
Remember me
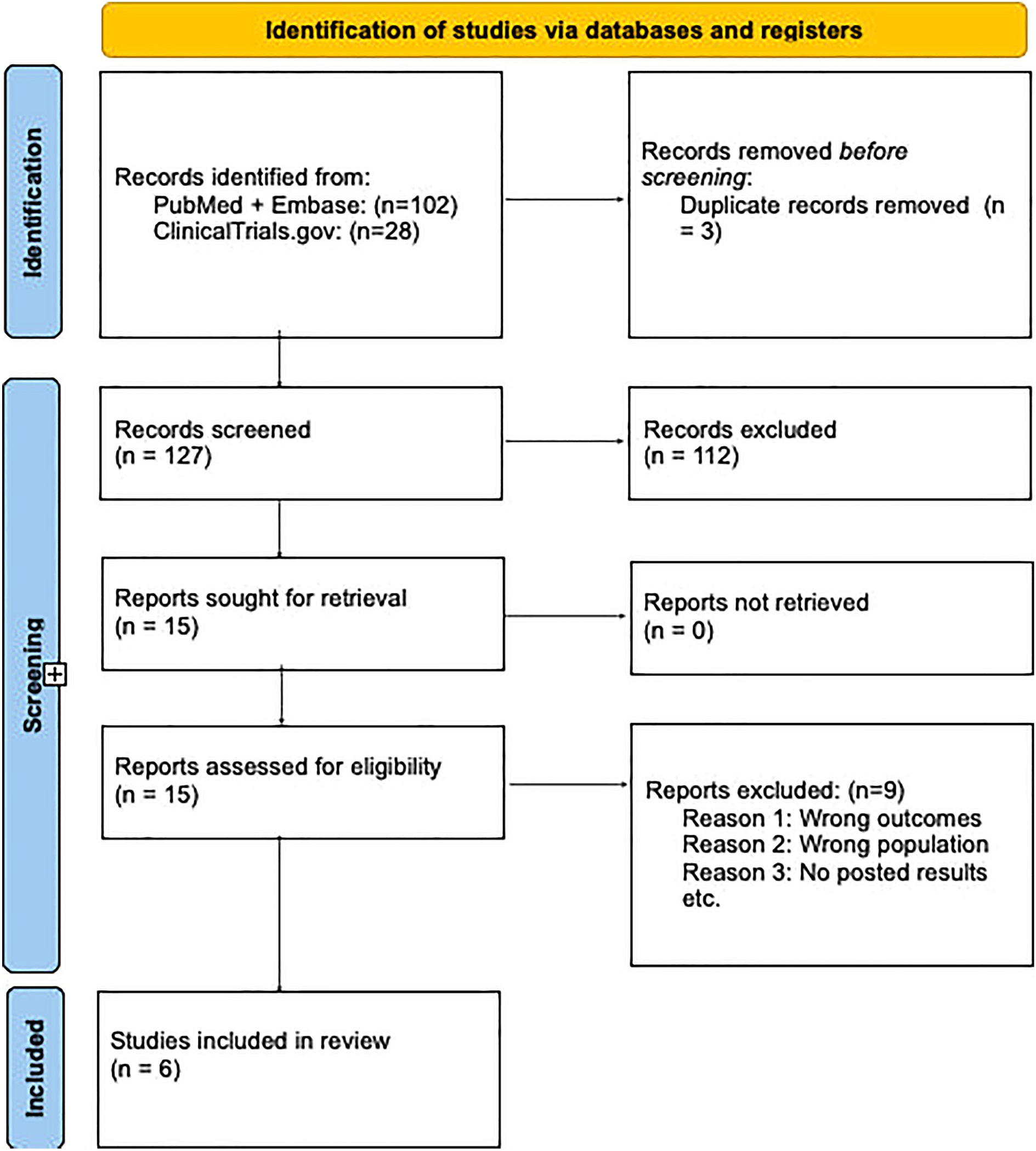
From a total of 511 studies eligible for full-text screening, 162 studies were included to form the main evidence base for selecting relevant studies for the meta-analyses (Figure S1).
Overall, 33 studies (providing 42 unique estimates of prevalence) and 66 studies (providing 124 unique estimates of prevalence) were included for meta-analyses in 18–59-year-old high-risk adults with respiratory illnesses and ≥ 50-year-old adults with respiratory illnesses, respectively (Table 1). This included two abstracts for the 18–59-year-old high-risk population, and two abstracts and six weblinks for the ≥ 50-year-old population. For 18–59-year-old high-risk adults, the total number of patients across the 33 studies was 55,890. For ≥ 50-year-old adults, the total number across the 66 studies was 80,214 (Table 1).
