Describing community-acquired pneumonia for a specific country is important because its epidemiology, clinical presentation, and outcomes can vary significantly by region due to factors like: local pathogen prevalence, antibiotic resistance patterns, health care infrastructure and access, population demographics, environmental and lifestyle factors and vaccination policies. This study presents the most recent comprehensive overview of CAP in Switzerland. Our primary findings were: (1) mortality rates were lower in our study compared to previously reported data; (2) molecular testing of sputum and BAL improved pathogen detection; and (3) S. pneumoniae remained the predominant pathogen overall, while H. influenzae was most frequently identified in immunocompromised patients.
First, the 28-day and 180-day mortality for the overall cohort as well as for the patients who required ICU admission were lower than rates reported in other studies: a retrospective analysis of a healthcare claims database in Germany reported 30-day mortality rates ranging from 2.8% in adults under 60 years of age to 26.8% in those over 60 with severe comorbidities [18]. In a previous CAPNETZ study, the overall mortality at 30 days was 5.5% [19]. In a Spanish single-center study, the 30-day mortality was reported to be 4.1% for non-ICU CAP, and 12% among those requiring ICU admission [4]. For severe CAP, 30-day mortality rates of 27% were reported in a study from the United States, while another Spanish study documented a rate of 33% [6, 7]. Compared to these studies, our cohort was relatively young (mean age 63.1 years), yet a large majority (76.4%) of participants had at least one documented comorbidity. These comparatively low mortality rates may reflect Switzerland’s well-resourced healthcare system, characterized by universal coverage, rapid access to care, and high availability of medical and ICU resources, which facilitate early diagnosis and timely treatment [20]. A strong primary care network also supports coordinated post-discharge management. Additionally, the Swiss population, particularly in German-speaking regions, tends to have favorable health behaviors, including lower smoking and alcohol consumption and higher physical activity levels [21]. At the same time, vaccination coverage against influenza and pneumococcus remains low in Switzerland: only 14% for influenza (36% in individuals ≥ 65 years) [22] and 4.5% for pneumococcus overall (9.6% in individuals ≥ 65 years, 27.1% in individuals with immunosuppression) [23]. A major reason is that at the time of the study, in adults PCV13 was recommended for persons at risk (but not for age as an independent risk factor) [24] but not licensed for adults and therefore not reimbursed, which may partly explain these low rates. Thus, while high healthcare quality and a generally healthy population may have contributed to lower mortality, limited vaccine uptake suggests potential for further improvement in the prevention of CAP.
Mortality was significantly higher during the COVID-19 pandemic compared with the pre-pandemic period, both among patients with CAP with and without documented SARS-CoV-2 infection. Interestingly, national data from Switzerland showed that hospital mortality rates for patients hospitalized with pneumonia during 2020–2021 were only marginally higher than during 2015–2019 [25]. During the first two years of the pandemic, the incidence of hospitalizations for acute exacerbations of COPD (AECOPD) and non–COVID-19 pneumonia markedly decreased in Switzerland, likely reflecting the impact of widespread social distancing and infection control measures [25]. Although overall hospital admissions declined, those who were hospitalized tended to present with more severe disease, which may explain the modestly increased in-hospital mortality observed during this period. Switzerland experienced an excess mortality in 2020 comparable to that of other European countries, with the highest peaks during the second wave (November–December 2020) and marked regional variability [26]. The regions of Basel and St. Gallen, where participants for our cohort were recruited, were less affected than others. Comparative data between Germany and Switzerland suggest that Swiss hospitals had lower mortality and ICU admission rates for severe acute respiratory infections, potentially reflecting differences in healthcare system capacity, ICU bed availability, and hospitalization criteria [27]. These contextual factors may partly explain why mortality rates in our cohort, and in Swiss national data, appeared relatively lower than those reported from some other European cohorts. Switzerland’s healthcare system maintained relatively high ICU capacity and avoided major periods of system overload, which likely mitigated mortality. It is also important to note that immunosuppressed patients were included in our study only from January 2020 onward, and mortality was highest among patients with malignancies or severe immunosuppression. Therefore, part of the observed increase in mortality may be attributable to the inclusion of these high-risk patients. Further investigation into the interplay between SARS-CoV-2–related risks, healthcare resource pressures, and organizational changes during the pandemic was beyond the scope of this study. Nonetheless, our findings support that much of the mortality associated with CAP during the pandemic reflects underlying comorbidities and immunosuppression rather than a direct effect of healthcare system strain [28].
