Summary and interpretation of the results
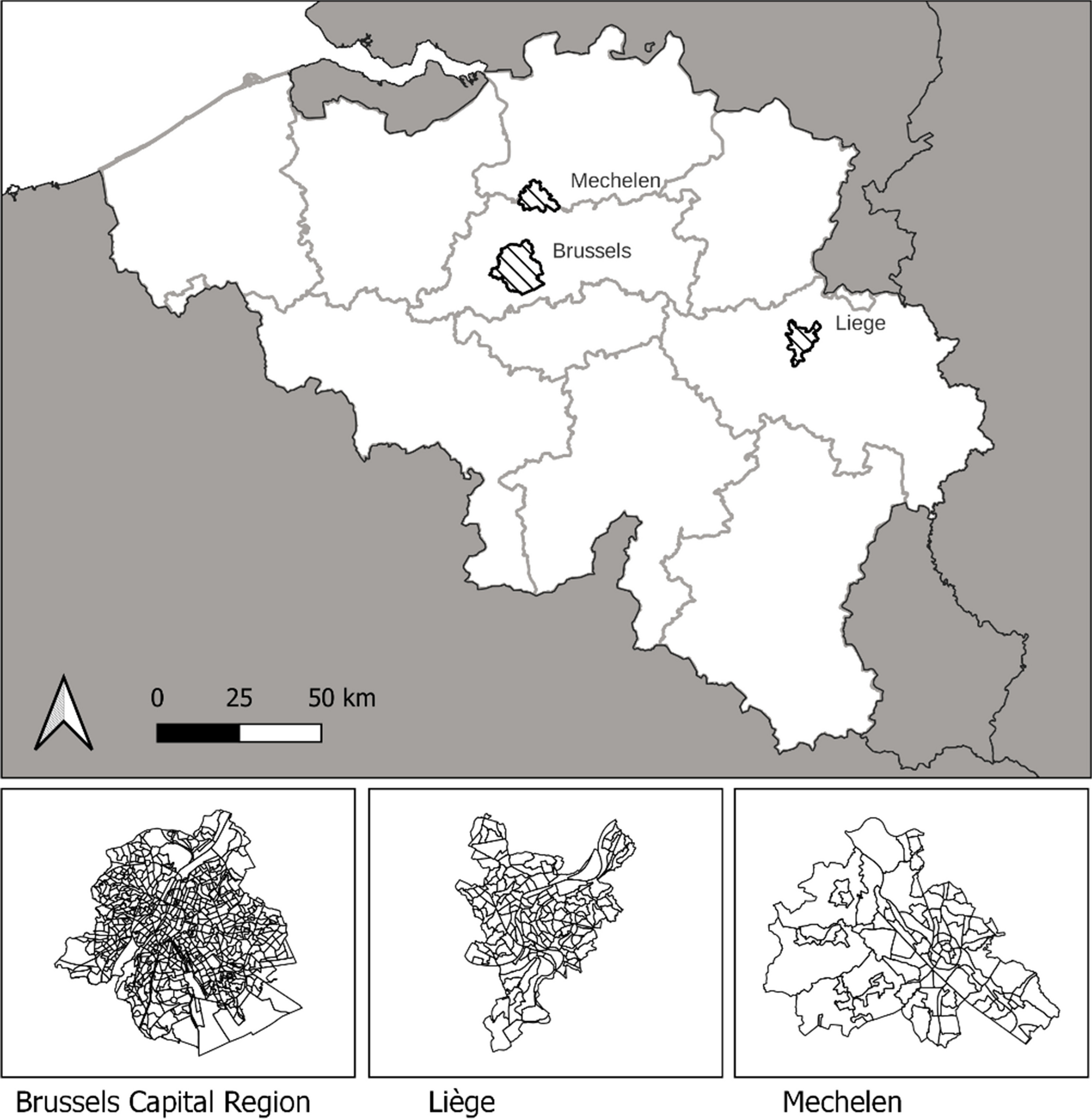
A strong correlation was found between air pollution, lack of green space, and adverse health outcomes in Mechelen, Liège, and Brussels. As is known from the literature review, cardiovascular mortality, diabetes, and asthma show varying degrees of correlation with environmental conditions. Population-weighted averages indicate that achieving WHO guidelines for air pollution and green space could significantly reduce diseases, including total mortality, cardiovascular mortality, diabetes, asthma, and depression.
Spatial analyses of the PF under current conditions reveal notable disparities within cities, with urban centres bearing a higher disease burden. Socio-economic factors, assessed through the BIMD, strongly correlate with health impacts, emphasising the complex interaction between environmental and social determinants of health.
