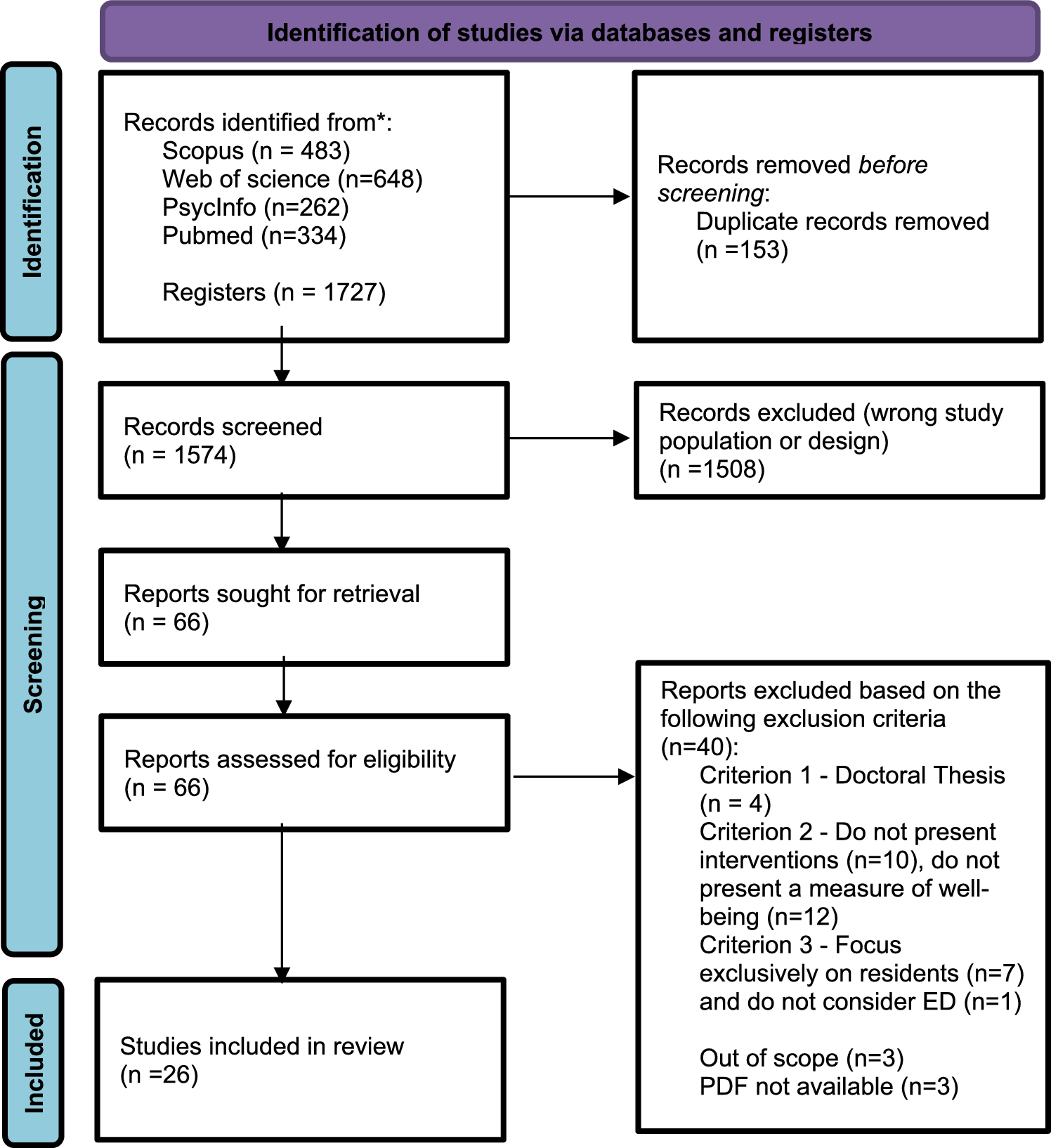
The search process is summarized in the PRISMA flow diagram (Fig. 1). A total of 1,727 records were identified through database searches. After removing duplicates, 1,574 articles were screened by title and abstract. Of these, 1,508 were excluded for not meeting the inclusion criteria, primarily due to ineligible populations or study designs. After full-text assessment, 26 studies published between December 2021 and 2024 were included in the final analysis. The substantial heterogeneity in study designs, methodology, participant characteristics, intervention types, and outcome measures made direct comparisons difficult and precluded the possibility of conducting a meta-analysis.
