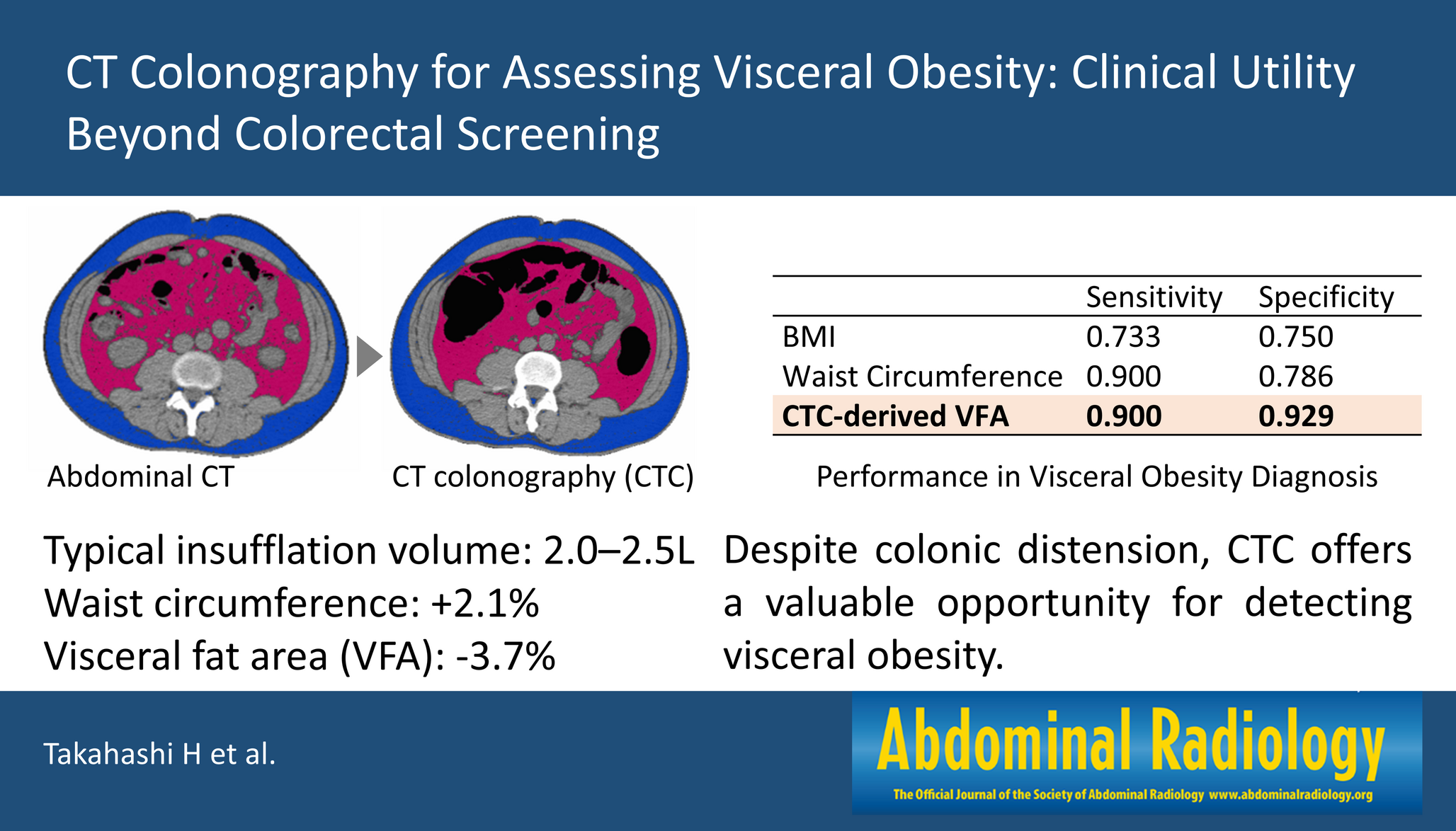
To our knowledge, this study is among the earliest to systematically evaluate the potential value of CTC vs. CT in assessing the visceral fat area. Despite the observed increase in waist circumference on CTC compared to CT, the VFA at the umbilical level was significantly lower on CTC (Table 2). This discrepancy may be attributed to colonic distension and compression of visceral fat caused by colonic insufflation. Bland–Altman analysis demonstrated good overall agreement between the CT-VFA and CTC-VFA, with 94.8% of patients within the limits of agreement (Fig. 2). Although a slight proportional bias and a few outliers were noted, their clinical impact appeared limited. In addition, correlation analyses showed that the CTC-VFA had the strongest association with the CT-VFA (r = 0.93, ρ = 0.94), further supporting its reliability. Overall, the CTC-VFA exhibited better predictive accuracy for visceral obesity than BMI and waist circumference (Fig. 3). This finding underscores the limitations of using BMI and waist circumference as markers, as they are influenced by factors such as muscle mass and subcutaneous fat, whereas CTC-VFA provides a more direct assessment of intra-abdominal fat [7, 13, 14]. Moreover, the incorporation of multiple slices further improved the diagnostic performance, suggesting that a multi-slice approach may enhance the robustness of CTC-VFA for visceral obesity assessment (Table 5).