The analysis of air pollution at measurement stations in Mechelen, Liège, and Brussels shows that relying solely on background concentrations, as implemented in the commonly used SHERPA tool, can lead to substantial underestimations of NO2 levels from traffic, sometimes by over 50%. This could result in policy analyses underestimating the health burden and the mitigation potential of urban and transport planning-related interventions. In contrast, PM2.5 concentrations from traffic are lower, with only modest underestimations at very busy traffic locations. However, for PM2.5, not applying traffic-specific dose–response functions may be a source of underestimation of the traffic-related disease burden.
Our research, even from a purely mathematical perspective, highlights the impracticality of achieving WHO air pollution targets (5 µg/m3 for PM2.5 and 10 µg/m3 for NO2) in urban contexts without substantially reducing traffic-related emissions. Furthermore, the prevalent allocation of urban spaces to vehicles, often at the cost of green areas, exemplifies poor urban and transport planning from a health standpoint. This lack of green spaces negatively affects health outcomes. Mechanisms involved here are potential direct effects of green spaces such as mitigating mental stress, improving social interactions, and enhancing microbial diversity. In addition, a higher availability of green spaces increases physical activity and reduces urban heat islands (Yang et al. 2021). Insufficient green space not only contributes to the development of urban heat island effects but also adversely affects the physical activity levels of urban residents (Choi et al. 2022; Iungman et al. 2023; Wang et al. 2021).
Earlier studies focusing on Barcelona and Vienna found that 20% and 8% of mortality, respectively, could be prevented through urban and transport planning considering air pollution, green space availability, physical activity levels, noise, and urban heat islands, with air pollution and physical activity being the most important factors (Khomenko et al. 2020; Mueller et al. 2017). However, these studies were based on now outdated recommendations of 40 µg/m3 NO2 and 10 µg/m3 PM2.5 exposure limits, and thus underestimate the mitigation impact under the new WHO guidelines of 10 µg/m3 NO2 and 5 µg/m3 PM2.5 exposure.
Strengths and limitations
Our study has several strengths. The results align with the research objectives, offering clear insights into the (preventable) disease burden linked to urban and transport planning practices. We identified important gaps in air pollution source allocation methods that could enhance mitigation strategies. The underestimation of NO2 levels from traffic highlights a crucial issue in current methodologies, which must be addressed to improve the accuracy of HIAs. Future research should focus on developing and validating techniques that more accurately quantify traffic-related pollution. Another strength of our study is its focus on the health burden of specific diseases, such as cardiovascular mortality, asthma, diabetes, and depression, rather than only assessing total mortality. A profound understanding of the impact on individual diseases is essential for effective mitigation.
Beyond these elements, this study advances previous HIA work in several important ways. It applies the framework to small and mid-sized Belgian cities such as Liège and Mechelen, which are rarely analysed in European research dominated by large metropolitan case studies. It also uses a high-spatial-resolution approach that enables neighbourhood-level assessment of preventable disease burden, providing more granular insights into intra-urban differences. By linking environmental exposures with socio-economic deprivation indicators, the study highlights inequalities in environmental health risks that remain invisible in aggregate analyses. Together, these advances provide a more policy-relevant perspective, helping to identify where and for whom urban and transport interventions could yield the largest health benefits.
Despite its strengths, however, our study has limitations, primarily due to data gaps and the lack of robust source allocation methods. This restricted our analysis to measuring the disease burden from traffic-related air pollution only at specific reference stations, rather than across entire cities, making it challenging to convert attributable factors to common indicators like disability-adjusted life years (DALYs). Key aspects such as the impact of physical inactivity and the urban environment on food consumption, safety, and general well-being are still missing for a complete understanding. Achieving zero-exposure concentrations is unrealistic, particularly due to natural particulates like soil dust and sea salt (in coastal areas), and traffic emissions contributing to secondary particulate matter. Therefore, we selected WHO target values for air pollution as the counterfactual scenario instead of zero exposure. However, the limit values of 5 µg/m3, and particularly 10 µg/m3, are not natural thresholds beyond which no progress can be made, as lower concentrations are observed in regions like Scandinavia. In 2015, the lowest observed annual values in Europe were 3.7 μg/m3 for PM2.5 and 3.5 μg/m3 for NO2 (Khomenko et al. 2021). In addition, the use of a two-pollutant model adjusted for PM2.5 may attenuate the estimated NO2 effect, as both pollutants share substantial variance in traffic-related exposures, including black carbon as a key fraction of PM2.5. This approach provides a conservative estimate of the potential health gains from achieving the WHO NO2 guideline, since part of the shared mixture effect is removed when both pollutants are modelled simultaneously. When both NO2 and PM2.5 are mutually adjusted, the resulting ERFs may therefore not fully capture the total traffic-related burden, while unadjusted models could overestimate it. In contrast, adjustment of PM2.5 for NO2 generally has a smaller influence, as PM2.5 originates from a multitude of sources beyond traffic, including residential heating, industry, and agriculture. Overall, the reported PFs should be interpreted as conservative and prudent lower-bound estimates. Sensitivity analyses using the unadjusted NO2 ERF are presented in Appendix IV, confirming that higher PFs are obtained when the PM2.5 adjustment is omitted. The ERFs for both mortality and morbidity were derived from large European multi-cohort studies that almost always included comparable adjustments for key individual and socio-demographic factors such as age, smoking, body mass index, and neighbourhood income. These ERFs therefore represent population-weighted, broadly generalisable estimates for the European adult population. When applied at the city level, modest deviations may occur due to local demographic or health characteristics, but they provide a robust basis for comparing preventable mortality and morbidity attributable to air pollution across cities.
