
Remember me



Radiotherapy treats cancers by destroying malignant tissues, however, this process can also kill healthy tissues, causing deleterious effects. Therefore, the challenge of radiotherapy is to deliver a dose sufficient for tumor destruction while simultaneously minimizing exposure to surrounding organs at risk (OARs) sufficiently to prevent adverse outcomes.
To address this challenge, modern radiotherapy systems have been developed that are capable of delivering highly conformal, precise, and accurate treatments [1, 2]. These technological advances have frequently left treatment planning as the largest hurdle to quality plan delivery. Therefore, many treatment planning support tools have been developed to facilitate various steps of the complex treatment planning workflow [1, 3]. In this paper, we present a treatment planning decision support infrastructure designed as a platform for the development, testing, and implementation of planning algorithms for identifying similar radiotherapy cases for use as references during plan creation.
Clinical backgroundThe increasing complexity of computer controlled radiation delivery machines, which offer numerous parameters for control, necessitate the development of medical imaging informatics infrastructures (MIII). The utilization of MIII for planning and delivery has transformed radiotherapy into a software defined system. Modern treatment planning support tools improve plan creation by using the available data rich environment, including 3D image-based dose simulations and the enhanced delivery accuracy availed by image-guided radiotherapy (IGRT), advanced multileaf collimators (MLCs), and gantry control. The use of 3D planning images for anatomical, dose simulations, and the options afforded by the MIII and the software defined nature of radiotherapy delivery have been key enablers for the development of new treatment modalities and planning support tools [1,2,3,4,5,6].
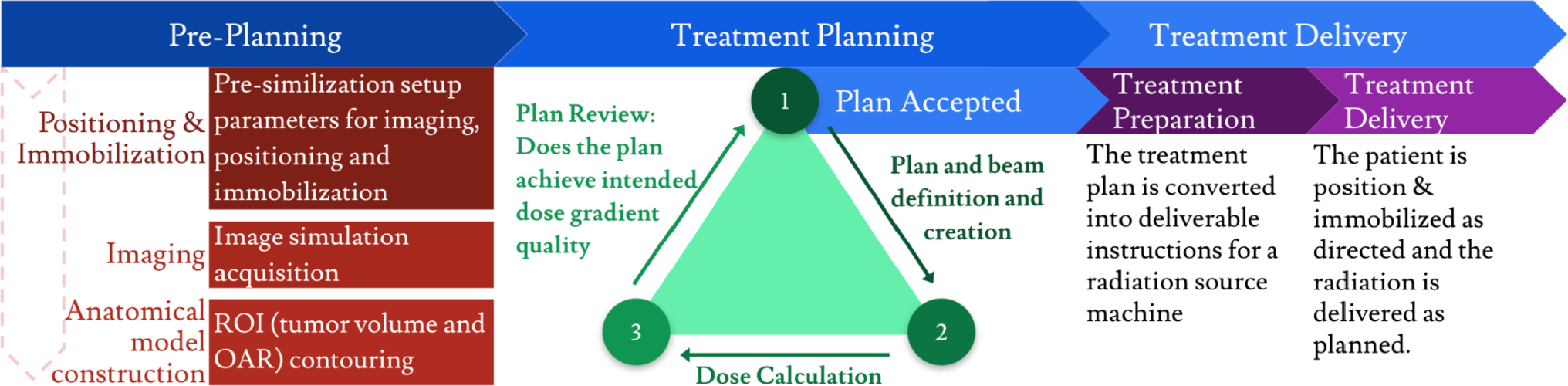
Current treatment planning support tools have become essential, fully integrated components of the standard clinical process, facilitating plan creation at various steps of the clinical workflow (Fig. 1). These tools support critical functions such as auto-segmentation, automated dose optimization, and knowledge-based treatment planning (KBP). Work in automated ROI segmentation helps to control ROI volumes from 3D medical images, partially automating a task that is otherwise a manual part of the clinical workflow. Another popular area of development is automated dose optimization and dose-volume histogram (DVH) prediction, which is a key enabling element of intensity-modulated radiotherapy (IMRT). These advances, including intensity-modulated radiotherapy, were made possible by the 3D dose simulations and other informatics capabilities of the MIII and software defined radiotherapy machines [1, 4,5,6,7,8,9].
