
Remember me

A total of 186 complete responses were received. One of the respondents was excluded from the data analysis as the respondent’s education did not meet the inclusion criteria (i.e., physician, pharmacist, or nurse). A total of 185 responses were analyzed. Of these 185 respondents, 32 were physicians, 50 nurses, 26 MSc pharmacists, and 77 BSc pharmacists. The majority (66%, n = 21/32) of the physicians were specialized.
3.1 DemographicsDemographics are presented in Table 1. Most of the HCPs participating in the questionnaire were professionally experienced, as almost 75% (n = 138/185) of the respondents had been in their profession for over 10 years. The majority of the physicians (94%, n = 30/32), 66% (n = 33/50) of the nurses, 74% (n = 57/77) of the BSc pharmacists, and 69% (n = 18/26) of the MSc pharmacists had over 10 years of experience in their profession. Only 14% (n = 25/185) of all HCPs had less than 5 years of experience in their profession. Half (56%, n = 18/32) of the physicians and 68% (n = 34/50) of the nurses worked in public healthcare (hospitals or healthcare center), whereas 69% (n = 53/77) of the BSc pharmacists and 46% (n = 12/26) of the MSc pharmacists worked in retail pharmacies.
Table 1 Healthcare professional demographics3.2 DHPC KnowledgeThe knowledge scores for each professional group are presented in Table 2. In our research sample, MSc pharmacists were best aware and nurses least aware of the meaning and purpose of DHPCs. The average knowledge scores for physicians, nurses, MSc pharmacists, and BSc pharmacists were 6.09, 4.54, 6.85, and 5.82, respectively, out of the possible 8.0. Unlike the observation that MSc pharmacists have the best knowledge of DHPCs, the observation that nurses are least familiar with DHPCs was also statistically confirmed by comparing nurses with the other HCPs (one-way analysis of variance [ANOVA] with post hoc Bonferroni correction, F(1, 183) = 13.74, p < 0.001). The knowledge scores did not change significantly if HCPs working in pharmaceutical industry were excluded (updated values for the same HCP groups: 6.10, 4.54, 6.72, and 5.77). The average knowledge score for all HCPs was 5.67.
Table 2 Direct healthcare professional communication knowledge among HCPsThe term DHPC was recognized by 65% (n = 121/185) of the respondents to be a communication letter sharing possible concerns related to safety and quality of medicinal products. Between professional groups, MSc pharmacists were best aware of this purpose, as 85% (n = 22/26) answered correctly. A relatively large portion of nurses (32%, n = 16/50) and BSc pharmacists (13%, n = 10/77) did not know what a DHPC is. Approximately half (45%, n = 84/185) of the respondents knew that DHPCs are published on the webpage of the Finnish Medicines Agency, the national competent authority.
3.3 DHPC ExperienceOnly 37% (n = 69/185) of the HCPs recognized that they had received one or more DHPC letters during their career. The majority (87%, n = 60/69) of these HCPs found the letters important for their work. Physicians seem to receive the most DHPC letters, as 56% (n = 18/32) had received at least one, whereas 39% (n = 10/26) of the MSc pharmacists, 34% (n = 26/77) of the BSc pharmacists, and 30% (n = 15/50) of the nurses had received at least one DHPC.
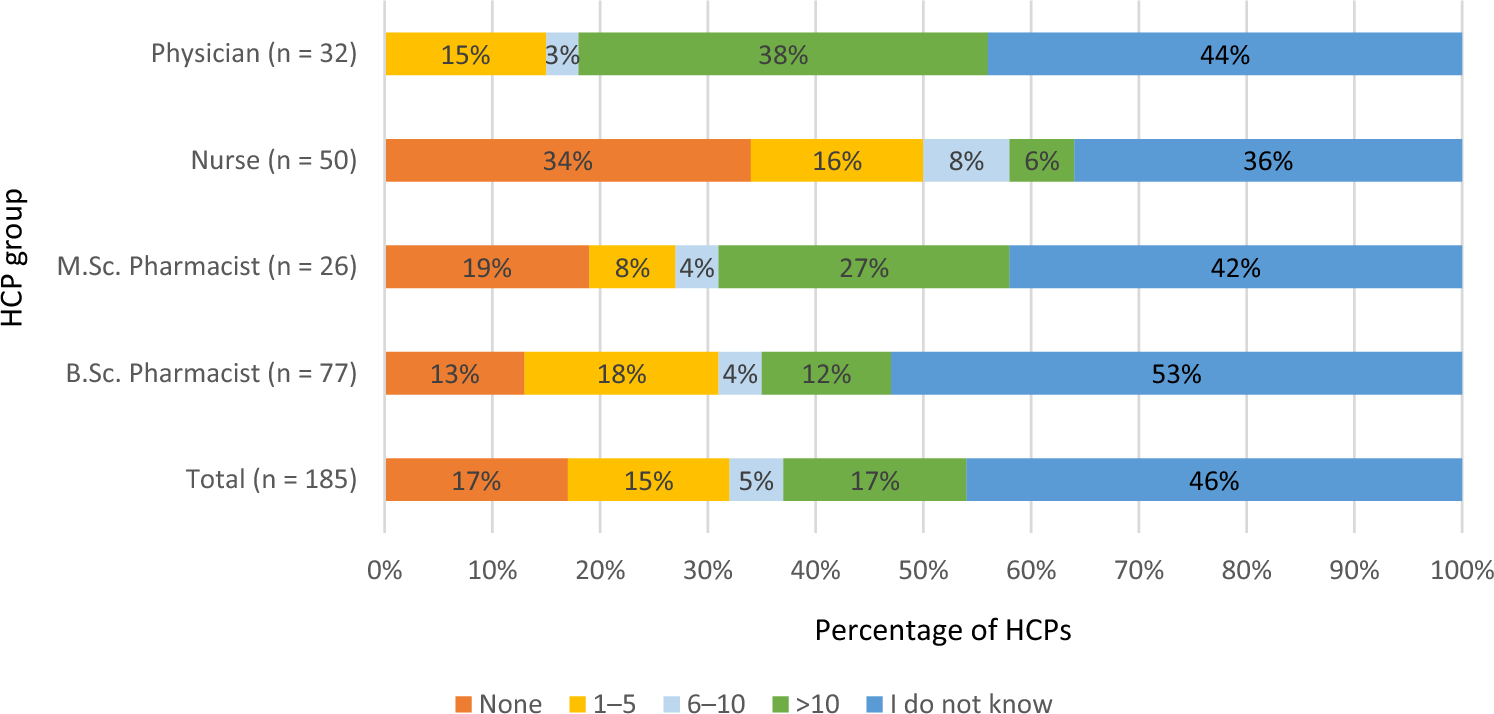
