
Remember me
Thyroid gland tumors are the most prevalent endocrine neoplasms. Among them, the uncommon oncocytic (Hürthle Cell) neoplasm is a distinct subtype of epithelial follicular cell-derived neoplasms, first designated in the World Health Organization (WHO) Classification of Tumors in 2017. The name “Hürthle cell” was removed in 2022, correcting the misnomer (since Hürthle described parafollicular cells or C-cells).[1] Before these updates, oncocytic neoplasms (ONs) were considered a subtype of follicular neoplasms (FNs) and were managed as such. Due to a better understanding of the distinct molecular prolife and clinical behavior of ONs, they are now recognized as a distinct entity. Specifically, the WHO Classification of Tumors denotes two oncocytic thyroid neoplasms: Oncocytic adenoma (OA) and oncocytic carcinoma (OC). Diagnosis requires the presence of >75% oncocytic follicular cells,[2] and OCs represent approximately 2% of all thyroid cancers.[3] Notably, oncocytic cells can exist in other types of reactive or neoplastic processes: Lymphocytic (Hashimoto’s) thyroiditis, multinodular goiter, and malignancies, including papillary, medullary, or poorly differentiated thyroid carcinoma, and metastatic oncocytic malignancies of non-thyroid origin. Ultrasonography is the current standard initial imaging modality for presurgical evaluation of ONs.[1] In advanced disease presentation, with extrathyroidal extension or lymph node metastasis, seen in about 13% of cases,[4] computed tomography or positron emission tomography is used.[5,6] When confined to the thyroid, OCs typically appear hypoechoic and larger than their benign counterparts on ultrasound.[7,8] The subsequent fine-needle aspiration biopsy (FNAB) study, ONs consists exclusively of (or almost exclusively of) oncocytes appearing in isolated cells, sheets, or crowded clusters. The cells exhibit abundant finely granular cytoplasm, revealing ample mitochondria, with enlarged centrally or eccentrically located nuclei and prominent nucleoli. FNAB can only delineate a probable ON with low specificity, and it is impossible to distinguish between OA and OC based on FNAB alone.[9,10] The definitive diagnostic criterion for OC requires evidence of capsular, lymphatic, or vascular invasion. However, FNAB cannot provide this level of specificity. Oncocytic papillary thyroid carcinoma (OPTC) is a subtype of papillary thyroid carcinoma (PTC) composed of oncocytic cells with nuclear features of PTC (nuclear enlargement, elongation, overlapping, chromatin clearing, nuclear grooves, and intranuclear pseudoinclusions). From a molecular basis, ONs have mitochondrial deoxyribonucleic acid (DNA)[11] or the related GRIM19 gene alterations[12] and chromosomal gains and losses, not commonly seen in other tumors.[2,13] A third of these neoplasms show gene copy-number variations.[2,14] These new insights into the molecular profiles of these neoplasms, which do not always correspond to morphology, aid in the identification of ONs.[15-17] However, they remain challenging to diagnose preoperatively, particularly in the early stage of the disease,[17] and it is also impossible to distinguish malignant ONs from benign.[13,16] Therefore, definitive diagnosis currently requires surgical excision. The pre-operative diagnostic challenges restrict surgical planning,[17] with only approximately 10% of nodules that are preoperatively suggestive of oncocytic neoplasm being OCs.[18,19] Overall, the rarity of ONs and their recent identification as a distinct subtype of follicular thyroid carcinoma have led to a lack of data and knowledge about this neoplasm.[17]
Limited previous studies have concluded that OAs and OCs, in general, display similar molecular profiles, with differences only seen between a highly invasive subgroup of carcinomas and benign adenomas.[13,14] This study aims to reexamine these statements in light of advancements in molecular technologies utilizing commercial assays, including Afirma, ThyroSeq, and ThyGeNEXT/ThyraMIR. We respectively investigate the cytological patterns and genetic alterations in the diagnosis of malignant and benign ONs of the thyroid.
MATERIAL AND METHODS Sample identification and classificationWe queried Cooper University Hospital’s electronic pathology program SoftPath to identify all ONs collected during the period of January 2018 through March 2025. We used the terms “Hürthle,” “oncocytic,” and “thyroid” to identify relevant cases. Most specifically, in the “Query” function on SoftPath, we input the date range and the above three search terms to obtain a list of potential cases. We then went through all populated cases and excluded any that were not actually ONs. All samples of ONs were included in the study. The classification of ON or non-ON was based on the diagnosis recorded in the final resection pathology report. Utilizing SoftPath and our Electronic Medical Record (EMR) system, Epic, we identified which cases had cytological studies performed. We categorized these samples into specific diagnostic groups. The classification of the ONs was also based upon the diagnosis recorded in the final pathology report from the resection. These diagnoses were solely based on pathological findings. The benign group included ON, and the malignant group included OC and OPTC. We also included an in-between group consisting of oncocytic noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP).
