This randomized, double-blind, placebo-controlled trial was conducted at a tertiary care government hospital in Maharashtra from December 2019 to April 2021. All children with cerebral palsy, between the age group of 3 to 12 y attending pediatric OPD and wards with sleep problems defined as those who did not fall asleep within 1 h of the lights off, waking up once or more during night, children getting less than 6 h of sleep and who failed behavioral management strategies for sleep disturbances, were enrolled. Children previously and currently treated with melatonin, with known allergy to melatonin, those with symptoms and signs suggestive of obstructive sleep apnea syndrome, with nocturnal seizures, and whose parents or caretakers were unwilling to participate in the study were excluded. The Institutional Ethical Committee approved the trial, and CTRI registration was done (CTRI/2020/09/027813). Written informed consent was taken from parents/caregivers.
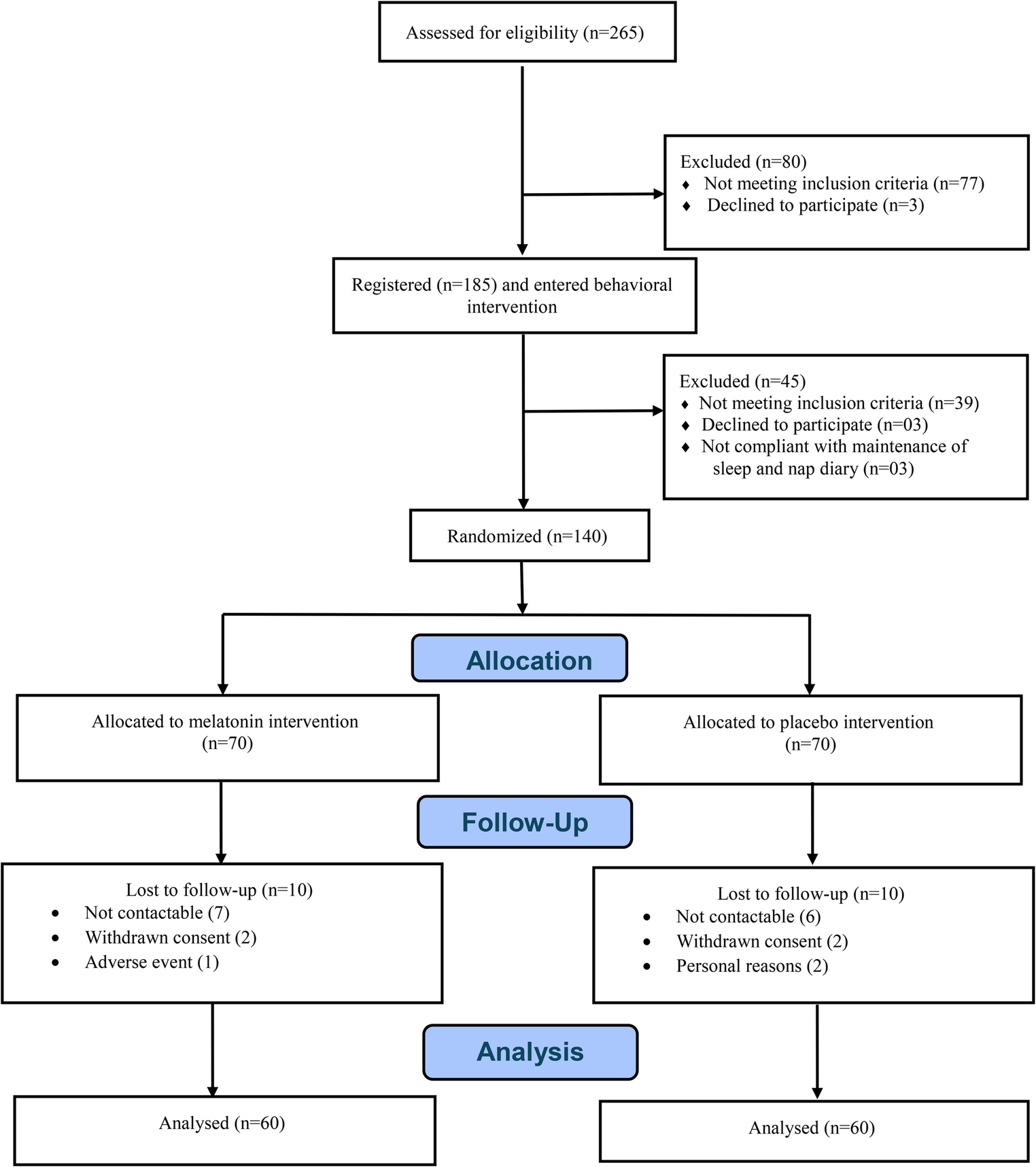
The sample size of 120 was calculated using open-Epi Version 3.01 software based on mean difference (MD) and standard deviation (SD) values from a previous randomized controlled trial [6]. The study was designed to detect a 1 h difference in total sleep time (TST) between the melatonin group and the placebo group. Assuming a typical standard deviation of 1.7 (based on published data in similar settings), a sample size of 46 per group increased to 60 per group to allow for an estimated 20% loss to follow-up, thereby providing 80% power using a t-test with a 0.05 two-sided significance level, was required.