Table 1 Summary of the studies analyzed to estimate the prevalence of RSV among 18–59-year-old high-risk and ≥ 50-year-old adults with respiratory illnesses18–59-Year-Old High-Risk Adults with Respiratory IllnessesOf the 33 studies reporting prevalence data for the 18–59-year-old high-risk population, 14 were from Latin America, while seven studies each were from Africa and Southeast Asia. Fewer studies were available from the Middle East/Eastern Mediterranean (n = 4) and one study reported data for multiple regions. Studies reporting estimates for 18–59-year-old high-risk adults with respiratory illnesses were either cross-sectional (n = 16), prospective cohort (n = 10), retrospective cohort (n = 6), or retrospective and prospective cohort (n = 1) studies.
A summary of further study characteristics of the included articles, including study setting, respiratory illness, RSV diagnostic method, and high-risk condition, is provided in Table S1.
≥ 50-Year-Old Adults with Respiratory IllnessesOf the 66 studies reporting prevalence data for the ≥ 50-year-old population, most were from Latin America (n = 27) or Southeast Asia (n = 19), while fewer were from the Middle East/Eastern Mediterranean (n = 10) or Africa (n = 9). One study reported data from multiple regions. Estimates for ≥ 50-year-old adults with respiratory illnesses were derived from cross-sectional (n = 38), prospective cohort (n = 22), retrospective cohort (n = 5), or retrospective and prospective cohort (n = 1) studies.
A summary of further study characteristics of the included articles, including study setting, respiratory illness, RSV diagnostic method, and age group is provided in Table S2.
Prevalence of RSV Among 18–59-Year-Old High-Risk Adults with Respiratory IllnessesPooled EstimateThe pooled estimate for RSV prevalence among 18–59-year-old high-risk adults with respiratory illnesses was 5.1% (95% CI 3.9–6.6%; Fig. 1A). The Q value was 892, with 41 degrees of freedom (p < 0.01), suggesting significant heterogeneity across studies. The I2 value was 95%. The prediction interval indicated that, in 95% of similar populations (or future studies), the RSV prevalence was likely to fall between 1.1% and 20.0%.
Fig. 1

Pooled estimate of RSV prevalence among A 18–59-year-old high-risk adults and B ≥ 50-year-old adults, both with respiratory illnesses. Studies are organized in an ascending order of RSV prevalence. The NOS was used for quality assessment [20]; total scores can range from 0 (lowest quality) to 9 (highest quality). In A, three estimates from conference abstracts were not evaluated for study quality. In B, 22 estimates from conference abstracts were not evaluated for study quality. Additionally, 12 estimates in B reported only the overall RSV prevalence and did not provide information on the actual number of RSV cases and total sample size. Therefore, an imputed total sample size of 181 (the median sample size across all the remaining 112 estimates) was used. The number of RSV cases for those 12 estimates was then calculated based on the imputed total sample size and the reported RSV prevalence. ARI acute respiratory illness, CI confidence interval, I inpatients, ILI influenza-like illness, NOS Newcastle–Ottawa Scale, NR not reported, O outpatients, RSV respiratory syncytial virus, SARI severe ARI
Influence AnalysisRemoval of any one study did not appear to affect the overall pooled estimate in a meaningful way (i.e., the pooled prevalence estimate did not change by greater than ± 10%). However, removing the two estimates from Luna et al. [45] reduced tau-squared from 0.57 to 0.51 for each estimate, whereas removing the Piralam et al. [46] and the Moyes et al. [47] studies increased tau-squared from 0.57 to 0.66 and 0.65, respectively, demonstrating an impact on the overall heterogeneity of effect sizes.
Subgroup AnalysisBy GeographyThe overall pooled prevalence of RSV was 7.8% (95% CI 5.5–10.8) in Latin America, 3.0% (95% CI 1.8–4.9) in Africa, 2.9% (95% CI 1.6–5.1) in Southeast Asia, and 8.0% (95% CI 3.3–18.3) in Middle East/Eastern Mediterranean (Figure S2). The difference between the four subgroups was statistically significant (p < 0.01). The level of heterogeneity (I2) within regions ranged from 57% in the Middle East/Eastern Mediterranean to 93% in Africa.
Studies from Africa comprised the largest sample size (n = 37,290), followed by Southeast Asia (n = 12,060), Latin America (n = 6036), and the Middle East/Eastern Mediterranean (n = 504).
For 18–59-year-old high-risk adults with respiratory illnesses, studies from the Middle East/Eastern Mediterranean were conducted exclusively in Turkey, and reported the highest pooled prevalence (8.0%) among all the regions. The small sample size in this subgroup resulted in wider CIs compared to other regions. R2 analog was 53.3%.