Statistical analysisThe data, including tumor diagnosis, general patient demographics (sex and age), tumor characteristics (tumor size), cytological results, and molecular results, were recorded. JMP Pro 18.0.2 Student Edition (JMP Statistical Discovery LLC; Cary, North Carolina) was used to perform all statistical tests. Wilcoxon Rank Sum testing was used to identify any statistically significant differences between benign and malignant groups regarding patient age and tumor size. Logistic regression was used to assess the effect of age and tumor size on tumor identity (benign vs. malignant). A two-tailed Fisher exact test was used to identify any significant difference in cytology classifications, number of molecularly negative samples, and patient gender between benign and malignant groups.
Molecular studiesFor our molecular studies, three commercial molecular assays: Afirma, ThyroSeq, and ThyGeNEXT/ThyraMIR were employed. The results from these assays obtained through the EMR system were reported as benign or suspicious/positive based on their own criteria. Genetic alterations were recorded if reported. We then retrospectively compared the molecular and cytological study results across the diagnostic groups to identify any patterns.
RESULTS Patient demographics and pathology diagnosisWe identified a total of 119 surgical resection cases: 55 were classified as malignant, 62 as benign, and two as NIFTP. Sixty-five of these samples underwent cytological testing. Twenty-eight of these were malignant cases, with 17 being OPTCs and 11 being OCs. One of these samples was NIFTP. The remaining 36 samples were benign cases (OAs).
The patient’s demographics and tumor sizes are shown in Table 1. A statistically significant difference between the malignant and benign cytology groups in regard to patient age is seen, with older patients being more likely to have benign neoplasms (P = 0.0300). There is no statistically significant difference between the malignant and benign groups regarding patients’ sex or tumor size.
Table 1: Patients’ demographics and tumor size (65/119, cytology/resection).
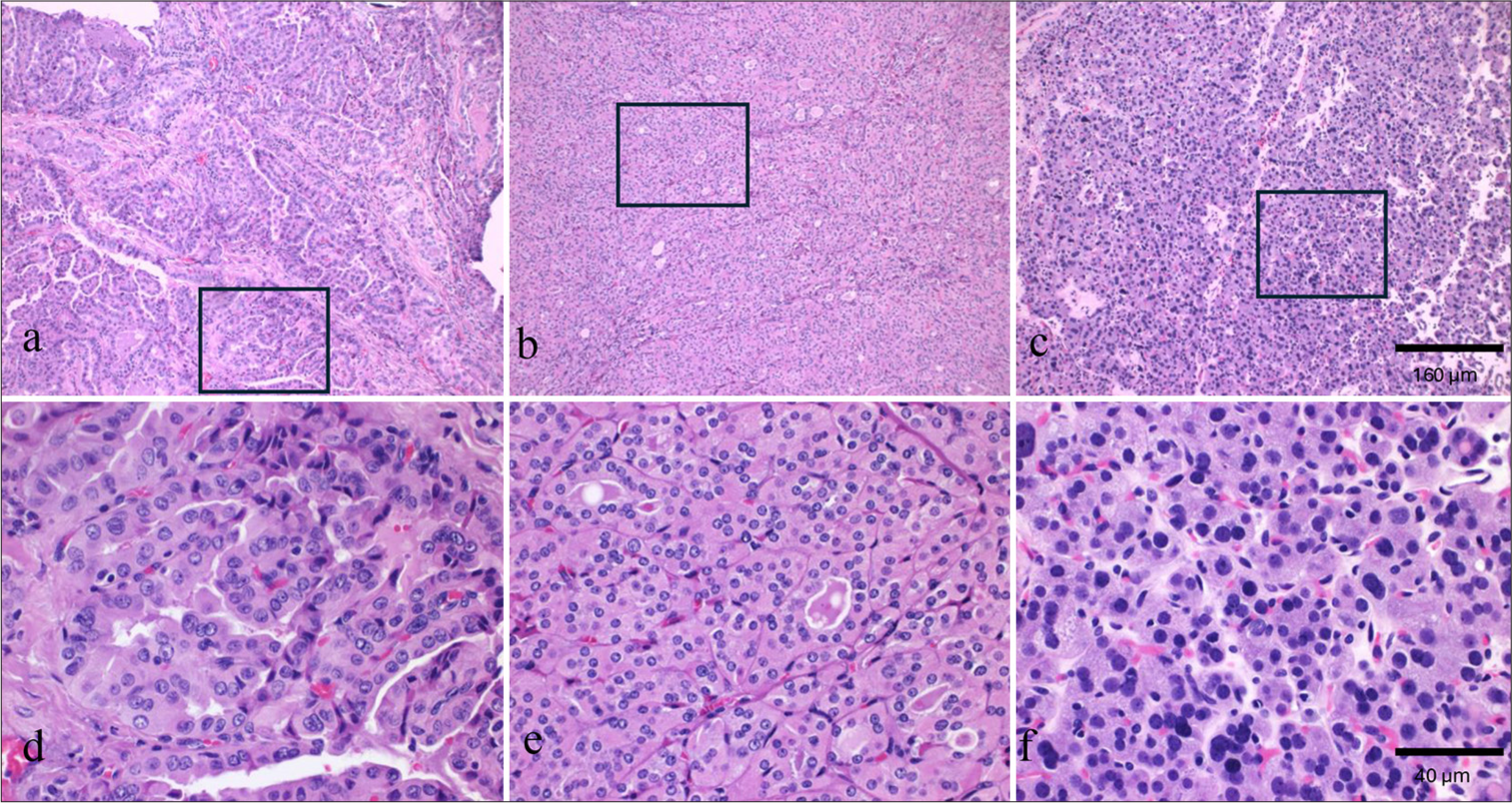
Malignant (28) NIFTP (1) Benign (36) P-valuesa Total malignant OPTC (17/28) OC (11/28) NIFTP OA (36) Malignant versus Benign Gender % (Female/total) 35.4 (23/65) 20.0 (13/65) 15.4 (10/65) 0 44.6 (29/65) P=1.000b % (Male/total) 7.7 (5/65) 6.2 (4/65) 1.5 (1/65) 1.5 (1/65) 10.8 (7/65) % (Female/total female) 44.2 (23/52) 25.0 (13/52) 19.2 (10/52) 0 55.8 (29/52) % (Male/total male) 38.5 (5/13) 30.8 (4/13) 7.7 (1/13) 7.7 (1/13) 53.8 (7/13) Age (years) Mean (range) 49.9 (24–78) 48.1 (24–78) 52.6 (24–75) 61 