
Remember me
A previously developed pharmacoeconomic model has been adapted to the Spanish context to carry out a cost-effectiveness analysis of ATM-AVI ± MTZ (only for patients with cIAI) for the treatment of serious infections (cIAI or HAP/VAP) caused by suspected MBL-EB in patients with APACHE II score ≥ 8 compared with COL+MER [16].
The model compares the costs and effects of the two alternatives using:
where Costs ATM-AVI and Costs COL+MER represent the total costs associated with each therapeutic alternative, and Effectiveness ATM-AVI and Effectiveness COL+MER represent the clinical outcomes in terms of life years (LYs) and quality-adjusted life years (QALYs) for both alternatives. The incremental cost-effectiveness (ICER) and the incremental cost-utility (ICUR) ratios have been calculated and expressed as the incremental cost per LY gained or QALY gained of ATM-AVI relative to COL+MER, respectively.
The model has been developed from the perspective of the Spanish National Healthcare System (NHS), thus only direct medical costs (in 2024 €) have been included.
A lifetime horizon has been considered as differences in mortality between the therapeutic alternatives analyzed are expected.
A discount rate of 3% has been applied annually for both future costs and effects [17,18,19].
The model structure and the main inputs and assumptions considered have been validated and complemented by a multidisciplinary panel of four clinical experts. Thus, the experts’ consultation was based on a questionnaire sent and complemented by the clinical experts and a meeting to review and discuss all the assumptions and inputs included in the questionnaire that have been used to adapt the model.
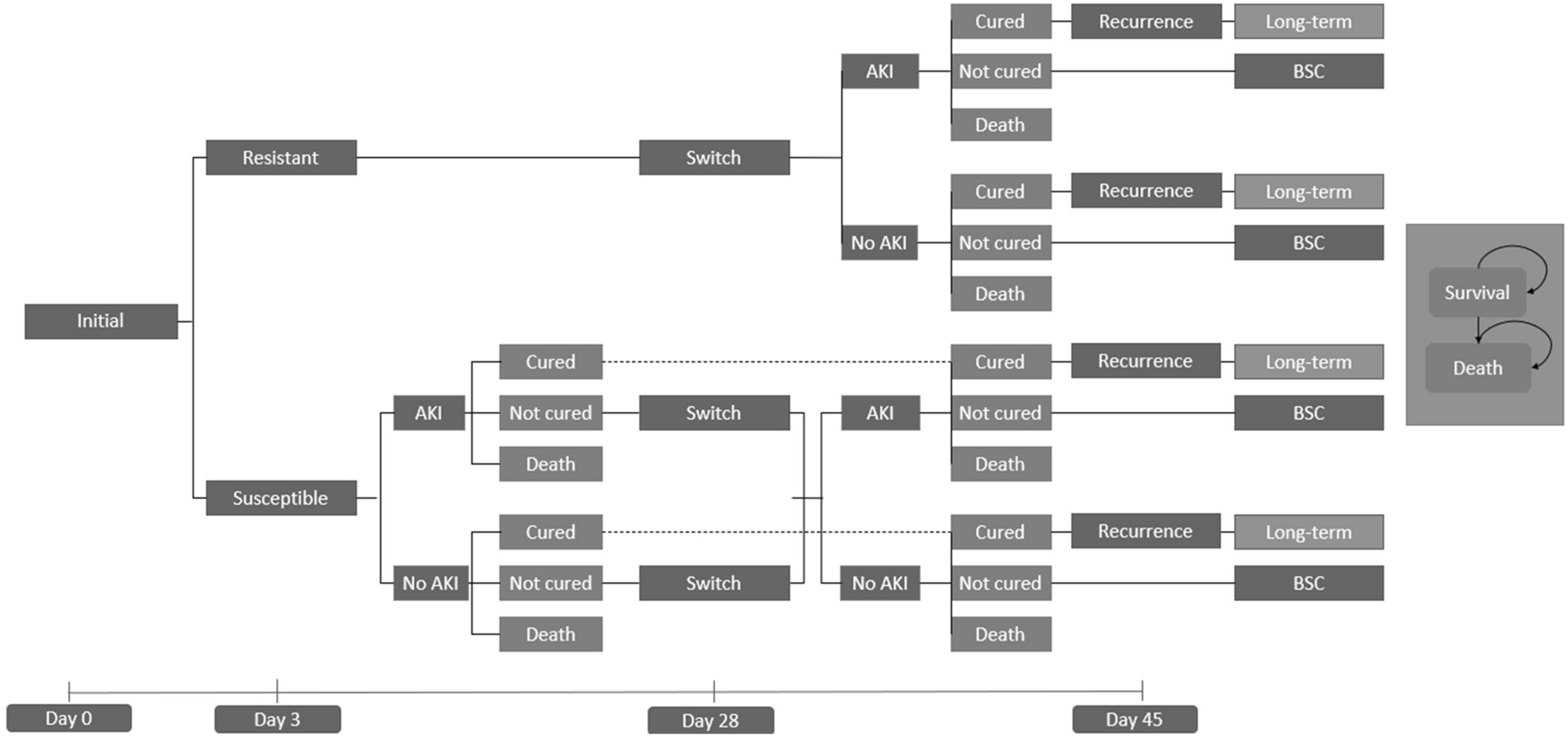
Model DescriptionThe cost-effectiveness model is structured as a decision tree model that simulates the clinical pathway of the REVISIT study for 45 days, followed by a long-term Markov model to capture lifetime outcomes (Fig. 1).
Fig. 1
Model structure. The adapted pharmacoeconomic model is composed by a tree decision model including three health states (cured, not cured and death) and a Markov model composed by two health states (alive and death). AKI acute kidney injury, BSC best supportive care