By Study SettingThe overall pooled prevalence of RSV was 15.4% (95% CI 1.3–71.4) in studies reporting data from both inpatient and outpatient settings, 4.8% (95% CI 3.5–6.6) in inpatient settings, and 3.6% (95% CI 2.5–5.0) in outpatient settings (Figure S3). The difference among the three subgroups was statistically significant (p = 0.03). The level of heterogeneity (I2) was 77% in the outpatient subgroup, 95% in the inpatient subgroup, and 89% in the combined inpatient and outpatient subgroup.
The sample size was much larger in the inpatient subgroup (n = 46,030) compared to the outpatient subgroup (n = 9279) and the combined inpatient and outpatient subgroup (n = 542).
The inpatient and outpatient subgroup exhibited notably wider CIs (95% CI 1.3–71.4) due to its small sample size of 542. After excluding the three studies reporting data from both inpatient and outpatient settings, the difference between the inpatient and outpatient subgroups was not statistically significant (p = 0.174). R2 analog was 18.7%.
By Respiratory IllnessThe overall pooled prevalence of RSV was 9.4% (95% CI 3.8–21.1) in patients with ARI, 4.8% (95% CI 3.4–6.7) in patients with SARI, 2.8% (95% CI 2.0–3.9) in patients with ILI, and 5.0% (95% CI 1.1–19.5) in patients with pneumonia-related illnesses (Figure S4). The difference between the four subgroups was statistically significant (p < 0.01). The level of heterogeneity (I2) ranged from 65% in the ILI subgroup to 95% in the SARI subgroup.
The sample size was notably larger in the SARI subgroup (n = 44,978) compared to the ILI (n = 8411), ARI (n = 1325), and pneumonia-related (n = 1176) subgroups. R2 analog was 20.2%.
Additional Subgroup AnalysesThe results of additional subgroup analyses by publication quality, country income level, sampling technique, high-risk condition, and diagnostic method are presented in full in the Supplementary Results.
Predictors of RSV Prevalence (Meta-Regression)Studies from Latin America had 2.83 times greater odds of reporting RSV compared to studies from Southeast Asia after controlling the effects of study setting and respiratory illness (p = 0.006; Table 2).
Table 2 Meta-regression for three predictors of RSV prevalence among 18–59-year-old high-risk adults with respiratory illnessesStudies reporting data from both inpatient and outpatient settings had 4.37 times greater odds of reporting RSV compared to studies that only included outpatient data, after controlling for the effects of geography and respiratory illness (p = 0.022; Table 2).
Study geography, study setting, and respiratory illness together accounted for ~ 54% of variation in the RSV prevalence estimates across studies included in the analysis.
Sensitivity AnalysisCompared to random-effects IV models, which reported pooled estimates ranging from 4.89% to 5.26%, the GLMM produced a slightly lower pooled estimate (4.84%; Table S3).
With other statistical parameters held constant, the Freeman–Tukey transformation yielded marginally different prevalence estimates compared to the logit transformation. The difference in pooled prevalence estimates using different between-study variance estimators was negligible when applying the logit transformation method (range 5.07–5.08%). However, when applying the Freeman–Tukey double arcsine method, there was a slight difference in pooled estimates (range 4.89–5.26%), but this was of little practical significance.
Publication BiasIn the cumulative meta-analysis by sample size, the 14 smallest studies (sample size ≤ 150) reported a high pooled RSV prevalence of 8.7%. As larger studies were included, the pooled prevalence estimates decreased and became more stable, approaching a pooled value of 5.1%. Seven out of the 14 smaller studies were rated as low quality.
Prevalence of RSV Among ≥ 50-Year-Old Adults with Respiratory IllnessesPooled EstimateThe pooled estimate for RSV prevalence among ≥ 50-year-old adults with respiratory illnesses was 3.9% (95% CI 3.3–4.7%; Fig. 1B). The Q value was 1738, with 123 degrees of freedom (p < 0.01), suggesting significant heterogeneity between studies. The I2 value was 93%. The prediction interval indicated that, in 95% of similar populations (or future studies), the RSV prevalence was likely to fall between 0.7 and 18.7%.
Influence AnalysisRemoval of any one study did not appear to affect the overall pooled estimate in a meaningful way (i.e., the pooled prevalence estimate did not change by greater than ± 10%). However, removing the first Mexico Ministry of Health [48] and fifth World Health Organization (WHO) Global RSV [49] Argentinian estimates reduced tau-squared from 0.75 to 0.70 and 0.67, respectively, whereas removing the Al-Romaihi et al. [50] study increased tau-squared from 0.75 to 0.88, demonstrating an impact on the overall heterogeneity of effect sizes.