Study characteristics
The included studies were primarily conducted in the United States (n = 5), Iran (n = 5), Canada (n = 3), and the Netherlands (n = 2). Sample sizes ranged from 14 to 578 participants. Twelve studies focused exclusively on nurses, six on broader ED staff (including administrative and allied health professionals), four on physicians alone, and four included both nurses and medical staff with two also including residents. In terms of study design, seventeen studies were classified as quasi-experimental, meaning they involved an active intervention without random allocation of participants. These included designs such as one-group pre-post evaluations and post-test-only formats, reflecting pragmatic approaches to studying real-world healthcare settings. Seven studies were randomized controlled trials (RCTs), which involve the random assignment of participants to intervention or control groups and are considered the gold standard for minimizing bias. One study used a mixed-methods approach, integrating both qualitative and quantitative data to examine outcomes from multiple perspectives. The dominance of quasi-experimental designs highlights the practical and ethical challenges of conducting randomized trials in emergency department environments. Nonetheless, several of these studies demonstrated strong methodological quality through careful design, use of control groups, and comprehensive reporting of outcomes, supporting their value within the evidence base despite the lack of randomization.
All studies used self-reported psychometric instruments to measure outcomes. Burnout was the most frequently assessed variable (n = 9), often in combination with job satisfaction [21, 22], stress [23, 24], anxiety [25], work engagement [26], or turnover intention [27]. Stress was measured in seven studies, one of which also included physiological parameters [28]. Other outcomes included anxiety and depression [30, 31], moral sensitivity and caring behaviors [31], and subjective evaluations of the intervention [33, 34]. Overall, 18 studies reported significant improvements in well-being outcomes at post-intervention (T2). However, only six studies included a follow-up phase to assess long-term effects (T3).
Intervention types
The review identified a variety of interventions classified according to the level at which they operate, following the framework proposed by Xu et al. [51]. Organizational-directed interventions aim to modify organizational factors or introduce policy and procedural changes to improve the working environment. Examples cited by Xu et al. [51] include adjustments to shift schedules and/or reductions in working hours or workloads. Individual-focused interventions are designed to strengthen personal coping abilities or stress-management skills. These interventions target the single healthcare professional and include strategies such as mindfulness programs or psychological training. Group-level interventions focus on teams or work units, promoting practices such as peer support or structured debriefings. Finally, multilevel interventions integrate components across individual, group, and/or organizational domains, aiming for a more systemic and comprehensive impact on staff well-being (Table 1).
Table 1 Characteristics of the studies included in the reviewMost studies included in this review (n = 21) implemented individual-level interventions, one study employed a group-level approach, two focused on organizational-level interventions, and two adopted multilevel strategies.
Individual-level interventions
Among the 21 studies using individual-level approaches, interventions were classified as either educational (n = 12) or mindfulness-based (n = 9).
Educational interventions
Educational interventions varied in content, delivery, and duration. Five studies focused on resilience training [31, 35,36,37,38]. In particular, in Hasani et al. [38], a resilience training program was delivered through eight 45-min sessions held twice weekly, aiming to reduce stress among nurses. Similarly, in the study by Arbuzia et al. [34], the intervention group received eight 30-min sessions of resilience training over two months, while the control group received no intervention. Two other studies focused on aggression management training [22, 39]. In particular, the quasi-experimental study by Masa'deh et al. [38] introduced both verbal and non-verbal communication techniques designed to help healthcare professionals de-escalate aggressive behavior. One study examined skill training focused on enhancing moral sensitivity and caring behaviors [31]. Another implemented a coaching program aimed at reducing burnout and turnover intentions [27], while a further study evaluated a mentorship initiative addressing career development, academic advancement, emotional well-being, and professional growth for physicians [39]. Additional interventions included a debriefing workshop [40] and a burnout reduction program [22]. The duration of interventions ranged from 3 weeks [31] to 7 months [40], with the majority (n = 9) lasting between 2 and 6 months. All studies included post-intervention outcome assessments, and three incorporated follow-up evaluations at a third time point (T3) [23, 32, 38]. Seven studies reported significant improvements in well-being outcomes—such as moral sensitivity, stress, and burnout—following the intervention. However, among the studies with follow-up, only one [37] demonstrated sustained long-term effects, whereas in another [22], the initial reduction in burnout was not maintained at the 3-month follow-up.
