
Remember me
Among the 158 geriatric patients admitted to the rehabilitation unit, the median age was 84 years (IQR 77–88), with a predominance of female patients (70.8%). The median length of stay was 40 days (IQR 22–67). For comparative analyses, patients were stratified into age tertiles: the youngest group (T1-age) included individuals aged ≤77 years, the intermediate group (T2-age) those aged 78–87 years, and the oldest group (T3-age) those aged ≥88 years. Demographic and clinical characteristics according to age tertiles are presented in Table 1.
Table 1. Patient characteristics stratified by age tertilesFemale sex was more prevalent in older age groups. Cognitive function, assessed with the MMSE, progressively declined with age (median 26.0 in T1 vs. 23.4 in T3; p = 0.0095), and BRASS scores increased, indicating greater discharge complexity (median 19.0 in T1 vs. 23.0 in T3; p < 0.0001). Comorbidity burden (CIRS-IC and CIRS-IS) and frailty index did not significantly differ across age groups, as well as the frailty index (median 0.6 in T1 vs. 0.7 in T3; p = 0.1007). Functional status at admission worsened with increasing age, with higher Hendrich II scores (median 4.0 in T1 vs. 5.0 in T3; p = 0.0360), lower Barthel Index scores (median 32.0 in T1 vs. 16.0 in T3; p = 0.0002), and lower Tinetti Scale scores (median 11.0 in T1 vs. 5.0 in T3; p = 0.0544). Polypharmacy (defined as the use of >5 drugs) was highly prevalent and comparable across age groups.
Sex stratification of the patient population showed that females were significantly older (median 84 vs 79 years, p = 0.0045) and exhibited higher frailty index scores (0.7 vs 0.6, p = 0.0165). Women also showed lower Barthel Index and Tinetti Scale scores, indicating reduced functional autonomy and mobility (p = 0.0052 and p = 0.0035, respectively). No sex differences were observed in MMSE, CIRS-IC, CIRS-IS, or Hendrich II scores (Supplementary Table 1).
Association of age with baseline functional parametersTo better understand the impact of chronological age on functional status at admission, we examined its independent association with performance scores after adjusting for sex and frailty index. In multivariable linear regression models adjusted for sex and frailty index, age was independently associated with Barthel scores (β = −0.65 per year; 95% CI −0.93 to −0.36; p < 0.001), but not with Tinetti or Hendrich scores. Frailty index showed a strong and consistent association with all functional outcomes: Tinetti (β = −39.9, p < 0.001), Barthel (β = −89.9, p < 0.001), and Hendrich (β = 6.8, p < 0.001). Sex was not significantly associated with any functional score (Table 2).
Table 2. Multivariable linear regression analysis evaluating the association between age, sex, and frailty index and functional outcomes (Tinetti scale, Barthel Index, and Hendrich II score) at hospital admissionWhen comorbidity burden (CIRS-IC) was included as an independent variable in the model, with frailty index and sex as covariates, it was significantly associated only with Tinetti scores (β = 8.51, 95% CI 5.73–11.30, p = 1.9 × 10⁻⁸), indicating that higher comorbidity burden predicted poorer balance and gait performance (Supplementary Table 2). Cognitive function (MMSE), entered as an independent variable with the same covariates, was not significantly associated with any of the functional outcomes (Supplementary Table 3).
Impact of age on rehabilitation outcomesTo evaluate whether age influenced rehabilitation trajectories, we compared functional outcomes between the youngest (T1-age) and oldest (T3-age) tertiles. As expected, the T3-age group showed significantly worse baseline scores across all domains (Fig. 1A–C, upper panels), confirming that advanced age was associated with higher functional impairment, increased fall risk, and reduced autonomy and mobility at admission.