Subgroup AnalysisBy GeographyThe overall pooled prevalence of RSV was 3.3% (95% CI 2.4–4.6) in Southeast Asia, 4.6% (95% CI 3.3–6.4) in Latin America, 3.7% (95% CI 2.8–4.8) in Africa, and 4.2% (95% CI 2.7–6.2) in the Middle East/Eastern Mediterranean (Figure S5). The difference between the four subgroups was not statistically significant (p < 0.47). The level of heterogeneity (I2) within regions ranged from 79% in Africa to 96% in Latin America.
Studies from Latin America comprised the largest sample size (n = 37,115), followed by Southeast Asia (n = 16,111), Middle East/Eastern Mediterranean (n = 15,871), and Africa (n = 11,117). R2 analog was 0%.
By Study SettingThe overall pooled prevalence of RSV was 3.8% (95% CI 3.0–4.7) in studies reporting data from inpatient settings, 3.7% (95% CI 2.4–5.8) in outpatient settings, and 4.2% (95% CI 2.7–6.3) in both inpatient and outpatient settings (Figure S6). The difference among the three subgroups was not statistically significant (p = 0.91). The level of heterogeneity (I2) was 89% in the inpatient subgroup, 78% in the outpatient subgroup, and 96% in the combined inpatient and outpatient subgroup.
The sample size was comparable between the inpatient subgroup (n = 28,908) and the combined inpatient and outpatient subgroup (n = 28,141), whereas it was notably smaller in the outpatient subgroup (n = 3729). R2 analog was 0%.
By Respiratory IllnessThe overall pooled prevalence of RSV was 4.4% (95% CI 3.2–6.0) in patients with ILI, 3.9% (95% CI 3.1–4.8) in patients with SARI, 4.6% (95% CI 2.1–9.8) in patients with ARI, 3.7% (95% CI 1.8–7.2) in patients with pneumonia-related illnesses, and 3.2% (95% CI 1.7–6.0) in patients with multiple respiratory illnesses (Figure S7). The difference between the five subgroups was not statistically significant (p = 0.88). The level of heterogeneity (I2) ranged from 84% in the ARI subgroup to 97% in the multiple subgroup.
The sample size was considerably larger in the SARI (n = 29,647), ILI (n = 21,630), and multiple (n = 21,268) subgroups compared to the ARI (n = 2692) and pneumonia-related (n = 4977) subgroups. R2 analog was 0%.
By Diagnostic MethodThe overall pooled prevalence of RSV was 3.0% (95% CI 2.2–4.0) in studies reporting multiplex-based diagnosis, 1.6% (95% CI 0.2–15.3) in multiple diagnosis, 3.9% (95% CI 3.1–4.9) in PCR-based diagnosis, and 7.2% (95% CI 3.8–13.4) in antigen-based diagnosis (Figure S8). The difference between the four subgroups was statistically significant (p = 0.03). The level of heterogeneity (I2) was 61% in the multiplex-based diagnosis subgroup, 83% in the multiple diagnosis subgroup, and 94% in both PCR-based and antigen-based diagnosis subgroups.
The sample size was considerably larger in the PCR-based diagnosis subgroup (n = 59,746), compared to the multiplex-based subgroup (n = 5774), multiple subgroup (n = 2931), and the antigen-based subgroup (n = 4567).
After excluding the studies from the multiplex-based diagnosis and multiple diagnosis subgroups, the difference between the PCR-based and antigen-based diagnosis subgroups was statistically significant (p = 0.024). R2 analog was 7.9%.
Additional Subgroup AnalysesThe results of additional subgroup analyses by publication quality, country income level, sampling technique, and age group (50–65 years and > 65 years) are presented in full in the Supplementary Results.
Predictors of RSV Prevalence (Meta-Regression)Studies using antigen-based diagnosis had 2.08 times greater odds of reporting RSV compared to studies using PCR-based diagnosis (p = 0.024; Table 3). Diagnosis accounted for ~ 8% of variation in the RSV prevalence estimates across studies included in the analysis.
Table 3 Meta-regression for one predictor of RSV prevalence among ≥ 50-year-old adults with respiratory illnessesSensitivity AnalysisCompared to random-effects IV models, which reported pooled estimates ranging from 3.43% to 3.92%, the GLMM model produced a slightly lower pooled estimate of 3.41% (Table S4).
With other statistical parameters held constant, the Freeman–Tukey transformation yielded marginally lower prevalence estimates compared to the logit transformation. The difference in pooled prevalence estimates using different between-study variance estimators was negligible when applying the logit transformation method (range 3.91–3.92%). However, when applying the Freeman–Tukey double arcsine method, there was a slight difference in pooled estimates (range 3.43–3.57%).
With other statistical parameters held constant, removing imputed studies from the dataset did not have any material impact on the pooled prevalences.
Publication BiasIn the cumulative meta-analysis by sample size, as studies were added in an ascending order of sample size, the pooled prevalence estimates gradually decreased and stabilized, converging to a pooled value of 3.9%.
Comments (0)