
Remember me

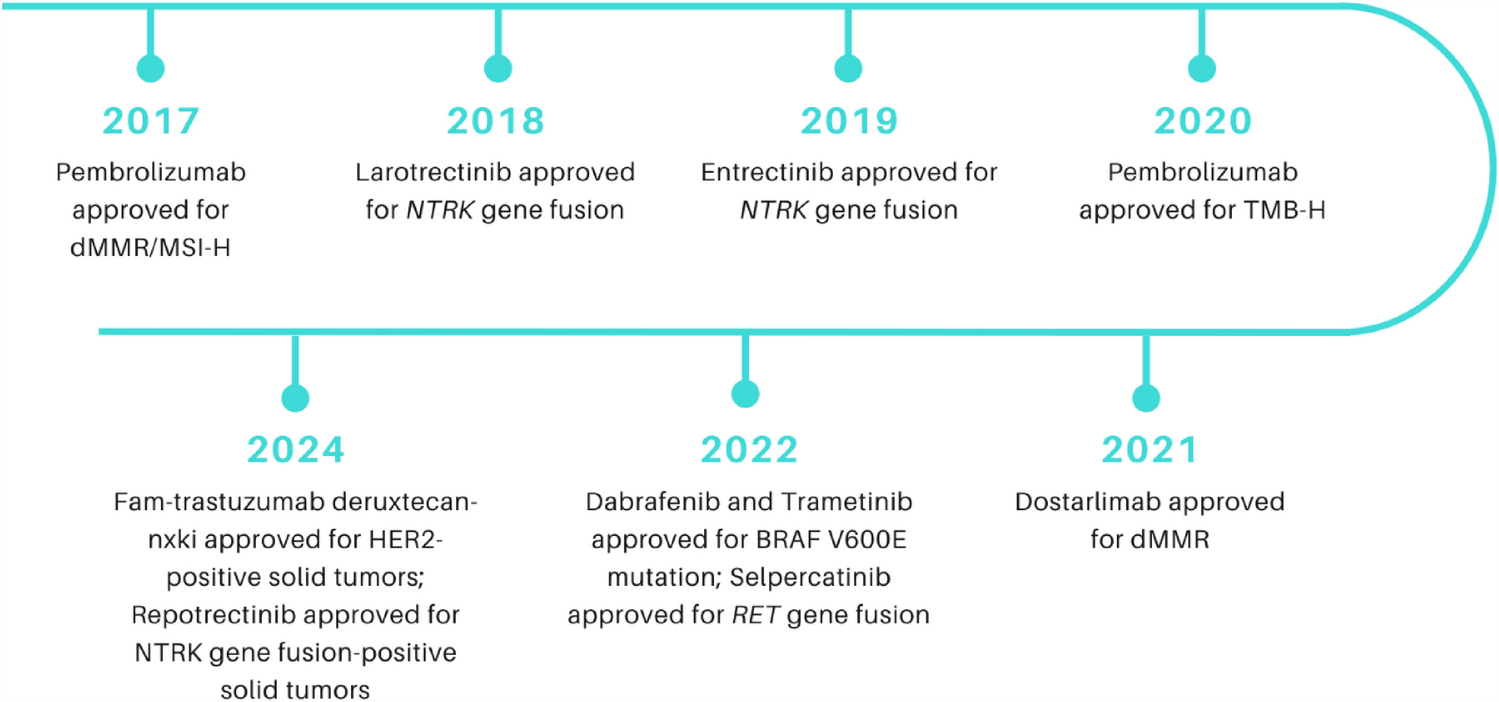
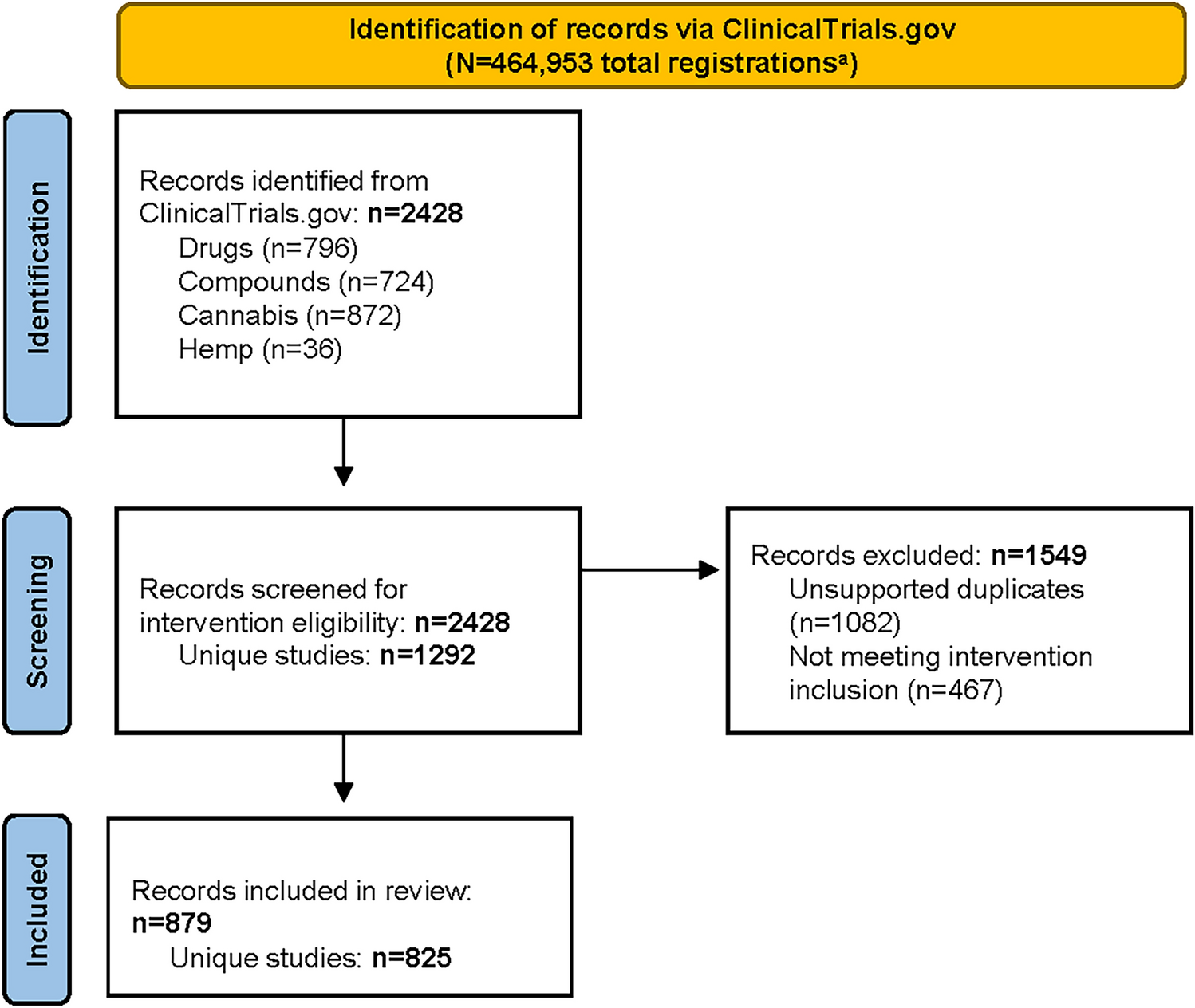
Since 2017, eight different drugs have received nine FDA-approved tissue-agnostic cancer indications (Fig. 1). Among the clinical trials supporting these approvals, seven have since published updated results specific to patients with lung cancer [14,15,16,17,18,19,20]. In addition, we identified two post-approval trials and one retrospective analysis pooling data from 12 trials. Lung cancer-specific cohorts across these studies ranged in size from 4 to 247 patients. The primary efficacy endpoint across trials was ORR, reported in seven trials that included patients with lung cancer (Fig. 2) [14,15,16,17,18,19,20]. These trials evaluated therapies targeting NTRK gene fusion (larotrectinib, entrectinib, repotrectinib), BRAF V600E mutations (dabrafenib with trametinib), RET fusions (selpercatinib), and HER2 positivity (fam-trastuzumab deruxtecan-nxki). Post-approval trial data were available for pembrolizumab (TMB-H) and selpercatinib (RET gene fusion), while updated lung cancer-specific results for other tissue-agnostic therapies were not yet available at the time of our search. The primary safety outcome, defined as the prevalence of TRAEs/TEAEs in patients with lung cancer, was reported in four trials, with rates ranging from 10 to 59.7% [15, 19, 21, 22]. Table 1 presents trial data identified by our search.
Fig. 2
Objective response rate (ORR) of all US Food and Drug Administration (FDA)-approved tissue-agnostic therapies. Bars represent the most recent ORR data from lung cancer cohorts included in the trials that led to FDA approval (excluding post-approval or other trials). Blue bars indicate data from general lung cancer cohorts, green bars represent cohorts of previously untreated patients with Lung cancer, and red bars represent cohorts of previously treated patients with lung cancer. Vertical error bars show the 95% confidence interval (CI), indicating the range of variability in the ORR estimates. Sample sizes for each trial cohort are displayed within the bars. Therapies without lung cancer-specific ORR data are left blank.