Visceral obesity is increasingly recognized as an important health concern because of its strong association with a wide range of metabolic and cardiovascular disorders, including metabolic syndrome, hypertension, type 2 diabetes, dyslipidemia, and coronary artery disease [1, 3, 6]. In contrast to subcutaneous adipose tissue, which primarily serves as an energy storage depot, visceral adipose tissue (VAT) is now recognized not only as an energy depot but also as a metabolically and immunologically active organ. It contributes to systemic insulin resistance through the secretion of proinflammatory cytokines (e.g., TNF-α and IL-6), the disruption of insulin signaling pathways, and the excessive release of free fatty acids that promote hepatic gluconeogenesis and atherogenic lipoprotein production. VAT also exacerbates hypertension by activating the sympathetic nervous system and the renin–angiotensin–aldosterone system, leading to vasoconstriction and sodium retention [4, 6]. Moreover, emerging evidence links visceral fat to the development of certain malignancies, such as colorectal and breast cancers [5, 7]. These multifactorial mechanisms suggest that VAT plays a key role in cardiometabolic pathology and underscore the clinical importance of accurately identifying visceral obesity.
We observed cases where patients with similar BMIs or waist circumferences presented markedly different fat distributions, with some demonstrating greater subcutaneous fat accumulation and others more pronounced visceral fat accumulation (Fig. 1b). From a clinical risk perspective, distinguishing between these fat compartments is essential [3, 4]. Direct measurement of the visceral fat area using conventional CT provides a more accurate assessment of intra-abdominal fat, thus enabling better risk stratification and targeted intervention. As shown in Fig. 3, CTC-VFA outperformed both BMI and waist circumference in terms of classifying visceral obesity across all diagnostic metrics. Although the sensitivity of CTC-VFA was comparable to that of waist circumference (both 0.90), the specificity of CTC-VFA was substantially greater (0.93 vs. 0.79), so this metric may help better distinguish individuals with predominantly subcutaneous fat.
The primary strength of this study lies in its direct comparison of VFA measurements obtained from both CT and CTC in the same patients, performed within a short interval. This design minimizes interpatient and temporal variability, allowing for a more precise assessment of CTC-specific procedural effects, which remain insufficiently investigated to date. CTC is a minimally invasive imaging modality that is primarily used for detecting colorectal polyps and cancers without the need for endoscopic insertion, thereby reducing patient burden [16,17,18,19,20, 24, 25]. In addition to evaluating the colon, CTC provides comprehensive abdominal imaging, allowing for the incidental detection of extracolonic findings. In previous studies, this characteristic has been leveraged in previous studies to assess solid organ diseases such as liver lesions, renal masses, and pancreatic abnormalities [18, 26, 27]. However, CTC differs from conventional CT in several procedural aspects, including colonic preparation with laxatives, oral contrast agents, and colonic insufflation [21, 23].
A procedural factor anticipated to influence visceral fat measurement is the use of CO₂ insufflation to distend the colon during imaging. In this study, the median insufflation volume was 2.3 L (IQR: 2.0–2.8), which is consistent with previously reported ranges of approximately 2.0–2.5 L [21, 22]. While there was a tendency for males to have higher insufflation volumes, the difference was not statistically significant. Unlike solid organs, adipose tissue is more susceptible to compression, potentially leading to underestimation of the VFA. Indeed, while waist circumference slightly increased during CTC, VFA decreased, suggesting that colonic distension may compress intra-abdominal fat, resulting in lower measured values (Fig. 1c). CTC yielded a 3.7% lower median VFA, resulting in three false negatives, with a limited impact on health risk but affecting CT-based classification (Table 2; Fig. 3c).