Nearly half (46%, n = 84/185) of the respondents did not know whether they had received DHPC letters, and close to one fifth (17%, n = 32/185) believed that they had not received any DHPCs during their career. The portion of HCPs being ignorant of having received DHPC letters was similar among professions. The DHPC experience among HCPs is shown in Fig. 1.
Fig. 1
Direct healthcare professional communication experience among healthcare professionals. Questionnaire question: How many DHPC letters have you received during your career? BSc Bachelor of Science, DHPC direct healthcare professional communication, HCP healthcare professional, MSc Master of Science
On the basis of the open-ended answers, HCPs would improve DHPC letters by keeping them as short and clear as possible. In addition, the core points of the safety message and required measures should be highlighted. Several HCPs highlighted the visibility of these letters. One BSc pharmacist stated, “visibility in such a way that it cannot go unnoticed; for example, on the front page of the pharmacy program immediately after opening the computer.” This quote also highlights the importance of finding the most effective distribution channels for each recipient group to maximize the impact of the message. In some situations, using multiple channels could lead to a better reach of the HCPs.
3.4 RMP Educational Material KnowledgeThe knowledge scores for each professional group are presented in Table 3. In our research, the sample of MSc pharmacists had the highest knowledge score concerning RMP educational material followed by BSc pharmacists, physicians, and nurses (average knowledge scores: 7.23, 6.48, 5.78, and 4.88, respectively). The better RMP educational material knowledge among pharmacists compared with physicians and nurses was also confirmed statistically (one-way ANOVA with post hoc Bonferroni correction, F(1, 183) = 12.68, p < 0.001). The knowledge scores did not change significantly if HCPs working in the pharmaceutical industry were excluded (updated values for the same HCP groups: 7.17, 6.44, 5.74, and 4.88). The average knowledge score for all HCPs was 6.03.
Table 3 RMP educational material knowledge among Finnish HCPsBased on our results, 78% (n = 145/185) of the HCPs knew that the purpose of the RMP educational material is to minimize the risks associated with the use of the medicinal product, and 78% (n = 142/185) knew that the purpose is to guide the HCPs and patients to the correct use of the medicinal product. Nearly 30% (n = 14/50) of the nurses, 19% (n = 6/32) of the physicians, and 12% (n = 9/77) of the BSc pharmacists but only 4% (n = 1/26) of MSc pharmacists responded that they did not know what RMP educational material is.
A total of 52% (n = 26/50) of nurses, 38% (n = 12/32) of physicians, and 16% (n = 12/77) of BSc pharmacists mistakenly thought that the purpose of the RMP educational material is to inform about medicinal product availability (including shortages). A relatively large portion of HCPs also erroneously thought that the purpose of RMP educational material is to inform about reimbursement updates (34%, n = 17/50 of the nurses; 22%, n = 7/32 of physicians; 14%, n = 11/77 of BSc pharmacists; and 8%, n = 2/26 of MSc pharmacists). The most challenging claim appeared to be the one questioning whether RMP educational material can be materials that are meant to improve the identification of possible adverse events caused by medicinal products. This claim was correctly answered by only 57% (n = 105/185) of the HCPs.