Fig. 1
General clinical radiotherapy treatment workflow
Knowledge-based treatment planning is another area of research that utilizes actionable insights from retrospective case datasets to support and optimize treatment planning. Most KBP methods rely on dose simulation comparisons with retrospective cases to predict more optimal dose gradients. Successful commercial implementations exist, such as Varian’s Rapidplan (Varian Medical Systems, Palo Alto, CA, USA), which uses features like ROI registration, target size, overlap area, and dose averaging to automate DVH prediction for plan optimization [10,11,12]. A review of literature from the last 15 years identifies over 165 published papers on KBP, with many successful approaches focusing on DVH prediction based on dose comparisons or averages [7, 8]. Some methods have partially included anatomical features, such as OAR overlaps, shape, size, and direct registration of ROIS, as part of their DVH prediction models [13,14,15]. A few studies have taken this a step further by using relational measures to describe the spatial relationship between an OAR and a target volume. However, most of these relational methods have largely been limited to considering single target-OAR pairs and do not construct a holistic model of the GTV-OAR constellation geometry [16,17,18,19,20]. Therefore, we present a KBP infrastructure to enable, test, and implement models which will match cases based on the spatial distributional geometric relationship of the target volumes to all surrounding OARs, what we call the GTV-OAR constellation.
Proposed decision support infrastructureThe purpose of this work was to develop a novel treatment planning support infrastructure to enable development, testing, and implementation of KBP support tools based on holistic geometric anatomical models. This system matches current planning cases to retrospective best practice cases based on similarity of their GTV-OAR constellation geometry and provides the treatment plans of the similar retrospective cases to serve as references and templates (Fig. 2). This infrastructure follows the trends of previous work by utilizing existing MIII and 3D anatomy simulations to support modeling and comparison of GTV-OAR constellation geometry. This platform is designed to enable exploration, development, and clinical implementation of similarity matching algorithms using holistic geometry models.
Fig. 2
System workflow intervention to clinical radiotherapy treatment workflow. Workflow intervention is in green
The KBP models this system implements allows for further development and exploration of modeling anatomical geometric relationships between target volumes and OARs. The key enabling element of our infrastructure is its ability to calculate quantitative features between the GTV and all OARs, and to store and structure these features relationally from multi-institutional knowledgebase datasets for knowledge-based planning. By calculating quantitative features from the GTV to every OAR, our infrastructure can construct and store a holistic relational representation of the GTV-OAR constellation geometry that is equivalently comparable between cases, even with anatomical variation, a capability that direct surface registration models lack. The data pipeline matches corresponding quantitative features from each GTV-OAR pair between cases, and the overall similarity is calculated from these comparisons. The overall similarity is weighted and normalized based on the number of OARs in common between the two cases, to enable equivalent comparison of calculated similarity across cases. Because it has been demonstrated that OARs with similar spatial relationships to target volumes have similar DVHs, identifying cases by GTV-OAR constellation geometry is a valuable approach [17, 18]. While the KBP model this infrastructure implements considers all GTV-OAR relationships evenly, by retrieving cases with similar constellation geometries, the system identifies clinician-created plans with appropriate differential consideration to each OAR based on factors like serial or parallel criticality or inhomogeneities in tissue between targets and OARs [17, 18].
Our KBP infrastructure retrieves retrospective best practice cases by using GTV-OAR constellation similarity matching, the plans for which can then be used as references during beam number selection and angle or arc conception. The method provides support during a step that is still largely a manual, trial-and-error process, especially in complex instances such as some non-coplanar or SBRT cases. Tools in development for beam configuration support are often complicated, computationally costly and sometimes still don’t assist in the initial conception of beam configurations [21,22,23,24]. While planning for many pathologies and treatment modalities is fairly standardized and automated, instances and modalities remain where delineation of beam field angles and arcs is a persisting challenge and art. In these cases, such as some non-coplanar SBRT or proton therapies, reference to template configurations used for similarly positioned target volumes is particularly valuable. Because cases with similar target-OAR anatomical relationships tend to receive similar doses, identifying cases with similar target-OAR constellations will present treatment and dose plans that reflect the clinical importance and implications of different GTV-OAR relationships.
Comments (0)