The umbilical level remains relatively stable despite respiratory variation and colonic insufflation. When performing assessments at the vertebral level, the umbilical slice was most frequently positioned at L4–L5 (62.1% on CT and 60.3% on CTC), with 84.5% of the cases showing no shift in the vertebral level between the protocols (Table 3). In contrast, upward shifts of approximately one vertebral level were observed in the liver, right kidney, and left kidney. Previous studies have reported respiratory-induced shifts of 1.0–1.3 cm for the liver and right kidney (Table 4), and 0.9–1.0 cm for the left kidney [28, 29]. As CTC is typically performed during deep expiration, the displacement observed may exceed that reported in prior studies. The extent of the shift suggests a contributing effect of colonic insufflation. The liver exhibited greater movement than did the retroperitoneal kidney, indicating that non-retroperitoneal organs may be more sensitive to pressure changes. While the lower poles of these organs were generally located above L4, thus minimizing their impact on measurements at the umbilical level, substantial organ overlap could influence fat area assessment.
Despite the imaging variations associated with colonic distension and positional shifts, CTC has demonstrated potential utility in assessing visceral obesity. Compared with conventional metrics such as BMI and waist circumference, VFA measured at the umbilical level via CTC had greater predictive accuracy for visceral obesity (Fig. 3). This finding suggests that when CTC is performed, incorporating the VFA measurement as an additional health indicator could provide valuable clinical information [30], particularly because it reflects intra-abdominal fat more directly than anthropometric indices. A large multi-institutional survey in Japan reported that 147,439 CTC examinations have been conducted across 431 institutions, indicating that CTC remains concentrated in several dedicated institutions [25]. This limited dissemination likely reflects a lack of awareness among clinicians and a shortage of trained specialists; however, according to prior studies, patient acceptability of this technique is high, owing to its low invasiveness, proven safety, and established diagnostic accuracy [31,32,33]. Expanding secondary applications, such as the assessment of visceral obesity as shown in this study, could further enhance the clinical utility of CTC and help promote its broader adoption, particularly among individuals reluctant to undergo colonoscopy.
Moreover, incorporating multiple slices suggested potential improvements in the predictive performance of CTC measurements in estimating CT VFA, serving as the reference standard. The multivariable regression model incorporating both the umbilical and L2 levels achieved the best predictive performance, significantly reducing the MAE from 19.76 to 16.54 cm² (P = 0.013) and improving the RMSE and R² compared with the baseline model using only the umbilical level (Table 5). The addition of the L2 slice, which was positioned superior to the umbilical level, likely provided richer information regarding visceral fat distribution, contributing to more robust predictions. Notably, previous studies have identified L2–L3 as anatomically stable landmarks for body composition analysis [34], possibly because of the presence of retroperitoneal structures such as perirenal fat, which are less susceptible to deformation from colonic insufflation. The observed improvement may therefore reflect the benefit of including slices less affected by procedural variation. Further investigations are warranted to develop predictive models that effectively account for imaging variability in CTC. In addition, future work should explore the optimization of cutoff thresholds, the integration of CTC protocol-related parameters, and the potential value of volumetric or multi-slice approaches to further improve diagnostic accuracy.
This study has several limitations. First, this was a single-center retrospective study with a limited sample size, and external validation is necessary to confirm the generalizability of the findings. Second, all CT image acquisition and analysis were performed using a single scanner and specific postprocessing software. While this approach ensures consistency within the study, it may limit reproducibility across different equipment or analytical platforms. Third, the diagnostic criteria for visceral obesity were based on Japanese standards [15], which may not be directly applicable to other populations [35]. Finally, although the umbilical level was chosen for its anatomical relevance and ease of identification, other studies have used different vertebral landmarks or volumetric analyses for fat assessment [7, 34, 36,37,38]. Further research is needed to establish the optimal measurement approach across diverse populations and imaging protocols after considering procedural factors such as colonic insufflation conditions.
In conclusion, this study suggests that the CTC-VFA is a useful marker for identifying visceral obesity, enabling opportunistic assessment without additional radiation exposure or cost. Given that CTC is already performed for colorectal screening, incorporating VFA assessment into routine interpretation could enhance its clinical utility, particularly in health checkups and preoperative risk assessment. This approach could also support metabolic risk evaluation in appropriate patient populations.

Comments (0)