3.5 RMP Educational Material ExperienceNearly 41% (n = 75/185) of the HCPs did not know whether they had ever used RMP educational material, and close to one quarter (24%, n = 44/185) believed that they had not used RMP educational material during their career. Especially physicians were ignorant of having used RMP educational material (59%, n = 19/32 versus 27–42% in other professions), and nurses were certain of not having used RMP educational material (48%, n = 24/50 versus 10–27% in other professions). The RMP educational material experience among HCPs is shown in Fig. 2.
Fig. 2
RMP educational material experience among healthcare professionals. Questionnaire question: How many times have you used RMP educational material during your career? BSc Bachelor of Science, HCP healthcare professional, MSc Master of Science, RMP risk management plan
Half (50%, n = 93/185) of the HCPs answered that they would like to be informed of RMP educational material as soon as it is available. Especially nurses (50%, n = 25/50) and pharmacists (44%, n = 45/103) would prefer to be informed of RMP educational material when administering and delivering a medicinal product to the patient. Physicians, however, prefer to receive information about RMP educational material as soon as possible (53%, n = 17/32) or as a summary once a month (34%, n = 11/32).
Nearly half (42%, n = 78/185) of the HCPs did not know where to check whether a medicinal product has RMP educational material. BSc pharmacists were the least aware of where to find the RMP educational material (56%, n = 43/77 versus 19–38% in other professions). This difference was also statistically significant (Chi-squared test, X2 = 10.13, df = 1, p = 0.001; Fisher’s exact test, p = 0.001).
Approximately one quarter (24%, n = 45/185) of the respondents considered web-based databases as the most accessible location for the RMP educational material. Databases are widely used in Finland to support HCPs in their daily work. Importantly, while physicians and pharmacists prefer electronic materials in web-based databases, nurses still want to receive RMP educational material as printed materials as well.
3.6 HCPs Experiences and Preferences Concerning Safety CommunicationHalf of the HCPs (54%, n = 99/185) felt that they receive insufficient up-to-date safety information about medicinal products. A clear separation between professions with a graduate degree (physicians and MSc pharmacists) and an undergraduate degree (nurses and BSc pharmacists) was observed. Two thirds (66%, n = 38/58) of physicians and MSc pharmacists felt that they receive enough up-to-date safety information, whereas nearly two thirds (62%, n = 79/127) of nurses and BSc pharmacists felt that the safety information they receive is not adequate. This difference was also statistically significant (Chi-squared test, X2 = 12.30, df = 1, p < 0.001; Fisher’s exact test, p < 0.001). The HCP satisfaction with the amount of safety information they receive is shown in Fig. 3.
Fig. 3
HCP satisfaction in the amount of up-to-date safety information they receive and their degree program pharmacovigilance education. BSc Bachelor of Science, HCP healthcare professional, MSc Master of Science
According to the open-ended answers, drug safety information should be shared especially on the following topics: important or new contraindications, adverse reactions and interactions, serious safety-related risks and risk minimization, preparation and administration of medicinal products, and other significant matters affecting the safe use of medicinal products. Especially new, significant, and serious side effects should be rapidly communicated to the HCPs (34%, n = 63/185). A physician summarized this point well: “factors influencing the prescribing of medications, particularly serious side effects and their avoidance.” Physicians and nurses stated that they would also like to receive information about new, significant interactions, while pharmacists would highly value information about quality and availability of medicinal products. Risk reduction related to the safe use of medicinal products is also important for pharmacists, while nurses value more information regarding the preparation of the medicinal product before administration and general administration of the medicinal product.
Email is the most preferred communication channel for safety information for 38% (n = 70/185) of the HCPs. Nurses seem to rely heavily on pharmacists/hospital pharmacies to keep them aware of the latest safety information.
3.7 Pharmacovigilance Education and Need for Additional TrainingMost of the respondents (79%, n = 146/185) felt that the PhV education in their degree program was not comprehensive enough. This observation applies to all professions, as no statistically significant differences were observed between the groups (Chi-squared test, X2 = 2.82, df = 3, p = 0.42). It seems that the dissatisfaction with the PhV education has not changed with time, as no statistically significant differences were observed between groups when HCPs were stratified according to their experience in their profession (Chi-squared test, X2 = 1.65, df = 3, p = 0.65). Interestingly, a shift in satisfaction might be on the horizon, as all physicians and MSc pharmacists who graduated less than 5 years ago consider the PhV education as sufficient in their degree program. Especially adverse reactions, interactions, and general pharmacovigilance were recognized as important topics that should be included in the degree more comprehensively. More than half (57%, n = 106/185) of the HCPs who answered the questionnaire stated that they would like to receive additional training in pharmacovigilance. The satisfaction of the HCPs with the PhV education in their degree program and HCPs wanting additional training in PhV are shown in Fig. 3.
Comments (0)