
Remember me
As of July 12, 2024 a total of 21 patients with R/R FL had received SC epcoritamab; the median follow-up was 35.0 months (range, 11.0–41.2). As reported previously, patients were heavily pretreated (median, 4 prior LOTs) and had high-risk features, including 57.1% with double-refractory disease and 57.1% with POD24 (Table S1) [18].
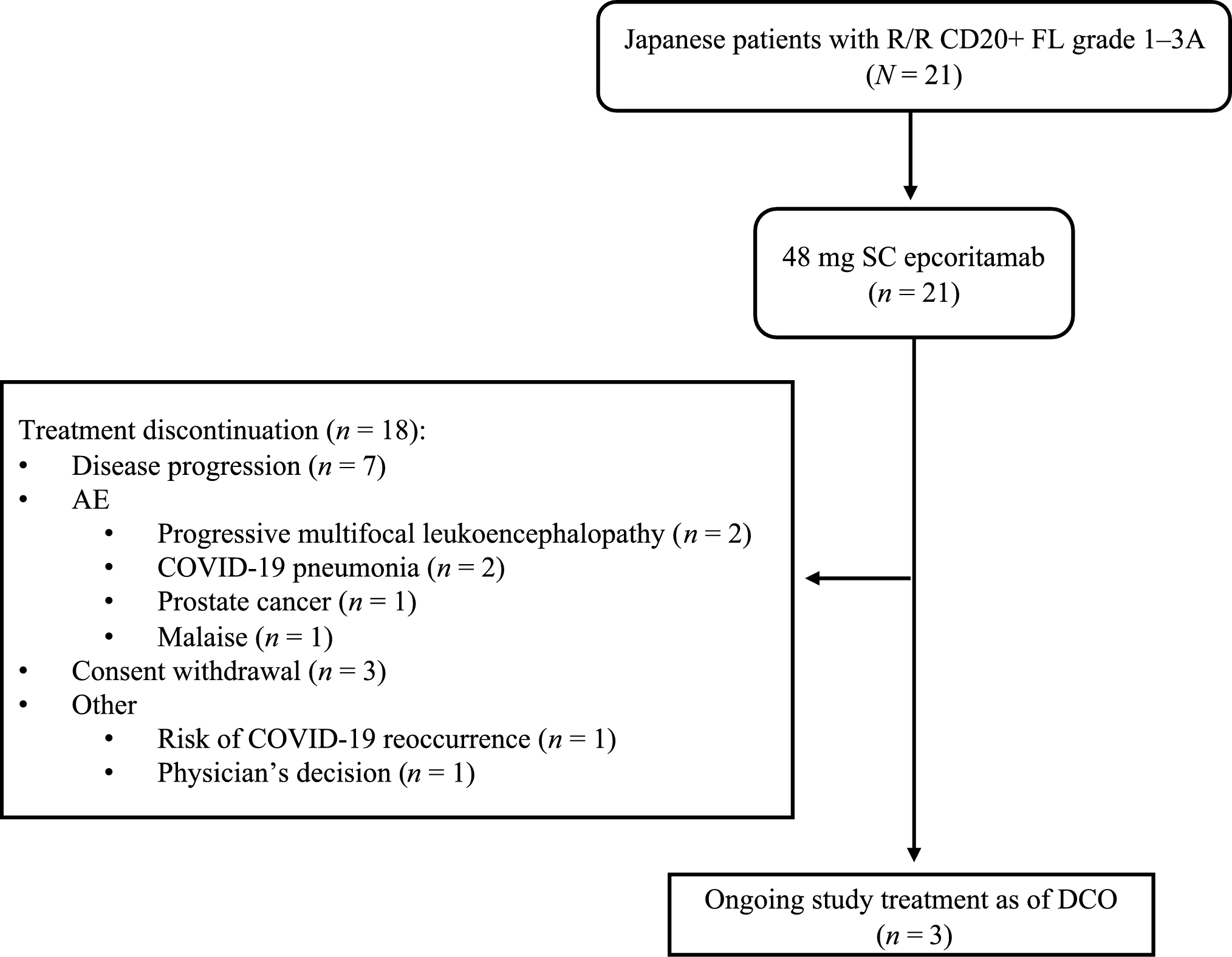
Treatment exposure and dispositionOf the 21 patients who received epcoritamab, 3 (14.3%) were still on treatment at the data cutoff and 18 (85.7%) had discontinued (Fig. 1). Overall, patients received a median of 13 treatment cycles (range, 1–43), and the median duration of treatment was 11.1 months (range, 1–39). The reasons for treatment discontinuation were PD (7/18 [38.9%]), AEs (6/18 [33.3%]), consent withdrawal (3/18 [16.7%]), risk of coronavirus disease 2019 (COVID-19) recurrence (n = 1), and physician’s decision (n = 1). AEs leading to discontinuation were progressive multifocal leukoencephalopathy (PML; n = 2), COVID-19 pneumonia (n = 2), prostate cancer (n = 1), and malaise (n = 1).