All children diagnosed with cerebral palsy attending the pediatric OPD and IPD during the study period were screened and assessed for eligibility. Those meeting the above inclusion criteria were enrolled. The medical staff administered a sleep questionnaire to parents/caregivers to ask: The average time it takes to fall asleep; average number of night awakenings; total time of nocturnal sleep; average total time of diurnal sleep and the presence of early morning arousals. Patients were recruited for the study by the primary investigator based on the analysis of the sleep questionnaire, which was completed on an estimated basis, indicating the persistence of a sleep disorder for at least 6 mo.
Baseline clinical history, physical examination, type of CP, and Gross Motor Function Classification System (GMFCS) level of the subjects were recorded. Sleep disturbances were assessed using the Sleep Disturbance Scale for Children (SDSC) and sleep diaries. The SDSC scale is a validated scale for assessing sleep disturbances in children, evaluating the occurrence of sleep disorders over the previous 6 mo. It consists of 26 items on a Likert-type scale, with values ranging from 1 to 5; higher numerical values indicate a greater clinical severity of symptoms. The sum of scores provided a total sleep score ranging from 26 to 130. A total score of ≥ 51 (>95th centile) was regarded as abnormal, and a score of less than 51 was considered to be normal [4]. Sleep and nap diaries (SND) were used to gather information from parents regarding their child’s daily sleep behaviors and pre-bedtime practices. In these diaries, parents were asked to make nightly recordings of the time the child goes to bed and falls asleep, the frequency and timing of night awakenings, the time the child wakes up in the morning, and the times of daytime naps [8]. Parents were asked to fill in the data at least 5 d a week throughout the study, and then the data were averaged by medical staff every 4 wk. Baseline sleep disturbance scores for children [10] and sleep diary were recorded at the intervention’s start and end.
All the recruited patients were advised behavioral therapy for 4 wk to ensure that children progressing to the randomization phase did not include those whose sleep disorder would respond to non-pharmacological intervention. During behavioral therapy, the parents were explained general sleep hygiene principles (bedtime routine and using it every night, putting child to bed while he is still awake, avoiding daytime naps, rewarding good nighttime behavior, trying not to give night time drinks, trying to avoid taking child into own bed for sleep, trying to be as dull as possible when dealing with child at night were used, settling your child to sleep, changing the time when your child sleeps) and strategies for dealing with problems of settling to sleep.