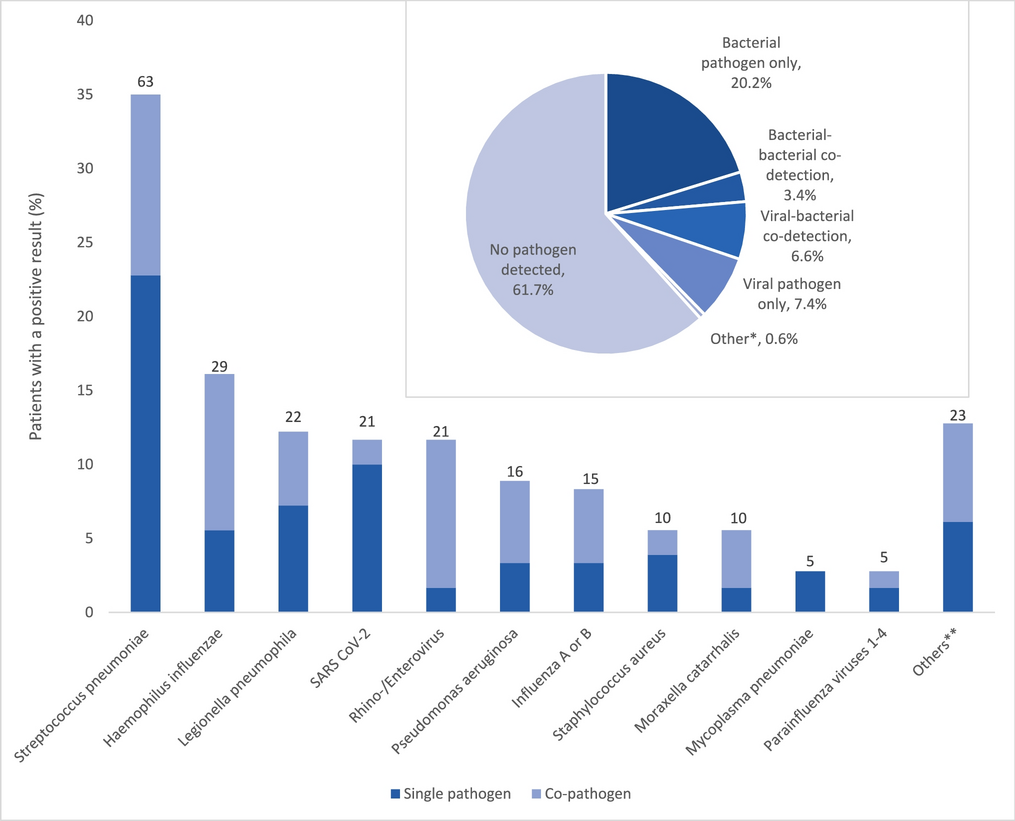
Second, a pathogen was identified in roughly a third of patients (38.3%), which corresponds to previously published findings [14, 29, 30]. The highest diagnostic yield for pathogen identification was achieved by sputum culture, especially if collected before the initiation of antibiotic therapy, and although information on the quality of sputum sampling is lacking in many patients. This confirms prior studies highlighting the yield of appropriate sputum culture as a neglected but affordable diagnostic tool [31,32,33]. Sputum culture has been shown to correlate well with BAL fluid [34, 35]. However, sputum was only performed in less than a quarter of patients in our study. Thus, we postulate that higher pathogen identification rates could be achieved by performing sputum culture more frequently. Alternatively, patients with sputum production and thus prone to providing sputum for examination might carry a higher microbiological load or simply diagnostic access to the site of infection [32, 36]. If negative, BAL, including molecular testing for respiratory viruses, likely improves etiologic diagnosis in CAP. The utility of obtaining specimens for microbiological testing is an ongoing matter of debate and is recommended in patients with severe CAP and patients with immunosuppression [2, 37]. Molecular testing of lower respiratory tract samples increases pathogen detection compared with culture (39–63% vs. 71–87%) [12, 38, 39], although PCR cannot distinguish viable organisms from residual nucleic acids [40]. Despite this limitation, molecular diagnostics markedly shorten the time to pathogen identification, enabling earlier transition from empirical to targeted therapy [39, 41] and reducing unnecessary broad-spectrum antibiotic exposure [42]. This facilitates more effective antimicrobial stewardship through timely de-escalation without compromising patient safety, with studies showing no increase in adverse events, ICU transfers, or recurrence compared with conventional management [42, 43]. Although some reports suggest shorter hospital stays with molecular-guided therapy [44, 45], pooled analyses have not confirmed a significant reduction [46]. Overall, integrating molecular testing into CAP management supports more precise and individualized empirical therapy decisions while strengthening antimicrobial stewardship.