57.0 (21–80) P=0.0300c Tumor size (cm) Mean (range) 2.8 (0.8-7) 3.0 (0.8–7) 2.6 (0.9–4.6) 4.2 2.7 (0.5–7.5) P=0.9051c Cytological diagnosis and molecular findingsCytology FNAB of 65 cases diagnosed using the Bethesda category system, as summarized in Table 2. A higher percentage of Category III patients (63.9%) is observed among OA patients compared to Category IV patients (33.3%), but this difference is not statistically significant (P = 0.7889) (Prob[Bethesda = FN] is different across Tumor Identities). Regarding molecular testing, results are summarized in Table 3 and Figure 1. Representative tumor images are shown in Figure 2. About 3.6% (1/28) of the malignant samples were negative. Dividing it further, none of OPTCs were negative, and 9.1% (1/11) of OCs were negative. Focusing on OPTCs, 17.6% (3/17) were Afirma suspicious without any identified mutations. About 41.2% (7/11) of the OPTCs displayed Harvey rat sarcoma viral oncogene homolog (HRAS) Q61R mutations, 11.8% (2/17) had neuroblastoma RAS viral oncogene homolog (NRAS) Q61R mutations, 11.8% (2/17) had paired box 8 — peroxisome proliferator activator receptor gamma(PAX8-PPARG), 5.9% (1/17) had B-Raf proto-oncogene, serine/threonine kinase (BRAF) V600E mutations, 5.9% (1/17) had Kirsten rat sarcoma viral oncogene homolog (KRAS) p.G13R mutations, and 5.9% (1/17) had anaplastic lymphoma kinase/echinoderm microtubule-associated protein-like 4 (ALK/EML4) fusions. About 11.8% (2/17) of these samples had concurrent multiple chromosomal copy number alterations (CNAs). The OCs consisted of 36.4% (4/11) Afirma suspicious, 9.1% (1/11) ThyGeNEXT/ThyraMIR positive, and 9.1% (1/11) ThyroSeq negative. About 27.3% (3/11) displayed eukaryotic translation initiation factor 1A X-linked (EIF1AX) p.A113_splice mutations, and 18.1% (2/11) displayed multiple chromosomal CNAs (ThyroSeq). Of the benign (OAs) samples, 33.3% (12/36) were negative. The statistical difference in percentage of positive versus negative samples between the benign and malignant groups was P = 0.0035 (Prob[Sample = Negative] is different across Tumor Identities). About 22.2% (8/36) were Afirma suspicious, 22.2% (8/36) were Afirma negative, 8.3% (3/36) were ThyroSeq negative, 2.8% (1/36) were ThyGeNEXT/ThyraMIR positive, and 2.8% (1/36) were ThyGeNEXT/ThyraMIR negative. One-third (12/36) of the OAs had multiple chromosomal CNAs (ThyroSeq), two of these also showed telomerase reverse transcriptase (TERT) p.C288T, and one with thyroid stimulating hormone receptor (TSHR) p.D633E mutations. About 8.3% (3/36) had NRAS mutations, two being p.Q61R, and one being p.G13R mutations. The NIFTP displayed a HRAS p.G13R mutation.