Mindfulness-type interventions
Eight studies focused on mindfulness-type interventions, while one employed an app-based cognitive behavioral therapy (CBT) program. The CBT intervention provided personalized sleep advice from specialists and encouraged self-reflection using data from fitness trackers and daily well-being questionnaires [41]. The mindfulness-type-type interventions varied considerably in terms of intensity, delivery methods, and duration across studies. Some were app-based [25, 26], while others used virtual reality (VR)–guided meditations accessed via a VR headset, or a standalone mobile app located in the emergency department (ED) on-call room [42]. Several interventions incorporated mindfulness practices in combination with breathing exercises, meditation, yoga/stretching, and relaxation techniques, which were designed to be practiced during work shifts and included all ED staff, including administrative personnel [43]. In terms of duration, four studies implemented the intervention over four weeks, two lasted three months, one was conducted over eight weeks, and another was nearly one weeklong. Most studies (n = 7) reported positive effects on healthcare workers’ well-being, primarily through reductions in burnout and stress, as well as improvements in sleep quality (n = 5). One study also assessed anxiety levels alongside burnout following the intervention [25], while another reported increased job satisfaction and reduced fatigue [44]. Additionally, one study monitored physiological changes such as heart-rate variability (HRV) and a relaxation biomarker, which were measured during each mindfulness session [42]. Two studies explored participants' perceptions of the intervention using semi-structured interviews, thus assessing effectiveness qualitatively rather than quantitatively [33, 34]. One study reported no significant change in outcome scores pre- and post-intervention. Notably, most studies assessed outcomes immediately after the intervention. Only four included a follow-up at a later time point (T2), and one study extended the evaluation to a third time point (T3), three months post-intervention [24].
Group-level interventions
One study adopted a group-level intervention [29]. In this case, the group setting was used as a vehicle for promoting change. Specifically, Connors et al. [29] conducted a pilot study to assess the feasibility, receptivity, and preliminary effectiveness of peer support groups in addressing anxiety, depression, distress, and burnout among ED physicians. The intervention consisted of eight weekly online peer support sessions. Each session began with a brief 2- to 3-min check-in, allowing participants to share their current experiences. This was followed by a group discussion focused on common and urgent issues and concluded with the sharing of positive action plans or inspirational reflections. The groups were facilitated by a non-clinician peer support leader and one of three trained emergency medicine physician co-facilitators.
Organizational-level interventions
Two studies implemented organizational-level interventions [29, 47], both involving modifications to the physical work environment. Specifically, these interventions exposed staff to various types of music or natural sounds during work breaks or shifts. For instance, in the study by Fattahpour et al. [46], a music player was used for 60 min at the beginning and end of each shift, playing nature sounds, such as a blend of bird songs and waterfall audio—selected from a dedicated sound database. Calamassi et al. [28] examined the effects of listening to music during work breaks, comparing it to routine breaks without music, in reducing stress and anxiety levels among ED nurses.
Although these interventions did not target traditional organizational aspects such as workload, work shifts, or task structure, they introduced a change in the physical work environment—namely, the presence of different types of music during shifts or breaks. Therefore, these interventions directly influenced the physical work context in which ED’s staff operate and thus we classified them as organizational-level interventions.
Multilevel interventions
This review identified two studies that implemented multilevel interventions [27, 46]. In the study by De Wijn et al. [26], a multilevel intervention was developed based on a comprehensive risk assessment and targeted both individual and organizational levels. The process began with a well-being survey and semi-structured interviews to identify key risks and gather contextual insights. This was followed by inspiration sessions to build knowledge, culminating in a management report with tailored recommendations. A Psychosocial Safety Climate (PSC) intervention was subsequently implemented. Organizational strategies included increasing the number of emergency department (ED) nurse trainees and support staff, scheduling medical specialists during peak hours, reorganizing patient flow by creating low- and high-care units, and enhancing security measures, such as installing staff-only access doors. At the individual level, the intervention introduced psychoeducation on burnout, coaching to enhance team communication, work shift adjustments to allow for rest, and the implementation of self-rostering to increase scheduling autonomy. The intervention spanned 2.5 years and incorporated both pre-post measures and follow-up assessments. In terms of outcomes, most job-related factors improved, with the exception of autonomy, which showed only a temporary increase. Notably, work engagement declined, and burnout levels remained stable.
The second study, conducted by Yang et al. [45]], implemented a multilevel intervention during the COVID-19 pandemic, using an action research approach. The process involved online surveys and group brainstorming to assess stress levels among ED nurses. The survey, based on a COVID-19-specific stress questionnaire, examined the sources and intensity of stress as well as nurses’ needs. Intervention strategies, developed over two iterative cycles, addressed three main areas: (1) infection protection (e.g., ultraviolet disinfection, personal protective equipment, health screenings), (2) workload reduction (e.g., training for junior nurses, shift limitation, increased staffing), and (3) body-mind-social well-being (e.g., meal delivery, bonus incentives, improved communication, and a more supportive work environment) [45].It is important to note that this intervention was implemented in the specific context of the COVID-19 pandemic, and its strategies may not be easily transferable to other settings or periods. Nevertheless, multilevel interventions, though limited in number, tend to be supported by more robust research designs and reflect a greater emphasis on contextual adaptation and implementation processes. First, thorough preliminary assessments help ensure that interventions are tailored to the specific needs of participants. Second, these interventions often extend over longer periods, such as in De Wijn et al. [26], allowing more time for stakeholder engagement and transparent communication, which can reduce resistance to change and improve implementation success.

Comments (0)