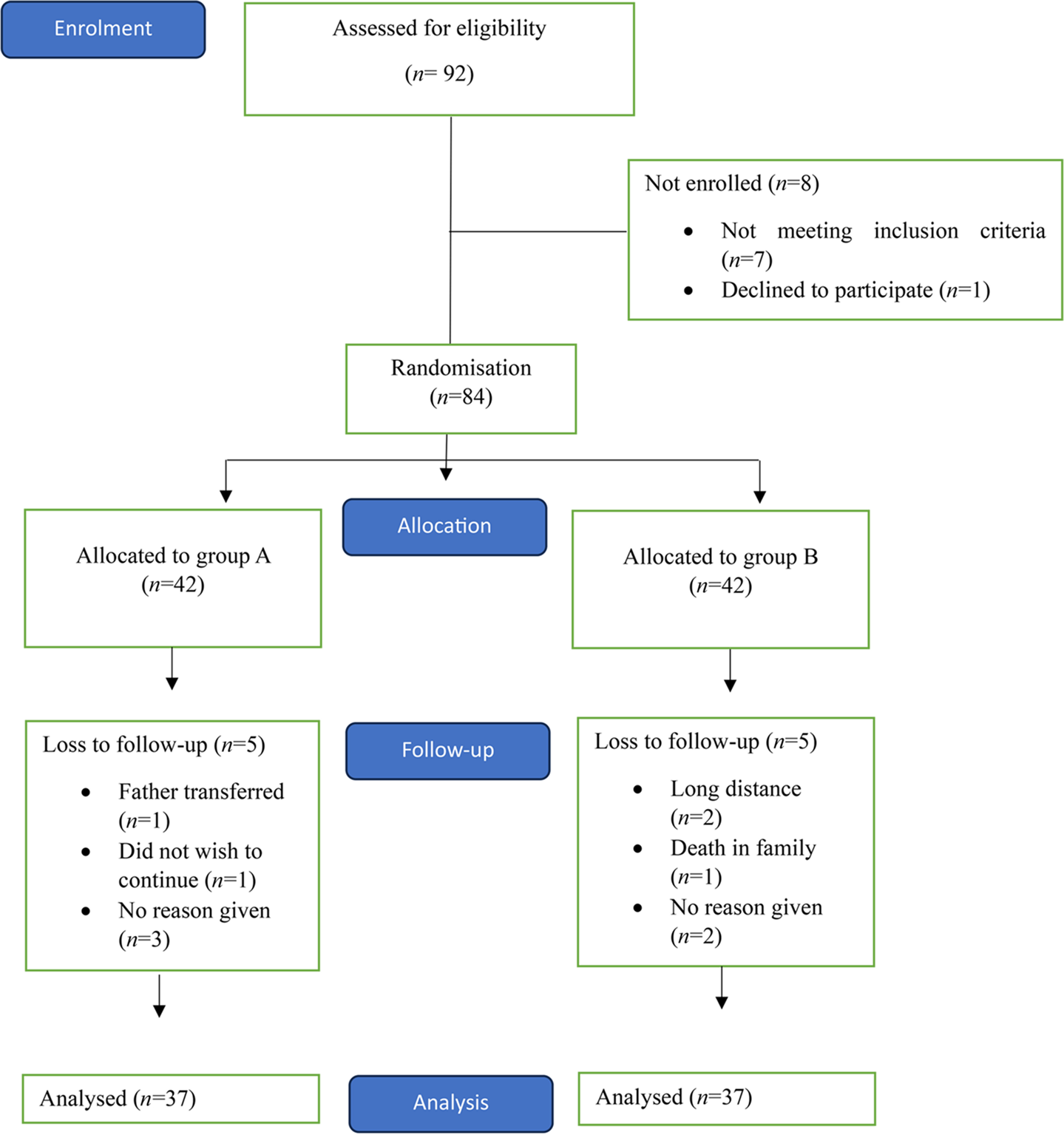
Children who failed behavioral therapy were finally recruited into the study. Enrolled patients were allocated into melatonin and placebo groups using Computer-generated random sequences with permutated blocks of variable sizes of 4 or 6 each. Allocation concealment was achieved using sequentially numbered, opaque, sealed envelopes by a researcher not involved in the administration or assessment of the drug. Blinding and randomization were performed by a researcher who was not involved in patient management.
The melatonin group received oral melatonin tablets (Altonil, Alteus Biogenic Limited, 3 mg, and 5 mg tablets) at a dose of 3 mg/d initially, and the other group received a similar placebo (matching in package and appearance). The drugs were administered 30 to 45 min before the child’s usual bedtime. Enrolled subjects were followed up every 15 d to monitor the effect of the intervention on sleep for a complete duration of 12 wk. Evaluation of various sleep parameters and side-effects (somnolence, increased excitability, mood swings, seizures, rash, hypothermia, and cough) of melatonin was conducted every 4 weekly. Based on these evaluations, dose escalation to 5 mg/d and subsequently to 10 mg/d was done at 4 wk and 8 wk respectively if there was persistence of inclusion criteria for sleep difficulties. Children whose sleep parameters improved were considered responders, and their dose remained unchanged.
The primary outcome was total nighttime sleep and was calculated using sleep and nap diary at 12 wk compared to the baseline. The secondary outcome was sleep onset latency (SOL) at 12 wk compared to the baseline.
The data obtained were compiled on an MS Office Excel and statistical analysis performed using the SPSS v 26.0, IBM. Descriptive statistics - frequencies and percentages for categorical data and mean and standard deviation (SD) for numerical data, have been depicted. An inter-group comparison was performed using an unpaired t-test, within-group using a paired t-test and Chi-Square test for categorical data. For all the statistical tests, p < 0.05 was considered statistically significant. The analysis was done using the per-protocol analysis. Cohen’s d formula calculated the effect size.





Comments (0)