Table 1 Tissue agnostic drug approvals and related trials led to US Food and Drug Administration (FDA) approvals and trials published post-approval3.1 dMMR & MSI-H: Pembrolizumab and DostarlimabDeficient mismatch repair (dMMR) indicates a disruption in the DNA mismatch repair system, which is responsible for correcting replication errors during cell division. When this system fails, mutations accumulate, particularly in regions of repetitive DNA sequences known as microsatellites, resulting in microsatellite instability-high (MSI-H) status and an overall high tumor mutational burden [46]. Tumors harboring dMMR or MSI-H alterations tend to generate numerous immunogenic neoantigens, increasing their visibility to the immune system [46]. These tumors are often heavily infiltrated by immune cells, especially cytotoxic T lymphocytes, suggesting an active immune response against tumor-associated antigens [47].
Pembrolizumab, a monoclonal antibody targeting the Programmed Cell Death Protein 1 (PD-1), was first approved in 2014 for metastatic melanoma. In May 2017, it received additional accelerated approval, becoming the first FDA-approved tissue-agnostic therapy. This indication was for patients with previously treated, unresectable or metastatic solid tumors characterized by MSI-H or dMMR, who had no satisfactory alternative treatment options [23]. This approval was based on pooled data from five clinical trials: KEYNOTE-012 [48], KEYNOTE-028 [49], KEYNOTE-016 [50], KEYNOTE-158 [14], and KEYNOTE-164 [51], comprising 149 patients in total (including only one SCLC patient) at the time of FDA review. Of these, only Keynote-158 included patients with lung cancer. The final publication of KEYNOTE-158 described a larger cohort of 233 patients, including four patients with SCLC explicitly reported. The trial also included an unspecified number of patients with lung neuroendocrine tumors [14], though efficacy outcomes were not disaggregated by cancer type. As a result, the clinical efficacy of pembrolizumab in dMMR/MSI-H lung cancer remains unclear [14]. Our review of the published literature and clinicaltrials.gov did not identify additional trials reporting lung cancer-specific efficacy data for this tissue-agnostic indication. Real-world evidence is also limited to case reports [52], which describe durable responses, but no cohort-level real-world data specific to dMMR/MSI-H NSCLC were found. These findings highlight the need for further studies to evaluate the role of pembrolizumab in the treatment of dMMR/MSI-H lung cancer.
Dostarlimab, another PD-1 monoclonal antibody, was initially approved by the FDA for the treatment of adult patients with dMMR recurrent or advanced endometrial cancer. In 2021, it received supplementary accelerated approval for the treatment of advanced dMMR solid tumors, regardless of tumor origin [53]. This tissue-agnostic approval was based on results from cohort F of the GARNET trial [35], though it is important to note that no patients with lung cancer were included in cohort F at the time of approval [36]. While cohort E of the same trial included patients with NSCLC, this group was not restricted to individuals with dMMR tumors [54]. Our review of the literature and ongoing trials did not identify any additional studies evaluating dostarlimab for tissue-agnostic indications that include lung cancer. No cohort-level real-world data were found for dostarlimab in dMMR/MSI-H lung cancer.
Together with the limited data available on pembrolizumab for dMMR/MSI-H lung cancer, these findings highlight a critical gap in the literature. Additional research is needed to determine the efficacy of PD-1 inhibitors, including pembrolizumab and dostarlimab, in lung cancer harboring dMMR/MSI-H alterations. The paucity of studies in this area is likely due, in part, to the rarity of dMMR/MSI-H mutations in lung cancer. One study reported that only 1.16% of patients with NSCLC were identified as dMMR/MSI-H [55]. Despite their low prevalence, these cancers are associated with high morbidity and mortality, highlighting the importance of continued investigation. Better understanding the role of immunotherapy in this rare molecular subset may not only improve outcomes for affected patients but also offer broader insights into lung cancer biology and the potential for precision immunotherapy.