Fig. 1
Flowchart illustrating patient enrollment and disposition in the EPCORE NHL-3 study for the R/R FL cohort as of the July 12, 2024 DCO date. AE adverse event, COVID-19 coronavirus disease 2019, DCO data cutoff, FL follicular lymphoma, R/R relapsed/refractory, SC subcutaneous
EfficacyConsistent with the primary analysis, epcoritamab demonstrated an ORR of 95.2% (20/21; 95% CI, 76.2–99.9) and a CR rate of 76.2% (16/21; 95% CI, 52.8–91.8). Only 1 patient had a PR as of the last assessment of the primary analysis, but this patient had no subsequent scans, and therefore, there was no evidence of conversion from PR to CR with longer follow-up. Median TTR was 1.3 months (range, 1.1–1.7) and median TTCR was 1.4 months (range, 1.1–3.6), with most CRs achieved by the first 6-week assessment (Table 1).
Table 1 Efficacy endpoints in the overall R/R FL populationHigh response rates (ORRs, 90–100%; Fig. 2) were also seen in patients with challenging-to-treat disease features, including patients refractory to their last LOT, those with POD24, those with double-refractory disease, patients ≥ 65 years of age, and those 65 to < 75 years of age.
Fig. 2
Forest plot displaying the best ORR across various clinically relevant patient subgroups based on baseline characteristics. The bars represent the percentage of patients in each response category within a 95% CI. aRefractory to both an anti-CD20 mAb and an alkylating agent, regardless of whether they are in the same or different lines of treatment. ASCT autologous stem cell transplant, CI confidence interval; CIT chemoimmunotherapy, mAb monoclonal antibody, ORR overall response rate, POD24 progression of disease within 24 months
At data cutoff, median DOR, DOCR, PFS, and OS were not reached (NR) in the overall population, with 89.7% of patients alive at 36 months (Table 1; Figs. 3 and 4). For patients achieving CR, median DOCR, PFS, and OS were also NR; at 36 months, 66.7% remained in CR, 66.7% remained progression-free, and 93.3% were alive (Fig. 4).
Fig. 3
Kaplan–Meier curve for DOCR in patients with a CR (n = 16). The y-axis represents the probability of maintaining a CR, and the x-axis represents the time in months from the first documented CR. Tick marks indicate censored patients. The median DOCR was not reached. CR complete response, DOCR duration of complete response
Fig. 4
Kaplan–Meier curves illustrating PFS (A) and OS (B) for the overall patient population (N = 21) and for patients who achieved a CR (n = 16). The y-axis represents the probability of survival (PFS or OS), and the x-axis represents the time in months. Tick marks indicate censored patients. CR complete response, OS overall survival, PFS progression-free survival
The majority of patients (14/21) did not proceed to the next treatment. Among the 7 (33.3%) patients who did proceed to the next treatment, 3 (14.3%) received CAR T-cell therapy and the remaining received a variety of chemoimmunotherapy. Of the 7 patients, 3 achieved a best response of CR, 3 achieved PR, and 1 had stable disease while on the next treatment. As of the data cutoff, 5 of the 7 patients were alive, 1 died, and 1 was lost to follow-up.
Of the 17/21 (81.0%) patients with prior bendamustine exposure (median time from last prior bendamustine treatment, 141 days [range, 1–214]), 13 (76.5%) achieved a CR, 3 had a PR, and 1 had stable disease while receiving epcoritamab treatment. The median PFS was 24.3 months (95% CI, 2.6–NR) and median OS was NR in this subgroup.
Among the 13 patients who achieved a CR and discontinued treatment, reasons for discontinuation were PD (n = 3), withdrawal by the subject (n = 2), and other reasons (n = 2: risk of recurrence of COVID-19 [n = 1] and investigator’s decision [n = 1]). The remaining 6 patients discontinued due to AEs. Nine of these patients had a CR as their last assessment and discontinued treatment for reasons other than PD (Fig. 5). Of these 9 patients (median time on treatment, 16.7 months [range, 7.7–34.6]), 7 had a documented CR after discontinuing epcoritamab without initiating subsequent therapy, and 2 did not have a post-discontinuation follow-up. All 7 patients remained in CR at the time of their last imaging evaluation (prior to data cutoff), with a median time from treatment discontinuation to this assessment of 12.3 months (range, 1.0–25.4).
