis to evaluate the impact of circulatory variability. Future studies should consider alternative normalization strategies or include sensitivity analyses to further validate fECV robustness. A further limitation is that ROI placement for fECV measurement remains operator-dependent. Although we reported good to excellent interobserver agreement, intra-observer reproducibility was not assessed. This may affect the consistency of measurements, particularly in clinical settings. Future studies should evaluate intra-observer variability to further establish the reliability of segmental fECV quantification. Finally, it is important to frame this study as a proof of concept. While our findings are promising, they remain exploratory due to several limitations. As discussed, we did not systematically account for all potential confounders, and our reference standard—the mALBI grade—is a functional surrogate rather than a direct measure of fibrosis. Moreover, the optimal cut-off values derived from ROC analysis were not validated using external datasets, nor did we perform internal validation techniques such as cross-validation. These thresholds should therefore be considered hypothesis-generating. To substantiate the clinical utility of segmental fECV, future prospective studies are needed. Such studies should include larger and more diverse patient populations, incorporate established non-invasive fibrosis markers such as MR elastography, and evaluate clinical outcomes to comprehensively validate this approach.

Comments (0)