Study Design and Data Sources
This study employed a retrospective observational matched-cohort design and data from a large US healthcare claims repository, the IQVIA PharMetrics Plus Database. Data for this study spanned the period from January 2016 through 31 March 2024 (“study period”). The PharMetrics Plus Database comprises fully adjudicated medical (i.e., facility and professional service) and outpatient pharmacy claims from a large number of health plans, and contains a longitudinal view of healthcare utilization and expenditures across the continuum of care settings. Per IQVIA, the enrollee population is generally representative of the commercially insured US population less than 65 years of age with respect to both age and sex.
Data available from each facility and professional-service claim include dates and places of service, diagnoses, procedures, and quantity of services (professional-service claims only). Data available for each outpatient pharmacy claim include the drug dispensed, dispensing date, quantity dispensed, and number of days supplied. Medical and pharmacy claims also include amounts paid (i.e., reimbursed) by health plans for healthcare services rendered. Selected demographic and eligibility information (including age, sex, three-digit zip code, payor/product type, dates of plan eligibility) is available for all health plan enrollees in the database.
The study database was deidentified prior to its release to study investigators, as set forth in the corresponding Data Use Agreement. Use of the study database for health services research was fully compliant with the Health Insurance Portability and Accountability Act Privacy Rule and federal guidance on Public Welfare and the Protection of Human Subjects (45 CFR 46§46.101). Institutional review board approval was not required.
Source Population
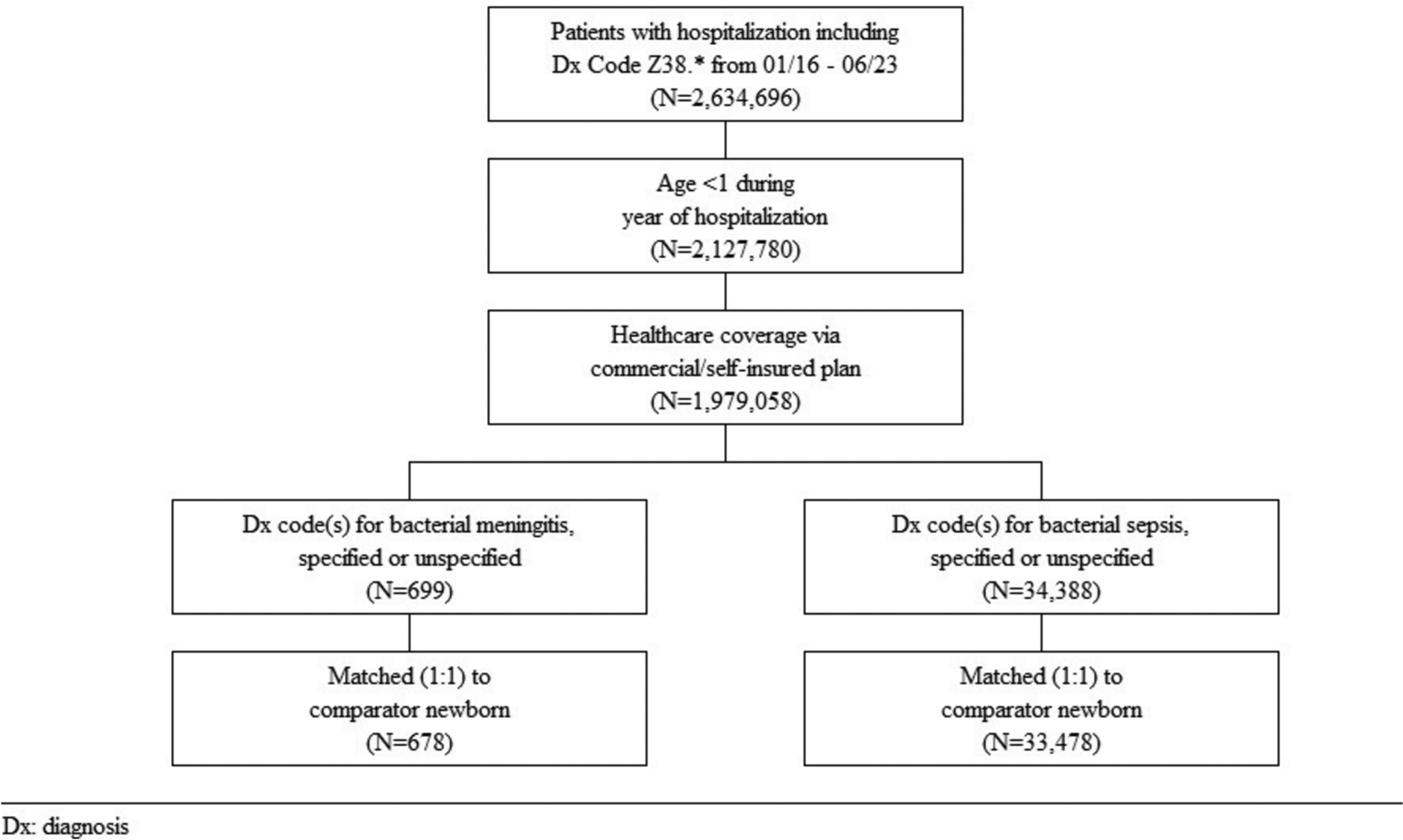
The source population comprised all newborns between January 2016 and March 2023 who had medical coverage via a commercial or self-insured payor on their date of birth. Births were identified on the basis of hospitalizations with diagnosis codes Z38.* (liveborn infants according to place of birth and type of delivery) and patient age < 1 year. For newborns who were transferred from their birth hospital to another acute-care facility (e.g., owing to the need for higher level of care), the two admissions were merged to create a single hospitalization (hereafter referred to as “birth hospitalization”).