Through the decision tree model, a cohort of patients were modeled through three health states: cured, not cured, and death. Patients entered the decision tree model when they began empiric treatment with either ATM-AVI or COL+MER. At day 3, susceptible patients to empiric therapy remained on treatment until TOC on day 28, while resistant patients switched to a second-line treatment. Patients in the cured state at TOC moved to the long-term Markov model, while those in the not cured state switched to the next line of treatment and underwent a TOC on Day 14 from receiving second-line therapy. Non-responder patients after a second-line treatment are assumed to move to best supportive care (BSC).
The long-term Markov model is composed by two health states: alive and death (Fig. 1). It captures long-term survival and any ongoing costs through 1-year cycles (half-cycle correction has been implemented).
As patients treated with COL are at an especially high risk of developing nephrotoxicity (NTX) [16], this has been reflected in the model as each treatment is associated with a probability of developing NTX.
Alternatives ComparedATM-AVI was compared versus COL+MER as first-line therapy based on the REVISIT study. Patients with cIAI also received MTZ (Supplementary Material, Table S1).
Patients with resistant infections or who do not achieve cure after first-line therapy received cefiderocol as second-line treatment. Patients with cIAI who do not achieve a response at the end of treatment will require a second surgery.
Treatment regimens and durations were based on the REVISIT study and the summary of product characteristics (SmPCs) for ATM-AVI and COL+MER [11], and on the SmPCs for cefiderocol [20] (Supplementary Material, Table S1).
Both alternatives were compared and the posology considered in the model were validated by the panel of clinical experts.
Input ParametersThe parameters of the model have been divided into clinical, utility, and resource consumption and costs inputs.
Clinical InputsIn order to model patients’ transition through the decision tree model and the Markov model, different clinical inputs were defined:
Patients' baseline characteristics regarding age, proportion of females, and distribution of cIAI and HAP/VAP.
Resistance probabilities associated with the compared therapies after 3 days of treatment initiation. Resistant patients will receive a second-line treatment, and susceptible patients will continue the treatment until day 28.
Probability of cure and 28-day mortality associated with each compared therapy to model the patients to the cured (and afterwards to the Markov model), not cured, or death states.
Recurrence probability of infection.
Long-term mortality to define patients on the Markov model alive or dead.
Incidence of nephrotoxicity as a consequence of the treatments administered.