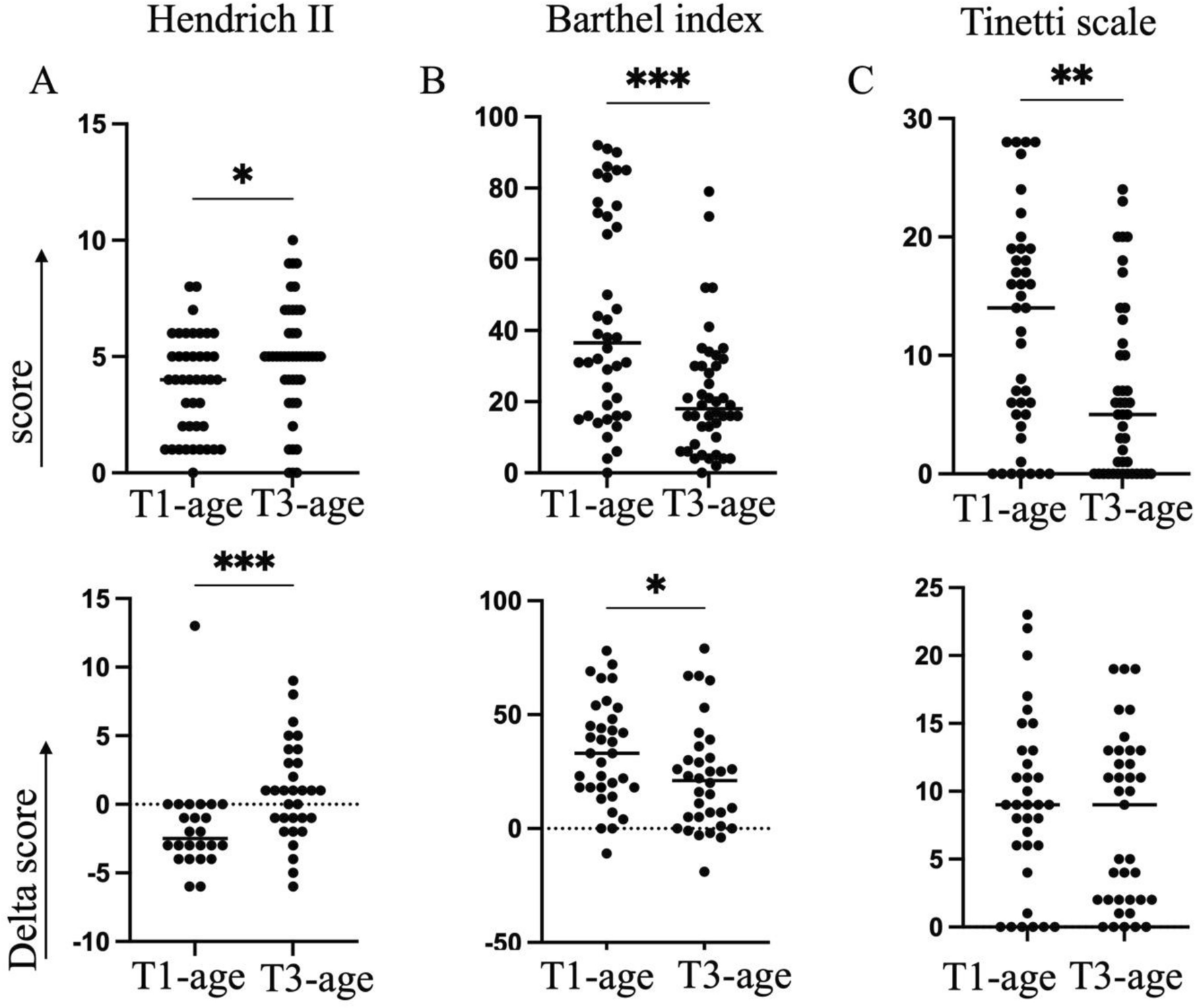
Fig. 1
Geriatric assessment scores at hospital admission and changes during rehabilitation by age tertiles. Panels A–C (upper): Baseline scores at admission for the Hendrich Fall Risk Model (A), Barthel Index (B), and Tinetti Scale, sum of balance and gait, (C) in the youngest (T1-age) and oldest (T3-age) tertiles. Panels A–C (lower): changes in scores from admission to discharge (Delta score = discharge—admission) for each assessment tool in the T1-age and T3-age groups. Each dot represents an individual patient. Horizontal dashed lines indicate no change following rehabilitation. p values were calculated using the Mann–Whitney U test
Analysis of score changes from admission to discharge revealed age-dependent responses to rehabilitation (Fig. 1A–C, lower panels). At discharge, Hendrich II scores remained elevated in the T3-age group compared to T1-age patients, indicating a persistently high fall risk despite the completion of rehabilitation (Fig. 1A, lower panel). Although Modified Barthel Index scores improved in both groups, the magnitude of improvement was significantly smaller in the T3-age group, suggesting more limited recovery of functional autonomy (Fig. 1B, lower panel). In contrast, Tinetti Scale scores improved substantially and to a similar extent in both age groups, indicating that mobility is responsive to rehabilitation regardless of age (Fig. 1C, lower panel). To further assess the impact of age on motor recovery, we analyzed the two subcomponents of the Tinetti Scale: balance and gait. At admission, patients in the T3-age group exhibited significantly lower scores in both domains compared to those in the T1-age group, with a median balance score of 5 versus 8.5 and a median gait score of 2 versus 7.5, respectively, indicating marked impairment, particularly in gait function (Supplementary Fig. 1 A, B). By discharge, both balance and gait scores improved significantly in both groups. Notably, the improvement in gait performance was particularly pronounced, with a median delta of 3.8 in T1-age and 4.5 in T3-age, suggesting that age did not limit the capacity for gait recovery.
Baseline functional scores predict post-rehabilitation outcomesBaseline functional scores (at admission) were tested as predictors of post-rehabilitation outcomes (Supplementary Table 4). Higher Tinetti scores at admission were significantly associated with higher scores at discharge (β = 0.58, 95% CI 0.45–0.71, p = 5.6 × 10⁻15). Similarly, higher Barthel Index scores at baseline strongly predicted better functional recovery (β = 0.87, 95% CI 0.68–1.06, p = 5.3 × 10⁻15). Baseline Hendrich II scores were also significantly associated with post-rehabilitation scores, although with a weaker effect size (β = 0.31, 95% CI 0.08–0.54, p = 0.0095). These findings highlight the central role of baseline functional status in predicting rehabilitation outcomes.
Assessing malnutrition as a determinant of fall riskBy the end of the rehabilitation program, the risk of falls—as measured by the Hendrich II score—remained significantly higher in the older cohort. To investigate potential contributors to this persistent vulnerability, we examined whether malnutrition could explain the incomplete recovery of fall risk. Nutritional status at admission was assessed using the Malnutrition Universal Screening Tool (MUST) [18]. Results were comparable between age groups: only three patients in each group had a MUST score ≥2, indicating high risk of malnutrition (Supplementary Fig. 2). These findings suggest that malnutrition alone is unlikely to explain the sustained fall risk observed in the oldest patients.
Comments (0)