Study Population
From the source population, all newborns (“cases”) who had evidence of meningitis, sepsis, or pneumonia due to a bacterial pathogen during their birth hospitalizations were identified. Clinical manifestations and bacterial pathogens were ascertained on the basis of operational algorithms and International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes (any position) on claims associated with birth hospitalizations (Supplementary Table 1). Qualifying newborns were classified into subgroups defined by clinical manifestation (i.e., meningitis, sepsis, or pneumonia) and infection type (any bacterial infection [including E. coli/GBS], E. coli, GBS). E. coli and GBS subgroups were included as these pathogens are leading causes of pediatric invasive disease [6, 18]. Newborns with evidence of multiple manifestations were classified via a hierarchy: if evidence of meningitis, then meningitis; if no evidence of meningitis and evidence of sepsis, then sepsis; if no evidence of meningitis/sepsis and evidence of pneumonia, then pneumonia.
Each case was matched (1:1, without replacement) to a comparator newborn from the source population without evidence of meningitis, sepsis, or pneumonia during their birth hospitalization. Matching was implemented for each case by randomly selecting all potential comparators who were born in the same calendar year and season (October–March versus April–September) and had the same gestational age in weeks (wGA) at birth (< 33, 33–36, ≥ 37; Supplementary Table 2), birth weight (< 1000, 1000 to < 2500, ≥ 2500 g), comorbidity profile (≥ 1 versus 0 high-risk condition; Supplementary Table 3), and sex (male, female). From all potential comparators, the one with the closest propensity score to the case—based on three-digit zip code, payor type, and product type (e.g., health maintenance organization)—was selected for inclusion in the study population.
Early and late preterm births were determined on the basis of diagnosis codes for short gestation listed on claims associated with birth hospitalizations; the absence of a code for short gestation was assumed to denote a term birth (wGA ≥ 37). Low birth weight was determined on the basis of ICD-10 diagnosis codes on birth hospitalization claims; the absence of a code for low birth weight was assumed to denote normal birth weight (≥ 2500 g). For newborns with missing three-digit zip codes (e.g., those residing in areas with populations < 20,000 persons), state of residence was used in the matching procedure. High-risk conditions (e.g., bronchopulmonary dysplasia, lung abnormalities, congenital heart disease) were identified on the basis of ICD-10 diagnosis codes in the principal or secondary position on birth hospitalization claims.
Study Variables
Baseline characteristics included birth wGA, birth weight, sex, comorbidity profile, payor type, product type, and year of the birth hospitalization, as defined above. Study measures ascertained during the birth hospitalization (“acute period”) included hospital length of stay (LOS), admission to the intensive care unit (ICU), use of mechanical ventilation, and total hospital expenditures. Measures ascertained during the 1-year period following birth hospitalization discharge (“long-term period”) included all-cause healthcare utilization and expenditures. Healthcare expenditures were tallied using paid amounts on corresponding healthcare claims and were expressed in 2023 US dollars. Expenditures from earlier years were adjusted using the appropriate component (e.g., hospital and related services) of the Consumer Price Index for All Urban Consumers [19].
Statistical Methods
Baseline characteristics were reported using percentages. For variables that were not considered in the 1:1 matching step, but that were considered in estimating propensity scores, the adequacy of the matching procedure was evaluated using standardized differences; a value < 0.1 was assumed to indicate a negligible difference in the characteristic between cases and matched comparators.
Study measures for cases and comparators (and corresponding differences) were summarized using means, medians, incidence proportions, and 95% confidence intervals (CIs), which were estimated using nonparametric bootstrapping techniques. Measures of all-cause healthcare utilization and expenditures following birth hospitalization discharge were adjusted for differential follow-up using a population-based approach.
Analyses were conducted for subgroups defined by clinical manifestation and pathogen. Results for meningitis and sepsis due to any bacterial infection are presented below and in the primary set of tables. Results for meningitis and sepsis due to E. coli/GBS, and all results for pneumonia, are set forth in the Supplementary Materials as causative pathogens are less commonly coded in healthcare claims, and the diagnosis of neonatal pneumonia is based on nonspecific/unique symptoms/findings and often is a diagnosis of exclusion. Only observed data were used in measuring study variables, and thus, variables were defined on the basis of the presence of specific data (e.g., diagnosis codes, procedure codes) in the study database. The absence of such data was assumed to indicate the absence of the characteristic/event captured by the variable. Analyses were conducted using SAS® Proprietary Software, release 9.4 (SAS Institute Inc., Cary, NC, USA).

Comments (0)