Baseline CharacteristicsBaseline characteristics for the population included in the model have been taken from the intention to treat (ITT) population of the REVISIT trial, specifically from the subgroup analysis of REVISIT considering patients with an APACHE score ≥ 8 [14]. Thus, patients with a mean age of 65.5 and 66.9 years for cIAI and HAP/VAP patients have been considered, respectively, with females 42.6% and 28.3%. This subgroup of patients has been selected for the base case as all patients specifically treated with COL+MER showed an APACHE score ≥ 8, and thus those treated with ATM-AVI with an APACHE II score ≥ 8 were selected for the comparison. Moreover, these patients better represent the real world of the Spanish clinical practice based on the experience of the clinical experts consulted.
The model estimates the ICER and ICUR for each indication analyzed separately (cIAI and HAP/VAP) or as a whole. For this purpose, the indication-specific distribution of the patient subpopulations considered in the model was estimated for the base case at 54.3% for cIAI and 45.7% for HAP/VAP [14], in line with the clinical practice in Spain.
Resistant PathogensProbability of resistance to ATM-AVI and COL+MER in the model base case has been obtained from the study published by Rossolini et al. [21] (0.6% for ATM-AVI ± MTZ and 8.9% for COL). For COL+MER, it has been validated with clinical experts that resistance to the combined therapy would be equivalent to resistance to COL. Similarly, treatment resistance rates have been assumed to be equivalent for both indications (cIAI and HAP/VAP) in the absence of indication specific data.
Based on available data, it was assumed that patients with resistant pathogens would show worse outcomes than those with susceptible pathogens, including higher mortality rates (odds ratio -OR- = 1.84), higher recurrence rates (OR = 1.49) and longer length of stay (LOS) (40% increase in hospital LOS) [22]. These ORs have been assumed to be the same no matter the indication tested. This assumption has been validated by clinical experts.
Probability of Cure and 28-Day MortalityProbabilities of cure and mortality for ATM-AVI and COL+MER have been obtained specifically from the subpopulation of patients with an APACHE score ≥ 8 [14]. Cure rates have been taken from the clinically evaluable (CE) population and mortality rates from the ITT population (Table 1).
Table 1 Treatment probability of cure, 28-day mortality, and recurrenceIn the case of cefiderocol-treated patients, cure and mortality rates have been obtained from the CREDIBLE-CR study from the population of patients with CRE infection and mortality from the population without Acinetobacter spp. infection, respectively [23].
Recurrent InfectionsRecurrence probabilities have been obtained from the APACHE subgroup analysis of the REVISIT trial (Table 1) [14].
Mortality after a recurrent infection has been considered equivalent to the mortality of COL+MER from REVISIT (6.7% and 18.2% for cIAI and HAP/VAP, respectively) [14].
Long-Term MortalityMortality in the long-term Markov model has been informed by general population life tables for Spain [24].
A hazard ratio (HR) based on the Charlson Comorbidity Index (CCI) score has been applied to the general population mortality [25] based on the percentage of patients in each CCI score category [26] (Table S2) to capture the increased risk of death due to the history of being infected by Gram-negative pathogens. Both CCI distribution and the associated HR applied to general population mortality have been validated by the panel of clinical experts.
Thus, even though comorbidities were not explicitly modeled as separate variables, the model incorporates long-term mortality adjustments using the CCI and HR. Additionally, the REVISIT trial population included an heterogenous group of patients with varying comorbidities, which are indirectly reflected in the efficacy and mortality outcomes used in the analysis.
NephrotoxicityThe NTX rate for ATM-AVI (1.9%) has been obtained from the subpopulation of patients in the REVISIT study with an APACHE score ≥ 8 [14] (Pfizer Clinical Study Report. Data on file). Nevertheless, given the limited sample size of the COL+MER arm in the REVISIT subgroup analysis [14], the NTX incidence for COL was sourced from a broader systematic review, in which 33.0% of patients treated with COL were reported to suffer from it [27] to provide a more stable and generalizable estimate.
