The study indicates that MUAC is a significant predictor of WHZ. Other studies have demonstrated a strong correlation between MUAC and WHZ across various contexts [4, 11]. Additionally, MUAC predicts child mortality better compared to other anthropometric indicators, including WHZ [11,12,13]. This reinforces the importance of using MUAC as a reliable tool for malnutrition screening in limited resource areas.
The findings conclude that the new MUAC thresholds are effective for identifying wasting (WHZ <−2) and severe wasting (WHZ <−3) in children. The study identified suitable MUAC thresholds for detecting wasting (WHZ <−2) and severe wasting in community settings. MUAC cut-offs were found to be < 13.2 cm for children 6–23 mo, < 13.9 cm; for 24–59 mo, and < 13.9 cm for overall 6–59 mo, for identifying wasting. For severe wasting, MUAC < 12.8 cm (for children 6–23 mo), < 13.4 cm (for children 24–59 mo), and < 12.9 cm for the overall age range. In community settings, where measuring height, length, and weight can be challenging due to the unavailability of proper equipment and logistical issues, as well as the risk of measurement errors by community health workers, MUAC measurement emerges as a practical alternative for detecting wasting and severe wasting.
The findings indicate that MUAC thresholds for wasting and severe wasting are slightly higher in older children (24–59 mo) compared to younger ones (6–23 mo), highlighting the need for age-specific thresholds. This approach can enhance screening accuracy and guide targeted interventions. While WHO recommends a single cut-off [1], other studies, like the present one, support the age-specific use of MUAC to better address childhood malnutrition and reduce morbidity and mortality [14, 15].
Several studies have proposed varying MUAC thresholds for detecting SAM in children. Laillou et al. (2014) suggested 13.3 cm [12], Fiorentino et al. (2016) reported 13.9 cm (children < 2 y) and 14.4 cm (2–5 y) in Cambodia [15], and Hai (2020) found 13.5 cm suitable in Vietnam [16]. Analyses from Africa [16] and multi-country studies [10] recommended 13.5 cm and 13.23 cm, respectively. These variations highlight the importance of context-specific MUAC guidelines for effective SAM screening across different populations and regions.
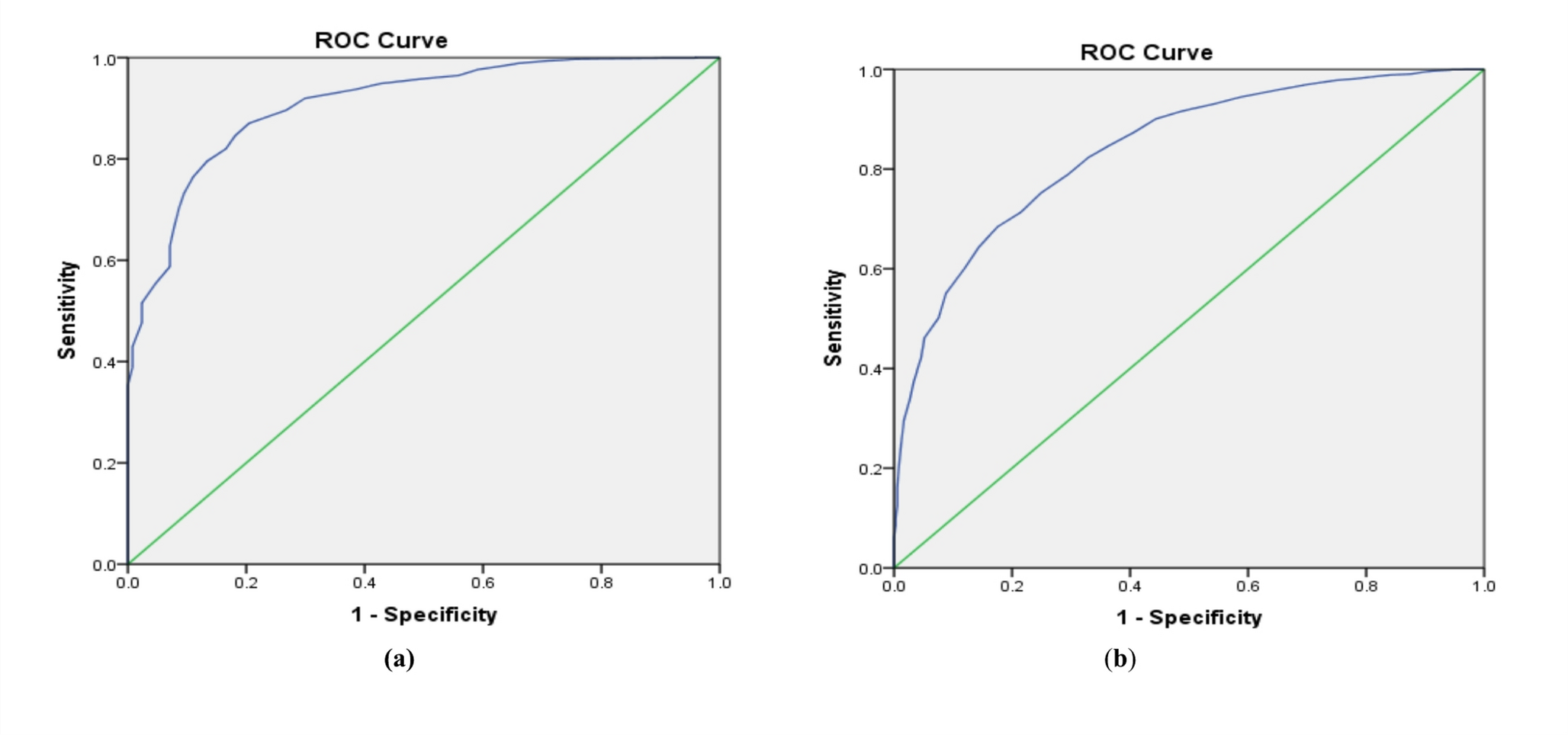