3.2 TMB-H: PembrolizumabIn June 2020, pembrolizumab received another FDA approval for the treatment of adults and children with TMB-H solid tumors, defined as tumors with ≥ 10 mutations per megabase. This approval was based on results from the KEYNOTE-158 trial, which evaluated pembrolizumab’s efficacy in patients with TMB-H tumors. TMB-H tumors tend to produce more neoantigens, novel proteins that enhance tumor immunogenicity and may trigger stronger anti-tumor immune responses. KEYNOTE-158 evaluated pembrolizumab across nine distinct cancer types, including SCLC, cervical, endometrial, and anal cancers. In the SCLC cohort (n = 34), the ORR was 29% (95% CI: 15–47) [55, 56]. Additional evidence of efficacy comes from a pooled retrospective analysis of 12 phase I–II trials including 158 patients with TMB-H NSCLC, where pembrolizumab achieved an ORR of 30.4% [33]. Real-world evidence is limited. In one cohort of 142 patients treated with first-line pembrolizumab, a TMB-H subgroup (n = 53) included 11 never-smokers, all of whom responded (ORR = 100%) with median OS of 27.95 months; this group showed enrichment for DNA damage response and repair (DDR) mutations [34]. Larger observational studies of PD-1/PD-L1 inhibitors in NSCLC similarly suggest that higher TMB is associated with better response and survival, although most cohorts included multiple ICIs [57]. To date, no lung-specific cohort study has focused on pembrolizumab in TMB-H disease.
The prevalence of TMB-H is notably high in lung cancers. In one study involving 2589 patients across various tumor types, 40% of SCLC and 38–42% of NSCLC cases were classified as TMB-H [57, 58]. These findings highlight the potential of pembrolizumab as an effective treatment option for patients with lung cancer with high tumor mutational burden, particularly in cases where standard therapies are limited or ineffective.
3.3 NTRK Fusions: Larotrectinib, Entrectinib, RepotrectinibNeurotrophic tyrosine receptor kinase (NTRK) genes encode the tropomyosin receptor kinase (TRK) family of proteins, which are involved in critical signaling pathways regulating cell growth, differentiation, and survival. Gene fusions involving NTRK1, NTRK2, or NTRK3 can lead to constitutive TRK activation, contributing to the development and progression of a wide range of solid tumors [60].
Larotrectinib is a highly selective TRK inhibitor that received accelerated FDA approval in November 2018 for the treatment of advanced solid tumors harboring NTRK gene fusions. This approval was supported by results from three clinical trials—LOXO-TRK-14001 [NCT02122913], SCOUT [NCT02637687], and NAVIGATE [NCT02576431] [25, 26, 61]—which enrolled a total of 55 adult and pediatric patients. Among these, only four patients with lung cancer (tumor histology unspecified) were included [62, 63]. A subsequent 2022 pooled analysis of 20 patients with NTRK fusion-positive lung cancer from trials NCT02576431 and NCT02122913 demonstrated durable clinical responses to larotrectinib. Among the 15 evaluable patients, the ORR was 73% [15]. The median PFS was 35.4 months (95% CI: 5.3–35.4) and median OS was 40.7 months (95% CI: 17.2–not reached) [15]. TRAEs of grade ≥ 3 occurred in only 10% of patients [15]. Real-world evidence is emerging. A Korean multicenter retrospective study including patients with lung cancer reported lower clinical efficacy for larotrectinib compared to phase I/II trials, potentially owing to false-positive or non-canonical NTRK fusions and co-existing driver mutations [64]. However, the abstract did not report lung-specific ORR or survival outcomes [64]. A prospective post-approval ON-TRK study is ongoing and includes a lung cancer cohort [65].
Entrectinib is a multikinase inhibitor targeting TRK, ROS1, and ALK, which received accelerated FDA approval in 2019 for the treatment of advanced NTRK fusion-positive solid tumors. This approval was based on a pooled analysis of three phase 1 and 2 clinical trials: ALKA-372-001, STARTRK-1 and STARTRK-2 [66, 67]. Entrectinib demonstrated durable responses across 10 NTRK fusion-positive tumor types, including NSCLC, sarcoma, mammary analogue secretory carcinoma, breast, thyroid, and colorectal cancers. In the initial analysis, only 10 patients with NSCLC were included [28, 66]. A 2020 update expanded the cohort to 22 patients with NSCLC, revealing an ORR of 63.6% (95% CI: 40.7–82.8), a median DOR of 19.9 months (95% CI: 10.4–29.4), and a median OS that was not reached (95% CI: 20.8–not reached) [16]. However, lung cancer-specific safety data were not reported. Real-world evidence remains limited. A multicenter real-world study from Turkey, which included patients with lung cancer, reported an ORR of 35.3% (95% CI: 14.2–62.7) with a median OS of 20.8 months (95% CI: 0–48.5), but lung-specific outcomes were not disaggregated [67]. Similarly, a US Veterans Health Administration study identified 33 patients with NTRK fusions or rearrangements across tumor types; of the four patients treated with entrectinib, none achieved an objective response, including those with NSCLC [68].