Table 2: Histology, cytology, and molecular findings of thyroid oncocytic neoplasm.
Histology (n) Malignant Benign P-valuea OPTC (17) OC (11) NIFTP (1) OA (36) Cytology (%) Bethesda Category III 8 (47.1) 6 (55.5) 1 (100) 23 (63.9) P=0.7889 Bethesda Category IV 8 (47.1) 5 (45.5) 0 12 (33.3) Bethesda Category V 1 (5.9) 1 (2.8)Table 3: Molecular findings of thyroid oncocytic neoplasm.
Histology (n) Malignant Benign OPTC (17) OC (11) NIFTP (1) OA (36) Molecular positives (n; %) HRAS p.Q6IR
Export to PPT
Export to PPT
DISCUSSIONProgress in the genetics of thyroid tumorigenesis has enabled the development of molecular tests that enhance cytological diagnoses and refine the risk-based stratification of indeterminate thyroid nodules. Three common molecular testing platforms include those developed by Afirma (Veracyte Inc., San Francisco, CA, USA), ThyroSeq® Genomic Classifier (GC) (Sonic Healthcare, Rye Brook, NY, USA), and ThyGeNEXT® + ThyraMIR (Interpace Diagnostics, Parsippany, NJ, USA), all of which are often considered effective rule-out tests due to their high negative predictive value. Utilizing these genetic tests can aid clinicians and surgeons in stratifying patient risk and planning effective management. Afirma improved Gene Sequencing Classifier (GSC) uses next-generation ribonucleic acid (RNA) sequencing and whole exome sequencing combined with machine learning algorithms to create classifiers that provide clinically meaningful diagnostic and prognostic information. Each sample is sequenced no <10,196 genes, providing data on gene and exon expression, mitochondrial expression, loss of heterozygosity, and detection of expressed gene variants and fusions. Among OA or OC reported in the articles, the final GSC sensitivity was 88.9% and the specificity was only 58.8%, however.[20] Interpace Diagnostics employs the ThyGeNEXT genotyping panel alongside the ThyGeNEXT/ThyraMIR molecular test, which uses a microRNA-based assay. Samples are initially assessed with ThyGeNEXT, and if no strong/driver mutation is identified, they are further evaluated with ThyGeNEXT/ThyraMIR. Mutation panel false-positive results occurred in a 33% (11/33) of oncocytic cell adenomas, and 75% (6/8) of oncocytic cell carcinomas had positive mutation panel results.[21] ThyroSeq v3 GC, the most recent and advanced version of ThyroSeq testing, uses next-generation sequencing technology to analyze 112 genes, providing information regarding >12,000 mutation hotspots and >120 fusion types. It detects mutations (single-nucleotide variants), insertions and deletions, gene fusions, gene expression alterations, and CNAs. Using ThyroSeq v3 GC, 46.7% of OA yields a negative test result. About 92.9% of OCs were correctly detected.[22]
To the best of our knowledge, this is the only recent study that compares the molecular identities of benign and malignant oncocytic neoplasms using three commercially available molecular testing services. Two previous studies have investigated the molecular differences between malignant and benign oncocytic neoplasms. Both studies were performed before 2022, however, and thus use “Hürthle cell” nomenclature. Ganly et al. examined samples from 26 patients, using mass spectrometry-based genotyping to identify hotspot point mutations in common thyroid oncogenes, common oncogenic fusions, global copy number changes, and gene expression profiles.[13] This study found differences between Hürthle cell adenomas (HAs) and invasive Hürthle cell carcinoma (HCC) in gene expression and in the PIK3CA-Akt-mTOR and Wnt/β-catenin pathway. Differences between HA and HCC in general (minimally invasive and widely invasive) were not elicited, as HA and minimally invasive HCC clustered together.[13] Doerfler et al. analyzed 58 HNs using the ThyroSeq next-generation sequencing panel.[14] This study was specifically evaluating the prevalence of DNA CNAs. It found that CNAs were present in 81% of HCC and 38% of HA. They concluded that CNAs are a characteristic of both HCC and HA but occur less frequently in the latter. They noted a significant positive correlation between cancer risk and nodule size.[14]
