
Remember me



A total of 1761 HNSCC patients were initially screened between January 2008 and July 2018. From these, we included only 728 patients who underwent surgery as their first treatment. We excluded 19 patients who were lost to follow-up, 53 with multiple simultaneous tumors, and 98 who had previous head and neck tumors, resulting in a final cohort of 558 patients. Among these, 243 received additional treatments (e.g., adjuvant or subsequent therapy) within the first postsurgical year. A total of 354 patients (63%) were male with a median age of 64 (interquartile range: 56–73).
While all 558 patients had at least 25% of the included clinical parameters and routine blood markers, only 195 had T1W contrast-enhanced MR imaging available. We included 34 clinical parameters, 18 blood markers, and 107 radiomic features in our study. A total of 478 patients (86%) in the included cohort survived within one year from surgery, whereas only 52 patients (9%) required a feeding tube after one year. Table 1 summarizes the baseline patient characteristics and the data modalities used.
Table 1 Baseline demographic and clinical characteristics of the complete 558 HNSCC patient cohort, along with the availability of data modalities for model developmentPredicting treatment outcomesWe investigated the predictive value of each pretreatment data modality—clinical data, blood-based markers, and imaging features—both independently and in combination, for two binary classification tasks: (1) one-year survival post-surgery and (2) one-year dependence on tube feeding. Model performance was evaluated using the area under the receiver operating characteristic curve (AUC), the area under the precision–recall curve (PR-AUC), and the F1-score.
Predicting one-year overall survivalWithout including postsurgical treatment information, clinical data alone demonstrated the highest predictive power for one-year survival (AUC: 0.75 ± 0.10, PR-AUC: 0.94 ± 0.03, F1-score: 0.64 ± 0.06; p < 0.001). Blood-based parameters showed moderate predictive ability (AUC: 0.67 ± 0.09, PR-AUC: 0.93 ± 0.02, F1-score: 0.68 ± 0.05; p = 0.001). In contrast, imaging features alone yielded a moderate AUC of 0.67 ± 0.17 but did not reach statistical significance (p = 0.26). Notably, combining all three modalities did not improve performance beyond that achieved by clinical data alone (AUC: 0.68 ± 0.16; p = 0.38).
When information regarding additional postsurgical treatments was incorporated into the model as a binary feature, the predictive performance of the prognostic model did not meaningfully change. Clinical data continued to yield the best survival predictions, with a slight increase in AUC (0.76 ± 0.07) and PR-AUC (0.95 ± 0.02). Blood data performance remained relatively stable, showing only a minor decrease in AUC (0.66 ± 0.09, PR-AUC: 0.92 ± 0.03; p = 0.002). Imaging data again provided modest predictive capability (AUC: 0.64 ± 0.16, PR-AUC: 0.92 ± 0.05, F1-score: 0.65 ± 0.08; p = 0.45). Importantly, adding imaging and blood variables to clinical data did not confer additional improvements (AUC: 0.66 ± 0.12, PR-AUC: 0.92 ± 0.04; p = 0.62).
Predicting one-year survival using information on whether the patient received additional postsurgical treatment data alone yielded the lowest performance (AUC: 0.57 ± 0.11, PR-AUC: 0.91 ± 0.03, F1-score: 0.13 ± 0.27; p = 0.08), indicating that merely knowing whether patients received additional therapies was insufficient for robust survival prediction (Table 1).
Predicting dependence on tube feedingPredicting feeding tube requirements one year after surgery was more challenging than predicting survival (Table 2). Before incorporating additional postsurgical treatment information, clinical data offered the highest AUC (0.66 ± 0.07) but had a low PR-AUC (0.23 ± 0.12) and an F1-score of 0.22 ± 0.06, without reaching statistical significance. Blood (AUC: 0.64 ± 0.08) and imaging (0.60 ± 0.24) had similar or lower performance, though imaging features had a slightly higher PR-AUC (0.28 ± 0.16). Combining all modalities did not markedly improve performance (AUC: 0.65 ± 0.19, p = 0.48).
Table 2 Performance of random forest models for predicting one-year survival using individual (clinical, blood, and imaging) and combined modalities across 10 cross-validation folds (with and without the inclusion of additional postsurgical treatment data)After including details about additional postsurgical treatments, performance for feeding tube prediction improved, particularly for blood data (AUC: 0.70 ± 0.12, PR-AUC: 0.22 ± 0.09; p = 0.001) and clinical data (AUC: 0.69 ± 0.07, PR-AUC: 0.22 ± 0.08; p = 0.01). Imaging performance remained largely unchanged (AUC: 0.61 ± 0.20, p = 0.77), while the combined model showed a slight decrease (AUC: 0.63 ± 0.22, p = 0.48). Interestingly, models using only the binary “presence of additional postsurgical treatment” variable achieved an AUC of 0.67 ± 0.07 (PR-AUC: 0.47 ± 0.08; p = 0.002), suggesting that postoperative treatment patterns may contain meaningful information relevant to nutritional support needs (Table 3 and Fig. 1).