Repotrectinib is a next-generation TRK inhibitor designed to overcome resistance to earlier TRK inhibitors. Initially approved for ROS1-positive NSCLC, it received supplementary accelerated FDA approval on June 13, 2024, for the treatment of locally advanced or metastatic solid tumors with NTRK gene fusions [20, 44]. This approval was based on the TRIDENT-1 trial (a multicenter, single-arm, open-label, multi-cohort trial) that assessed repotrectinib in both TRK inhibitor-naïve and TRK inhibitor-pretreated patients [20, 44]. Among 21 patients with NSCLC included in the lung-cancer-specific cohorts, TRK inhibitor-naïve patients had an ORR of 62% (95% CI: 43–86), a 12-month DOR of 92% (95% CI: 76–100) and 12-month PFS of 64% (95% CI: 43–86). In TRK inhibitor-pretreated patients with NSCLC, the ORR was 42% (95% CI: 18–71), with a 12-month DOR of 44% (95% CI: 1–88) and 12-month PFS of 23% (95% CI: 0–49) [20, 44]. However, Lung cancer-specific safety data were not reported. Real-world evidence remains limited. Only case-level data have been published, including one report of a patient with atypical carcinoid of the Lung achieving a sustained partial response lasting over 10 months [68]. To date, no cohort-level real-world data are available for repotrectinib in NTRK fusion-positive lung cancer.
Despite these promising outcomes, NTRK fusions are rare in solid tumors, occurring in approximately 1% of all cancers [69]. In NSCLC, the estimated prevalence of NTRK1/2/3 rearrangements is 1–2% [70, 71]. Consequently, while the overall utility of NTRK-targeted therapies in lung cancer is limited by their low incidence, early studies indicate that patients with NTRK fusion-positive lung cancer may derive meaningful benefit from TRK inhibitor therapy. These targeted agents have shown favorable efficacy in appropriately selected patients, particularly when compared to outcomes reported with standard chemotherapy. While early safety profiles appear encouraging, the lack of lung cancer-specific safety data highlights the need for further investigation in this patient population.
3.4 BRAF V600E Mutations: Dabrafenib plus TrametinibBRAF V600E is a constitutively active mutation of the BRAF kinase that drives unregulated cell proliferation and differentiation, independent of upstream RAS activation. Initially targeted in melanoma, BRAF V600E has since been identified in multiple tumor types, including colorectal cancer (CRC), thyroid cancer, glioma, and NSCLC [72]. However, responses to BRAF inhibition vary across cancers, reflecting the complexity of tumor biology. For example, while BRAF inhibitors produced strong responses in melanoma, their efficacy in CRC was limited, despite the same underlying mutation, due to compensatory EGFR activation [73]. This discovery informed the development of combination therapies targeting both BRAF V600E and EGFR [74].
The broader success of combination therapy led to the adoption of dual BRAF and MEK inhibition, targeting both upstream and downstream components of the MAPK pathway. The combination of dabrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) demonstrated synergistic antitumor activity, an acceptable safety profile, and efficacy across multiple tumor types, including lung cancer [75]. In 2017, this combination was approved for the treatment of metastatic NSCLC with BRAF V600E mutations [76]. In 2022, this regimen received supplementary accelerated FDA approval for adult and pediatric patients (≥ 6 years) with unresectable or metastatic BRAF V600E mutant solid tumors who had progressed on prior therapies and had no satisfactory treatment alternatives [17]. This approval was based on six clinical trials: BRF117019, CTMT212X2101, NCI-MATCH, COMBI-d, COMBI-v, and BRF113928 [37]. Lung cancer-specific data came from cohorts B and C of the BRF113928 trial, which included 57 previously treated and 36 treatment-naïve patients with BRAF V600E-mutated metastatic NSCLC [77]. A follow-up analysis with at Least 5-years of data showed that, in previously treated patients (cohort B, n = 57), the ORR was 68.4% (95% CI: 54.8–80.1), median PFS was 10.2 months (95% CI: 6.9–16.7), and median OS was 18.2 months (95% CI: 14.3–28.6) [17]. In treatment-naïve patients (cohort C, n = 36), the ORR was 63.9% (95% CI: 46.2–79.2), median PFS 10.8 months (95% CI: 7.0–14.5), and median OS was 17.3 months (95% CI: 12.3–40.2) [
Comments (0)