This study was intended to re-examine those statements, considering advancing molecular technology. Within this study, there was a statistically significant difference between the occurrence of molecular negative samples between the benign and malignant groups (P = 0.0035). Due to the small sample sizes in our study, statistical analysis was not done on specific molecular positives. On visual inspection, there are certain mutations only present in certain diagnostic groups. HRAS p.Q61R, BRAF p.V600F mutations, KRAS p.G13R, ALK/EML4 gene fusions, and PAX8-PPARG gene fusions were unique to OPTCs. Seven OPTCs demonstrated HRAS Q61R mutation that was not noted in OA. Some reports found that HRAS Q61R mutation was only identified in malignant PTC cases.[23,24] However, the positive predictive value of HRAS Q61R mutation for malignancy was 45.5% in one review article.[25] EIF1AX mutations were unique to OCs in this cohort. While EIF1AX mutations recently were reported in both benign and malignant thyroid tumors, p.A113_splice mutation was more susceptible to malignancy.[26] TSHR p.D633E and TERT c.C22BT mutations were only seen in OAs. Notably, while other studies support TSHR mutations being suggestive of adenomas.[27] TERT mutations are commonly seen in malignant neoplasms.[10]
One of the previously identified defining characteristics of ONs is the presence of multiple chromosome copy number changes (MCCs), with previous studies claiming a third of all oncocytic neoplasms display MCCs.[2,14] The data from this study do not fully align with this finding, as only 24.6% (16/65) of the molecularly tested neoplasms displayed MCCs. Notably, among OAs, there was also a higher percentage of MCCs, with 33.3% (12/36) of the OAs possessing MCCs compared to 18.2% (2/11) of the OCs and 11.8% (2/17) of the OPTCs. Thus, in this study, benign OAs were more likely to display MCCs compared to malignant OC/OPTCs. This further contradicts previous research, as Doerfler et al. found that MCCs, while present in benign neoplasms, are more common in malignant neoplasms.[14] This discrepancy indicates that the presence of MCCs may not be a good indicator of a neoplasm’s malignant potential. However, further comprehensive investigation with larger case numbers would be necessary to reach a definitive conclusion.
The Bethesda System for Reporting Thyroid Cytopathology represents an international reporting system for thyroid cytology used to standardize the reporting of fine-needle aspiration cytology.[9] It divides samples into six categories based upon their malignancy likelihoods, which range from <5% malignancy likelihood to >95%. Based on the most recent updates released in 2023: Category I is nondiagnostic, Category II is benign, Category III represents atypia of undetermined significance (AUS), Category IV is FN (specify if oncocytic type), Category V is suspicious for malignancy, and Category VI is malignant. Each of these categories then has a prescribed management approach. Categories III-IV are considered indeterminant categories and may require further testing. Furthermore, only Bethesda Category IV has a specifier for oncocytic type, while Category III has specifiers for nuclear atypia.[9] As such, almost all our molecularly tested samples were either Category III (AUS) or Category IV FN/ON. Although no statistically significant difference between the Bethesda Categories and benign and malignant samples is observed in our study, Bethesda Category III is more likely to be benign (63.2%, 24/38) than Category IV (48.0%, 12/25).