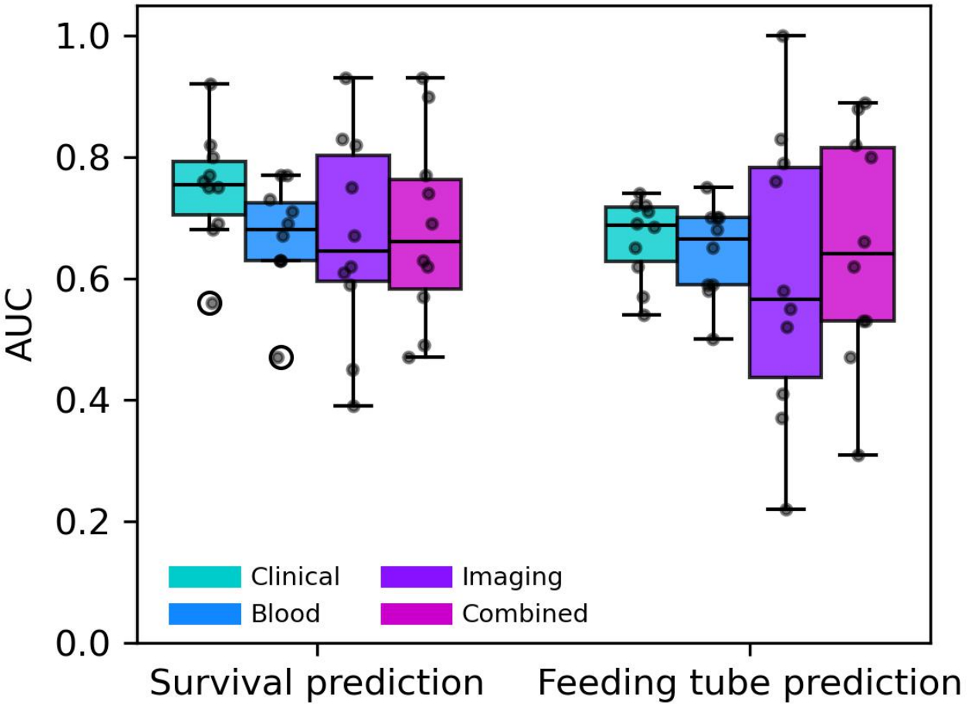
Table 3 Performance of random forest models for predicting one-year feeding tube dependence using individual (clinical, blood, and imaging) and combined modalities across 10 cross-validation folds (with and without the inclusion of additional postsurgical treatment data)Fig. 1
Predictive performance of models trained on individual and combined data modalities. Boxplots of the area under the receiver operating characteristic curve (AUC) across 10 cross-validation folds for both (left) one-year survival and (right) one-year feeding tube dependence predictions. Predictive models were evaluated using (turquoise) clinical data, (blue) blood markers, (purple) imaging features, and (magenta) all modalities combined
Explainability of the classifiersWe used SHAP values to identify the most influential features in predicting both survival and feeding tube dependence.
With respect to predicting survival, the interpretation of most influential features is as follows. In the clinical model, T stage and N stage consistently emerged as the strongest survival predictors (Table 4). T stage corresponds to the tumor size and extent, while N refers to the degree of lymph node involvement. Functional or lifestyle factors (e.g., work situation, physical disability) also remained relevant. After including postsurgical treatment information, heart rate (pulse) appeared among the top five features, indicating potential physiological influences. For blood biomarkers, albumin, hemoglobin (Hb), C-reactive protein (CRP), and mean corpuscular hemoglobin concentration (MCHC) were key predictors, highlighting the impact of systemic inflammation and nutritional status. The binary “additional treatments” feature also emerged as an important variable when included. Gray-level co-occurrence matrix (GLCM) correlation and first-order kurtosis consistently ranked among the top radiomic predictors. Shape-based metrics, such as maximum 2D diameter (slice), were also important before and after including postsurgical treatment information. When all modalities were combined, clinical and blood-based features (e.g., medication count, unique medications count, and Hb) dominated the combined model’s top rankings. Among the imaging features, GLCM correlation and gray-level dependence matrix (GLDM) dependence entropy were the most influential, hinting at the importance of tumor texture heterogeneity for survival prediction. Figure 2 illustrates the ranked predictors for survival in SHAP summary plots.
Table 4 Top five SHAP-ranked features (in order of importance) driving one-year survival prediction for each data modality (clinical, blood, imaging, and combined), reported with and without the presence of additional postsurgical treatments as a binary featureFig. 2
Explainability of survival models. SHAP summary plots showing the most influential features for predicting one-year survival when using a clinical data, b blood markers, c imaging features, and d all modalities combined. These analyses do not include additional postsurgical treatment data
With respect to predicting dependence on tube feeding, the interpretation of the most influential features is as follows. Before accounting for postsurgical treatment details, clinical T stage, diagnosis type, weight, and age had the highest impact (Table 5 and Fig. 3). For blood-based predictors, CRP, sodium, magnesium, potassium, and glucose repeatedly appeared as top predictors, reinforcing the role of systemic inflammation, electrolyte balance, and metabolic status in prolonged feeding tube dependence. In the imaging model, shape-based features were the most predictive. Least axis length, minor axis length, and maximum 2D diameter slice were among the strongest predictors, suggesting that anatomical structures contributed to feeding tube dependency. When all modalities were combined, metabolic markers (e.g., glucose, magnesium) and shape-based features (e.g., least axis length) were important before additional treatment information was taken into account. Once postsurgical treatment information was added to all individual and combined modalities, the “additional treatments” feature became the leading predictor, suggesting that subsequent interventions significantly influenced whether patients developed feeding tube dependence.
Table 5 Top five SHAP-ranked features (in order of importance) influencing one-year feeding tube dependence prediction under each data modality (clinical, blood, imaging, and combined), both with and without incorporating additional postsurgical treatments as a potential confounderFig. 3
Explainability of feeding tube prediction models. SHAP summary plots illustrating key predictors of one-year feeding tube dependence using a clinical data, b blood markers, c imaging features, and d all modalities combined, without incorporating additional postsurgical treatment information
Comments (0)