
Remember me
From January 2022 to February 2024, a total of 21 Japanese patients were enrolled: 9 from the global cohort and 12 from the Japan expansion cohort. Overall, 10 patients were randomized to BPd and 11 patients to PVd. At data cutoff, 60% of patients (6/10) in the BPd group and 27% of patients (3/11) in the PVd group continued study treatment, 10% (1/10) in the BPd group and 64% (7/11) in the PVd group were in follow-up, and 20% (2/10) in the BPd group and 9% (1/11) in the PVd group died. One patient in the BPd group withdrew from the study. The median duration of follow-up was 12.9 months (range 0.2–26.6) in the BPd group and 14.5 months (range 6.0–26.7) in the PVd group, with a minimum ongoing follow-up of 2.8 and 6.0 months, respectively.
Baseline patient characteristics and previous treatments received were generally similar in the two groups, except for International Staging System (ISS) stage III (BPd 20% [2/10] and PVd 0%), extramedullary disease (BPd 20% [2/10] and PVd 0%), and high-risk cytogenetics (at least one high-risk abnormality: t(4;14), t(14;16), or 17p13del; BPd 30% [3/10] and PVd 9% [1/11]) (Table 1). More patients in the BPd group were refractory to lenalidomide (BPd 80% [8/10] and PVd 36% [4/11]), anti-CD38 antibodies (BPd 40% [4/10] and PVd 27% [3/11]), and proteasome inhibitors (BPd 40% [4/10] and PVd 9% [1/11]) than the PVd group. The median total duration of treatment exposure was 6.8 months (range 0.9–26.7) in the BPd group and 6.2 months (range 0.7–26.9) in the PVd group. The BPd group received a median of 7 treatment cycles (range 1–29) of any study treatment while PVd received median of 8 treatment cycles (range 1–35). The overall median relative dose intensity was 76.3% for belantamab mafodotin in the BPd group and 98.2% for bortezomib in the PVd group.
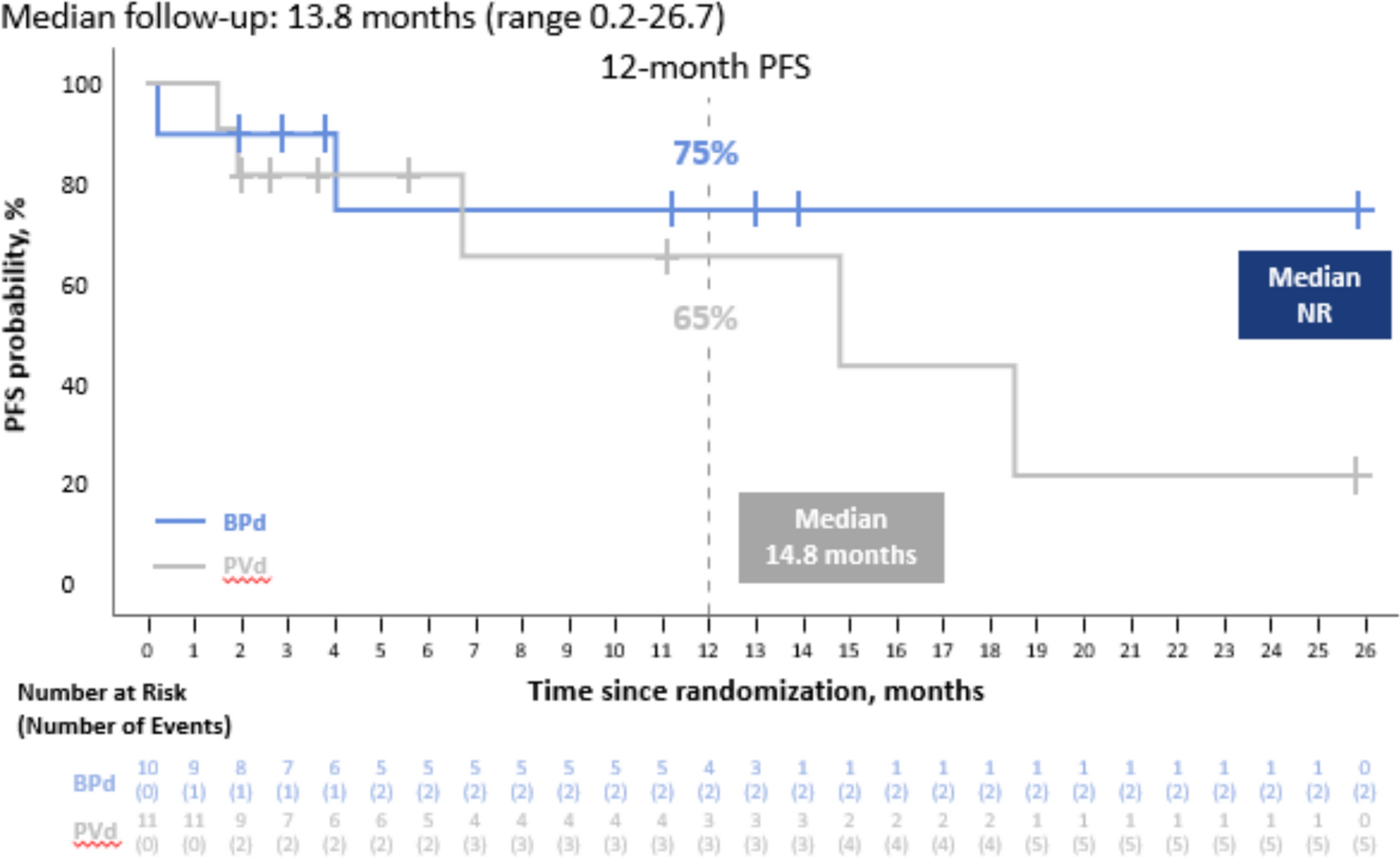
Table 1 Baseline demographic and clinical characteristics and previous therapiesEfficacyThe median PFS was not reached (NR; 95% CI, 0.2–NR) in the BPd group and was 14.8 months (95% CI, 1.9–NR) in the PVd group (Fig. 1). The risk of disease progression or death was lower in the BPd group than the PVd group, although the CI for the HR was wide due to the small sample size (HR 0.53; 95% CI, 0.10–2.78). Disease progression or death occurred in 20% (2/10) in the BPd group and 45% (5/11) in the PVd group. In the BPd group, one patient died from fatal sepsis, which was reported as not related to the study treatment. The sepsis was caused by an infection with Morganella morganii that started prior to day 1 of study treatment. This was felt to be possibly related to high-dose cytotoxic chemotherapy that the patient had received in the month preceding the start of the study treatment. One patient in each of the BPd and PVd groups died due to cancer. Follow-up for OS is currently ongoing.