Regarding secondary findings, there was a statistically significant difference between the malignant and benign groups regarding patient age, with older patients being more likely to have benign neoplasms. Previous research has shown different results, with advanced patient age (over 65) being correlated with an increased likelihood of malignancy in oncocytic neoplasms.[28,29] Our study does, however, display a similar mean age of patients, an age of around 50, as reported elsewhere.[29] Our study found no statistically significant differences between the malignant and benign groups in regard to patient gender or tumor size, however. The majority of the samples in this study were from women, which is to be expected, as previous studies found that oncocytic thyroid neoplasms were less common in men.[30] Specifically, in literature, the incidence of males is 20–30%,[31] which is very similar to the demographics in this study. Notably, previous studies also found that men have a statistically significant increased incidence of oncocytic thyroid carcinomas,[32] but this was not seen in our study. Previous research has also shown that there is a correlation between tumor size and its malignancy risk;[28,29] however, our study did not show any significant difference between the groups. This suggests that tumor size is not very predictive of a given neoplasm malignancy.
There are several limitations to this study. This is a retrospective study rooted in the review of EMRs. Thus, any data included in this study are only as reliable as those who entered the data points or measured the data points. Furthermore, our information is limited to what tests were performed at the time of identification and to what was included in reports. Notably, only tests of clinical significance were performed. This leads to another limitation of the study. Each sample was only analyzed by one assay, as that is what is clinically indicated, so results from three different genetic assays from three different companies were compared without standardization. This heterogeneity of molecular data reduces the internal consistency of the results and potentially the strength of the findings. The sample size of this study is also a limitation. As oncocytic tumors are rare thyroid tumors,[29] the number of samples was somewhat limited. Our subgroup sample sizes (OA, OPTC, NIFTP, and OC) also varied substantially, presumably reflecting the differing prevalence of the subgroup identities. All the samples in this study also came from a single institution, limiting geographic diversity. These factors, unfortunately, make identifying statistically significant results difficult, limiting the conclusions that can be drawn and their impact, as well as limiting the generalizability of the results.
SUMMARYIn conclusion, various genetic alterations are seen in both benign and malignant ONs. In this study, 3.6% (1/28) of malignant OPTC/ONs were reported as negative by molecular studies, and genetic alterations were identified in 66.6% (24/36) OAs. Notably, some genetic mutations were unique to specific groups, such as BRAF, ALK/EML4, and PAX8-PPARG in OPTCs or EIF1AX in OCs. These unique profiles may provide some insight into tumor classification; however, this information should be used with caution, as these findings are not necessarily consistent with other studies.[10] Notably, TERT and NRAS mutations were seen in benign OAs. Overall, currently available thyroid molecular testing demonstrates diversified genetic changes that cannot reliably differentiate benign from malignant ONs in the majority of cases. Our data do suggest, however, that samples testing molecularly negative are more likely to be benign ONs compared to malignant ONs.
AVAILABILITY OF DATA AND MATERIALSThe datasets used and analyzed during the present study are available from the corresponding author on reasonable request.
ABBREVIATIONSAUS: Atypia of undetermined significance
BRAF: B-Raf proto-oncogene, serine/threonine kinase
CNA: Copy number alterations
EIF1AX: Eukaryotic translation initiation factor 1A X-linked
EMR: Electronic medical record
FN: Follicular neoplasm
FNAB: Fine-needle aspiration biopsy
FTC: Follicular thyroid carcinoma
HA: Hürthle cell adenoma
HCC: Hürthle cell carcinoma
HRAS: Harvey rat sarcoma viral oncogene homolog
KRAS: Kirsten rat sarcoma viral oncogene homolog
MCC: Multiple chromosome copy number changes
NIFTP: Non-invasive follicular thyroid neoplasms with papillary-like nuclear features
NRAS: Neuroblastoma RAS viral oncogene homolog
OA: Oncocytic adenoma
OC: Oncocytic carcinoma
ON: Oncocytic thyroid follicular neoplasm
OPTC: Oncocytic papillary thyroid carcinoma
PAX8-PPARG: Paired box 8 — peroxisome proliferator activator receptor gamma
PTC: Papillary thyroid carcinoma
ROM: Risk of malignancy
TERT: Telomerase reverse transcriptase
ThyGe: ThyGeNEXT/ThyraMIR
TSHR: Thyroid stimulating hormone receptor
AUTHOR CONTRIBUTIONSSR and LR: Contributed to the study conception; LR: Contributed to the clinical management of the patients; CC and SR: Contributed to the data acquisition, analysis, and interpretation; CC and SR: Contributed to the drafting of the manuscript. All authors contributed to the critical revision and final approval of the manuscript. All authors are accountable for all aspects of the work. All authors meet the authorship status of ICMJE.
Comments (0)