Third, S. pneumoniae was the most frequently identified pathogen in our study, followed by H. influenzae. In contrast, two recent Scandinavian studies [12, 47] identified Haemophilus as the most prevalent pathogen, surpassing S. pneumoniae. In our cohort, this was particularly evident among patients with severe immunosuppression, where Haemophilus emerged as the predominant pathogen, while S. pneumoniae was not detected. Haemophilus also exhibited the second-highest mortality rate in our study, exceeded only by SARS-CoV-2. This elevated mortality may be attributed to the frequent involvement of H. influenzae in bacterial-viral coinfections, which are known to be associated with worse clinical outcomes [48, 49]. There is variability across studies regarding CAP mortality rates by pathogen [4, 50, 51]. However, the 2016 Global Burden of Disease study identified S. pneumoniae as the leading cause of mortality in LRTIs [52]. Introduction of pneumococcal conjugate vaccines in childhood vaccination programs has been linked to decreased case-fatality rates from invasive pneumococcal disease even in adults [53, 54]. These findings have important implications for the empirical antibiotic therapy recommendations for CAP and underscore the need for tailored approaches in immunocompromised populations.
It is important to note that antibiotic treatment prior to bronchoscopy likely reduced BAL culture sensitivity for causative pathogens. In addition, antibiotics may alter upper airway flora [55] that can be carried into the lower airways during bronchoscopy. In hospitalized patients, these effects, together with antibiotic exposure, may contribute to increased detection of Gram-negative organisms, potentially explaining the relatively high rates of Pseudomonas aeruginosa and Staphylococcus aureus identified in our cohort.
Our study has several limitations. Due to its prospective design, which required patient consent, a disproportionately larger number of hospitalized patients—and potentially less acutely ill patients—were included. Consequently, this cohort may not fully represent the entire population of community-acquired pneumonia (CAP) patients in Switzerland, where primary healthcare is robust and many CAP cases are managed by General Practitioners on an outpatient basis. Additionally, the requirement to obtain informed consent in this prospective study led to a selection bias, as previously described in other CAPNETZ studies [19]. This is reflected by relatively low CRB65 scores in patients, even those admitted to ICU. Furthermore, this most likely explains the comparatively low mortality rate in our cohort.
Moreover, CAPNETZ represents a convenience sample, as patient inclusion depended on available study staff and resources rather than systematic recruitment of all hospitalized CAP cases. Consequently, only a subset of eligible patients was enrolled. While this may limit representativeness, it reflects the real-world feasibility of long-term, resource-dependent patient recruitment across participating centers.
Finally, the cohort evolved over time with the inclusion of a second study center in 2017, adding variability but also broadening the scope of the study. Furthermore, diagnostic testing was performed at the discretion of the treating physicians rather than according to a standardized study protocol. Although this could have led to variability in pathogen detection rates, it also reflects real-world clinical practices, providing insights into typical CAP management within healthcare settings and enhancing the study's relevance to everyday clinical decision-making. Notably, 98.3% of participants had at least one specimen type available for bacterial and/or viral testing, forming a solid basis for assessing pathogen distribution even with varied testing approaches.
Focusing predominantly on hospitalized cases allowed the study to capture the types of cases that impose the most substantial burden on healthcare resources, enabling a focused analysis of critical aspects of CAP management in a hospital context. The inclusion of immunocompromised patients and extensive molecular workups broadened the scope and strengthened the generalizability of the findings, providing insights from a diverse population and reflecting local pathogen profiles and resistance patterns.
In conclusion, although lower than in other countries, mortality rates of CAP remain high in Switzerland. Pathogen identification rates are low, yet molecular testing of sputum and BAL seems to enhance pathogen detection in hospitalized patients with CAP. Haemophilus influenzae emerged as the most frequently detected pathogen in immunocompromised patients, a finding that should be taken into consideration when developing therapy guidelines for this population.


Comments (0)