The MUAC thresholds identified in this study for children 6–59 mo showed sensitivities of 82% for wasting and 80% for severe wasting. However, some true cases may still be missed using MUAC < 13.9 cm for wasting and < 12.9 cm for severe wasting. To improve detection, higher cut-offs of < 14.5 cm (97% sensitivity) for wasting and < 13.5 cm (92% sensitivity) for severe wasting are recommended. Children below these thresholds would be sent to the nearest health centres for further assessment.
The Government of India is currently implementing the nationwide Integrated Child Development Services (ICDS) program through an extensive network of Anganwadi Centres (AWCs). In addition, the central government has recently introduced guidelines for Community-Based Management of Acute Malnutrition (CMAM) to improve the identification and management of uncomplicated SAM at the community level. Several state governments have already begun integrating CMAM interventions within the existing ICDS framework. To further strengthen the effectiveness of wasting and severe wasting screening, the government could consider adopting the MUAC cut-offs identified in this study as a standardized tool for the first level of SAM screening at AWCs. Children whose MUAC measurements fall below these thresholds can then be sent to the nearest health facilities for comprehensive assessment and confirmation of SAM status. This two-tiered approach would enhance the accuracy of community-level screening, minimize the risk of missing true SAM cases, reduce program costs by ensuring accurate targeting of vulnerable children, and facilitate timely treatment and improved nutritional outcomes for vulnerable children. Such a strategy would also align with national efforts to strengthen community-based nutrition interventions to address child malnutrition and associated mortality in India [17].
Addressing childhood malnutrition also requires a holistic approach beyond screening and treatment. It must ensure adequate nutrition while addressing socio-demographic factors like maternal education, sanitation, and healthcare access. Long-term solutions should focus on improving socioeconomic status through poverty reduction, social protection, and community empowerment, fostering sustainable reductions in malnutrition and enhancing overall child well-being [18].
The strength of this study lies in its coverage of five high-burden areas across four Indian states, providing a representative assessment. It supports using MUAC for quick, effective community-level screening of wasting and severe wasting in children. However, since the study is India-specific, its findings may not apply globally. Establishing international MUAC cut-offs will require a meta-analysis using large, diverse datasets from multiple countries.





Comments (0)