Subjects
Twenty-one subjects who were aware of prediabetes were recruited through open announcements. The fifteen subjects were selected to meet the following eligibility criteria in a screening test, including a blood test using hemoglobin A1c (HbA1c) and fasting blood glucose (FBG). Inclusion criteria comprised individuals aged 19–65 with prediabetic status, as defined by the Korea Diabetes Association standards [25], including an HbA1c level of 39 mmol/mol (5.6%) to 46 mmol/mol (6.4%) or an FBG level of 100 mg/dL to 125 mg/dL. Exclusion criteria included individuals diagnosed with type 1 diabetes, an HbA1c level ≥10.2 mmol/mol (8.0%), an FBG level ≥180 mg/dL, and those using antidiabetic medications or insulin except metformin. Other exclusion criteria were body mass index (BMI) ranging from <18.5 kg/m2 or >30.0 kg/m2, use of medications or health-functional foods that have been known to affect glucose tolerance in the past 1 month; uncontrolled hypertension patients (systolic blood pressure/diastolic blood pressure ≥160/100 mmHg); medical treatments or medical severe histories of cardiovascular, endocrine metabolic, respiratory, hepatobiliary, renal, blood, or tumor disorders; participation in another study in the past 1 month; and those judged by the investigator to be inappropriate for the study.
Study design
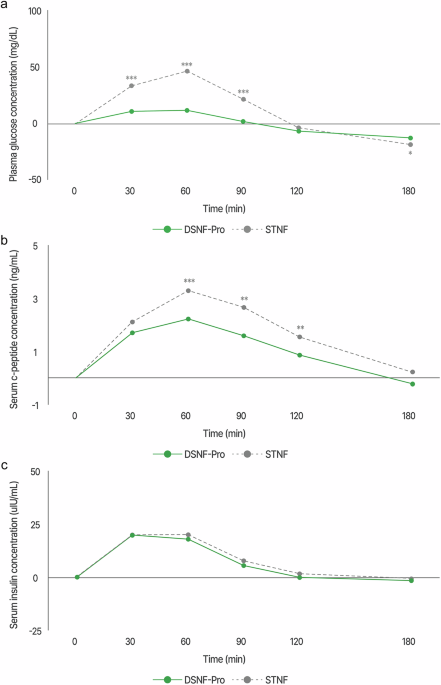
An open-label, cross-over clinical trial was conducted to assess the efficacy in fifteen adults with prediabetes. The eligible subjects were assigned to two investigational products: DSNF-Pro on the first visit and Standard nutritional formula (STNF) on the second. Since the interventions were not expected to cause any fixed or random effects, a uniform visit sequence was followed for all subjects. On each visit day, subjects visited the research facility after fasting for 10–12 h. Fasting blood samples were collected via a catheter inserted into an antecubital vein, and subjects consumed the designated investigational product within 5 min of the initial sip. Blood samples were subsequently obtained at 30, 60, 90, 120, and 180-minute post-consumption to assess plasma glucose, serum insulin, and serum c-peptide concentrations. Throughout the study, subjects maintained their regular dietary and physical activity. The subjects had a washout period of 1–14 days between visits.
Investigational products
DSNF-Pro used in this study was Nucare Glucose Plan Pro (Daesang Wellife Corp., Seoul, Republic of Korea), a 230 mL product providing 140 kcal. For comparison, the STNF widely consumed in the general population, was selected to match the isocaloric content. Nucare Glucose Plan Pro contains 12 g of protein, 12 g of carbohydrates, and 6 g of fat per serving. In contrast, the STNF includes 4.9 g of protein, 21 g of carbohydrates, and 4.2 g of fat. Notably, Nucare Glucose Plan Pro has a higher protein and fat content compared to the STNF and also contains monounsaturated fatty acids (MUFA), which are known to help regulate glucose levels, these are comprised 60% of the total fat. Additionally, it includes amounts of low glycemic index (GI) carbohydrates such as xylitol, palatinose, and dietary fiber. The nutritional profiles of the two investigational products are shown in Table 1.