NTX has been associated with an additional length of hospital stay, renal replacement therapy (RRT) and loss of quality of life in the short-term, and chronic RRT and loss of quality of life in the long-term. The proportion of patients requiring RRT has been derived from a previously published cost-effectiveness analysis [28], in which 5.2% of the patients required short-term RRT, while 2.4% required long-term RRT. A mortality risk of 0% associated with NTX has been considered, as it is assumed that this would be captured in the mortality rate considered for the 28-day time horizon. All data points/assumptions related to NTX have been validated with clinicians.
Utility InputsUtility values are used to represent the impact on quality of life associated with a particular health state, on a scale ranging from 0 (death) to 1 (perfect health).
The adapted model considers utilities associated with the included health states, with the development of NTX or recurrence, and utility values of the general population.
The utility of patients achieving clinical response or cure has been considered equivalent to that of the age-adjusted general population of Spain [29, 30].
Utility values for patients with cIAI and HAP/VAP who did not achieve clinical cure have been obtained by weighting the mean time spent in general ward or intensive care unit (ICU) reported in the REVISIT study and the utilities associated with the hospital stay [31,32,33,34].
Disutility associated with suffering a recurrence has been assumed to be the difference between the utilities of cured versus uncured patients.
The utility values of the long-term Markov model are based on the utility values of the Spanish general population [29, 30] (Table 2).
Table 2 Utility and disutility valuesDisutility associated with NTX has been derived from the study developed by Simon et al. [28], which has been calculated as the difference between the utility associated with NTX and hospitalization (Table 2).
Disutility associated with chronic dialysis has been estimated as the difference between the utility of chronic dialysis [35] and the cured state [29, 30] (Table 2).
Resource Consumption and Cost InputsThe analysis was conducted from the perspective of the Spanish NHS, consequently only direct clinical costs (in 2024 €) were considered.
Treatment CostsDrug unit costs have been expressed as ex-factory list prices, considering, when applicable, deductions established in Royal Decree-Law 8/2010 [36, 37] (Table 3). To estimate the pharmacological cost of each therapeutic alternative analyzed in the model, the dosages included in the REVISIT trial (Table 3) and mean treatment durations reported for the total population in each indication have been considered [13]. For cefiderocol, considered as a second-line treatment in the model, dosage and treatment duration has been obtained from its SmPC [20].
HospitalizationInpatients may be admitted to ICU or general ward. Hospitalization costs have been calculated as a weighted average of the ICU costs and general ward costs using time spent in each location (Table 3).
Recurrence and Secondary SurgeryRecurrence costs have been modeled as a one-off cost at the time of recurrence. It has been assumed that the same level of medical management is required to manage the recurrences regardless of the treatments analyzed for the initial infection episode. Recurrence costs are based on length of ICU or hospital general ward stay for each indication based on the REVISIT study, and the corresponding unit costs have been applied, obtaining a cost of €10,794.3 for cIAI and €29,866.1 for HAP/VAP [31, 38].
The cost of secondary surgery is assumed to be the same as the cost of recurrence of cIAI.
NephrotoxicityWhen patients experience NTX, additional hospital days have been factored in, based on whether the patient needs RRT (5.2 days) or not (2.3 days), as reported in the study by Simon et al. [28]. It has also been assumed that patients requiring RRT will undergo dialysis every other day for the duration of the extended stay due to NTX (2.6 days) (Table 3).
Best Supportive CareFor patients that are not cured after two lines of treatment, the model assumes 1 week of survival under BSC. Patients are assumed to remain in hospital stay for the duration of the BSC period, and the cost of general ward days has been used to inform this cost.
Sensitivity AnalysesTo assess the uncertainty of the variables considered in the model and determine the robustness of the results, deterministic (univariate and alternative scenarios) and probabilistic sensitivity analyses have been conducted.
Univariate sensitivity analysis has been carried out to test the uncertainty of the parameters included in the model independently over a plausible range defined by either the 95% confidence interval (CI) or ± 20% where no estimates of precision were available.
Additionally, different alternative scenarios have been studied to evaluate the uncertainty regarding some assumptions considered in the model.
Furthermore, a probabilistic sensitivity analysis (PSA), with a total of 10,000 Monte Carlo simulations have been carried out exploring joint parameter uncertainty based on different distributions (Table S3).
Ethical ApprovalThis article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Comments (0)