Fig. 5
Swim lane plot detailing the treatment and response duration for patients with a CR as their last assessment who discontinued treatment for reasons other than PD (n = 9). An additional patient achieved CR as the best overall response; however, this patient was excluded from the figure since the last assessment prior to discontinuation was not CR. Per protocol, patients continued to receive scans if they discontinued treatment for reasons other than PD. Each bar represents an individual patient. The length of the bar indicates the time from the start of treatment, with symbols showing the best overall response and the timing of the last disease assessment. Vertical lines indicate 1- and 2-year landmarks. CR complete response, DCO, data cutoff, NE not evaluable, PD progressive disease, PR partial response
Of the 18/21 (85.7%) MRD-evaluable patients, 16 (88.9%) achieved MRD negativity. In patients who were MRD-negative by the landmark C3 day (D) 1 (n = 12) time point, median PFS was NR (95% CI, 2.1–NR) as of data cutoff (Table 1).
SafetyThe safety and tolerability outcomes observed in this 3-year follow-up analysis were largely consistent with those observed in the primary 2-year analysis [18]. CRS (19/21 [90.5%]), injection-site reaction (15/21 [71.4%]), neutropenia (8/21 [38.1%]), rash (8/21 [38.1%]), increased alanine aminotransferase (6/21 [28.6%]), increased aspartate aminotransferase (6/21 [28.6%]), and COVID-19 (6/21 [28.6%]) remained the most reported treatment-emergent adverse events (TEAEs) in ≥ 20% of patients (Table 2). Of the 15/21 (71.4%) patients with grade 3/4 TEAEs as of the current data cutoff, 2 patients experienced new events, all unrelated to epcoritamab treatment, since the time of primary analysis: 1 patient with grade 3 events of stomatitis (not recovered/not resolved at the time of data cutoff) and decreased white blood cells (recovered/resolved) and 1 patient with a grade 3 event of upper respiratory tract infection (recovered/resolved). TEAEs led to dose delays in 14/21 (66.7%) patients. With an additional 13.8 months of follow-up since the primary report, 2 new TEAEs leading to treatment discontinuation were observed (both COVID-19 and related to epcoritamab treatment). Serious TEAEs were reported in 13/21 (61.9%) patients; 1 new serious TEAE of stomatitis, unrelated to epcoritamab, occurred since the primary analysis. No fatal TEAEs occurred during the trial.
Table 2 TEAE summary and most common TEAEs occurring in ≥ 20% of patientsNo new CRS events were observed since the primary analysis with longer follow-up. As previously reported, CRS occurred in 90.5% of patients; events were predominantly grade 1–2, manageable, and all resolved without leading to treatment discontinuation [18]. No immune effector cell-associated neurotoxicity syndrome or clinical tumor lysis syndrome events were reported during the trial.
The EPCORE NHL-3 trial was conducted during the peak of the COVID-19 pandemic and during the time period when the highly infectious Omicron variant and subsequent variants were prevalent. COVID-19 occurred in 6/21 (28.6%) patients over the course of the study; 2 of these patients experienced new events of grade 2/3 COVID-19 after the primary analysis, both of whom discontinued treatment. At data cutoff, 5/6 patients had COVID-19 that had resolved or were recovering/resolving. Maintenance of response was preserved, irrespective of COVID-19 and any resulting deviations in treatment adherence; 6 patients had at least one follow-up scan after COVID-19 and all remained in response (4 CRs and 1 PR who converted to CR after treatment was resumed post COVID-19) except 1 patient who had PD before COVID-19.
Seven patients reported grade ≥ 3 infections, with only 1 grade 3 infection of upper respiratory tract infection reported beyond 2 years of treatment. Grade ≥ 3 infections were mostly viral and respiratory in nature, with no fungal infections or cytomegalovirus reactivations observed. A total of 9 patients received concomitant Ig therapy as of the data cutoff, 2 of whom were new recipients since the primary analysis. Six patients received granulocyte colony-stimulating factor (G-CSF) treatment for grade 3/4 neutropenia during the study; 1 of these patients also experienced an event of grade 3 febrile neutropenia that required treatment with G-CSF and the event resolved. After an initial decline from baseline, a trend to recovery of IgG levels was observed as early as C4D1 and remained stable through C28D1 (Fig. 6).
Fig. 6
Line graph showing the mean IgG levels (mg/dL) in patients over the course of treatment, from baseline through C28D1. The points represent the mean IgG level at each time point, and the error bars indicate the standard error of the mean. The numbers below the x-axis denote the number of patients with available data at each assessment. C cycle, D day, IgG immunoglobulin G
Comments (0)