Table 1 Nutrient composition of the investigational products.MeasurementsSocio-demographics and anthropometric measurement
During the screening visit, socio-demographic data, including sex, birth, lifestyle, alcohol consumption, smoking status, and medical and family history were collected. Anthropometric measurements (height, weight, body fat mass, body fat percent, skeleton muscle mass) and vital signs (blood pressure, pulse rate) were recorded at each visit. The anthropometric measurements of subjects were measured by a trained clinical trial coordinator while wearing lightweight clothing. Height was assessed using the BSM370 (Biospace Co., Ltd., Seoul, Korea) device, and weight was measured using the Inbody 970 (InBody Co., Ltd., Seoul, Korea). Height and weight measurements were rounded to one decimal place.
Glycemic profiles
Plasma glucose, serum insulin, and serum c-peptide levels were collected at each visit following a minimum 10-h overnight fast. After allowing the blood to stand at 20–25 °C for 30 min, it was centrifuged at 3000 rpm for 10 min to separate serum and plasma. The separated samples were then refrigerated at 2–8 °C. Blood samples were obtained from venous blood in ethylenediaminetetraacetic acid (EDTA)-treated tubes. Plasma glucose levels were determined using an enzymatic colorimetric glucose oxidase assay (ADAMS glucose GA-1171; Arkray Co, Kyoto, Japan). Serum insulin and c-peptide were collected from venous blood in serum separate tubes (SST) and measured using radioimmunoassay (RK-400CT; Izotop co., Budapest, Hungary, c-peptide IRMA KIT; Beckman Coulter Inc., California, United States, respectively).
Dietary assessment
Nutritional intake with subjects’ regular meals was assessed using a 24-h dietary recall method. Based on previous research indicating that the meal from the previous day affects postprandial glycemic response [26], subjects were instructed to maintain their usual dietary habits throughout the study. At each visit, subjects reported their dietary intake from the previous day, and a registered dietitian conducted interviews to gather information on their dietary choices. Daily nutritional intake analysis was performed using the CAN-Pro program (CAN-Pro 6.0; Korean Nutrition Society, Seoul, Korea).
Physical activity assessment
The physical activity of the subjects was assessed using the International Physical Activity Questionnaire (IPAQ). The IPAQ was recorded weekly for the typical physical activities of the subjects. Physical activity was expressed as the metabolic equivalent task (MET)-min/week (MET level × activity minutes/day × activity days/week). MET scores were calculated based on the intensity of activity as follows: vigorous intensity, 8 METs; moderate intensity, 4 METs; and walking, 3.3 METs (IPAQ Research Committee, 2005).
Ethics
All subjects were provided with detailed information about the experimental procedures and the associated risks, before obtaining their written informed consent. The study was conducted according to the guidelines established in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Institutional Review Board of Kyung Hee University Hospital (KHUH 2023-05-091) and registered at the Clinical Research Information Service (CRIS) of the Korea Disease Control and Prevention Agency (KDCA) (Registration Number KCT0008904).
Statistical analysis
The primary outcome was the changes in postprandial glucose response comparing DSNF-Pro to STNF. Secondary outcomes were changes in postprandial insulin and c-peptide. Sample size calculations were conducted using G*Power Software for version 3.1.9.7 (Heinrich-Heine-University Düsseldorf, Germany). A sample size of 12 subjects was calculated as adequate for detecting variations in glucose incremental area under the curve (iAUC) with 90% statistical power at a 5% α level, assuming matched pairs based on a prior study [27]. Consequently, a sample size of 15 was calculated, considering a drop-out rate of 20%.
Statistical analyses were executed using SAS version 9.4 (SAS Institute, Cary, NC, USA). Descriptive statistics were presented as means ± standard deviation (SD) for continuous variables, and categorical variables were expressed as n (%). Wilcoxon’s signed rank test was used for variables to compare group differences. The iAUC for postprandial glucose, insulin, and c-peptide were individually calculated using the trapezoid rule [28]. Integrals were determined for each time interval and changed from baseline to the 180-minute endpoint, with the exclusion of the area beneath the baseline concentration. Additionally, the maximum concentration (Cmax) and the incremental maximal concentration (iCmax) were determined by subtracting each baseline value from Cmax. Statistical significance was defined as a p-value < 0.05.

Comments (0)