Fig. 1
Kaplan–Meier Analysis of Progression-free Survival. BPd, belantamab mafodotin, pomalidomide, and dexamethasone; PFS, progression-free survival; PVd, pomalidomide, bortezomib, and dexamethasone; NR, not reached
The proportion of patients who had an ORR (partial response or better) was 90% (9/10; 95% CI, 55.5–99.7) in the BPd group and 73% (8/11; 95% CI, 39.0–94.0) in the PVd group (Table 2 and Fig. S2). The corresponding proportions of patients with a complete response or better were 30% (3/10; 95% CI 6.7–65.2) and 27% (3/11; 95% CI 6.0–61.0), and a very good partial response or better were 70% (7/10, 95% CI, 34.8–93.3) and 36% (4/11; 95% CI, 10.9–69.2) (Table 2). The proportion of patients with a complete response or better and achieved MRD-negative status was 20% (2/10) in the BPd group and 18% (2/11) in the PVd group (Table S2). Among patients with a partial response or better, the median DoR was NR (95% CI, 1.2–NR) in the BPd group and 17.5 months (95% CI, 13.8–NR) in the PVd group. In the BPd group, 78% (7/9) of patients with response had not progressed or died and had ongoing follow-up for PFS at the data cutoff date, compared with 38% (3/8) in the PVd group.
Table 2 Treatment response to BPd and PVdSafetyThe safety population included 21 patients (10 in the BPd group and 11 in the PVd group). AEs of any grade were experienced by all patients in the BPd and PVd groups (Table S3). AEs leading to permanent discontinuation of any treatment was higher in the PVd group (36%, 4/11) compared to the BPd group (10%, 1/10). The most frequently reported AEs in the BPd group were blurred vision (90%, 9/10), alanine aminotransferase increase (60%, 6/10), constipation (50%, 5/10), aspartate aminotransferase increase (40%, 4/10), diarrhea (40%, 4/10), and foreign body sensation in eyes (40%, 4/10). In the PVd group, the most frequently reported AEs were constipation (64%, 7/11), neutrophil count decrease (45%, 5/11), peripheral edema (36%, 4/11), platelet count decrease (36%, 4/11), thrombocytopenia (36%, 4/11), and white blood cell count decrease (36%, 4/11) (Table 3). Of non-ocular AESIs, the incidence of any grade thrombocytopenia (thrombocytopenia and platelet count decreased) was slightly greater in the PVd group (64%, 7/11) than in the BPd group (60%, 6/10). No infusion-related reactions occurred in the BPd group. The incidence of infections was 70% (7/10) in the BPd group and 36% (4/11) in the PVd group, with grade ≥ 3 infections reported in 40% (4/10) and 18% (2/11), respectively (Table S4). In the BPd group, grade ≥ 3 infections were pneumonia (2 patients), cytomegalovirus chorioretinitis (1 patient), and Morganella morganii infection (1 patient). In the PVd group, grade ≥ 3 infections were pneumonia and influenza (1 patient, each).
Table 3 Adverse events by preferred term in ≥ 20% of patients in either treatment group (safety population)At data cutoff, 90% (9/10) of patients in the BPd group experienced CTCAE-graded ocular AEs compared to 9% (1/11) in the PVd group; all ocular AEs were treatment-related (Table 4). The most frequently reported ocular AEs with BPd were blurred vision (90%, 9/10), foreign body sensation in eyes (40%, 4/11), dry eye, and eye irritation (20%, 2/10 each). Grade 3 ocular AEs were reported in two patients in the BPd group, both experiencing blurred vision, and none were reported in the PVd group; no grade 4 ocular AEs were reported. Ocular AEs did not lead to treatment withdrawal or dose reductions in both treatment groups. CTCAE-graded ocular AEs led to dose interruptions or delays in 44% (4/9) of patients who received BPd and none in those who received PVd. The first occurrence of ocular AEs in the BPd group were resolved prior to the end of treatment exposure in 56% (5/9) of patients. Of the four patients with unresolved events, one patient’s event (blurred vision, grade 2 or below) remained unresolved at the end of follow-up (study withdrawal) and was managed without dose modification; the remaining three patients had unresolved events at the data cutoff and remain in follow-up.
Table 4 Ocular and corneal events (safety population)Corneal events as defined according to the KVA scale were reported in 90% (9/10) of the patients who received BPd, where 50% (5/10) experienced a KVA grade ≥ 3 event (Table 4). KVA-defined events led to a dose reduction in 50% (5/10) of the patients who received BPd, and a dose interruption or delay in 80% (8/10) of the patients. Of the 8 patients with grade ≥ 2 KVA-defined events, 6 patients had their first event resolved prior to or after the end of treatment exposure and 2 patients remain in follow-up (Fig. S2).
Comments (0)