Further, we assume a sub-additive effect through the multiplicative PF, while some studies note the possibility of synergistic effects of unfavourable outcomes from combined exposure to suboptimal environmental conditions (Vandeninden et al. 2024). Lastly, The NDVI data used in this study correspond to the year 2016, whereas air pollution data were obtained for 2022, which introduces a temporal mismatch between the datasets. However, comparisons of other consistent land-cover datasets (e.g. CORINE Land Cover 2012 vs. 2018) indicate that land-use changes in Brussels, Liège, and Mechelen have been minimal over this period. It is therefore reasonable to assume that overall green space patterns remained largely stable between 2016 and 2022. While small local greening projects may not be captured, this limitation is unlikely to affect the overall magnitude or direction of the results.
Implications for research and policy
The findings of this study have implications for both future research and policymaking in the realm of urban and transport planning. Firstly, the clear linkage between air pollution, lack of green space, and various health outcomes necessitates a re-evaluation of urban planning priorities. Policies aimed at reducing air pollution, particularly NO2 and PM2.5, and increasing green spaces in urban areas could significantly diminish the disease burden from asthma, diabetes, depression, and cardiovascular diseases. This is especially pertinent in densely populated urban centres, and adjacent suburbs, where the study identified the highest health risks, and where a mitigation of a lack of green space and reducing NO2—the traffic-related component of air pollution—can result in strong health gains for the residing population. A recent meta-analysis (Kuss and Nicholas 2022) investigated the effect of mitigation measures on car use in cities and found that congestion charging, parking and traffic control, zones with limited traffic, investments in public transport and making public transport more affordable or free, and apps for sustainable mobility all result in reductions in car use of more than 10% each.
Considering the broader context of integrated urban and transport planning, the adoption of electric vehicles, while beneficial in certain aspects, including reducing NO2 exposure, falls short in addressing key urban environmental challenges. In 2020, 50% of PM2.5 in the EU originated from non-exhaust emissions such as brakes and tyres, with an increasing trend of PM2.5 non-exhaust emissions and a decreasing trend of PM2.5 exhaust emissions (European Topic Centre on Air pollution, Transport, Noise and Industrial Pollution, 2020). Transitioning to electric vehicles does not curtail the emission of non-tailpipe PM2.5 particles, nor does it mitigate the extensive spatial demands of urban transportation infrastructure. This continued space consumption hinders the expansion of green areas, which is crucial for reducing urban heat island effects and fostering increased physical activity among city dwellers (Dávalos et al. 2016; Nieuwenhuijsen 2023).
This study underscores the need for advanced source allocation methods in environmental health research, emphasising that current approaches may underestimate NO2 levels from traffic. Future research should prioritise the refinement of these techniques to more precisely measure traffic-related pollution and improve HIAs. Policymakers and urban planners can utilise these insights to develop more effective strategies for urban design and transport management, ultimately leading to healthier cities and communities.
More detailed discussion of policy relevance and effectiveness of selected urban and transport measures
Low emission zones (LEZs) remain among the most widely discussed urban traffic measures. Across European cities, LEZs result in varying reductions in NO2 and PM concentrations. In some countries and LEZ zones, such as in the Netherlands, significant differences were not observed, while in other areas such as Germany, the LEZ typically reduced NO2 and PM concentrations by a few percent. In London, the ULEZ reduced PM10 by 27% and NO2 by 12.4% (Broster et al. 2025; Holman et al. (2015). In London, introduction of the ULEZ is estimated to result in a reduction in the incidence of childhood asthma of up to 8% in some neighbourhoods such as Camden and Kenningston and a 6% reduction in coronary heart disease, 5% reduction in low birth weight, and 2% reduction in diabetes in the same neighbourhoods (Holman et al. (2015). In Brussels, the LEZ reduced NO2 by 30% in the highest-traffic routes, with projections suggesting an additional 24% decline by 2035 (Pelgrims et al. 2024). LEZs also tend to yield larger benefits in more deprived neighbourhoods, thus contributing to environmental equity (Pelgrims et al. 2024). However, LEZs primarily affect air pollution and traffic emissions and do not directly increase green space availability.
Similarly, congestion charging schemes achieve 10–20% reductions in traffic volumes and accompanied decreases in air pollution levels. It is estimated that in the inner city of Stockholm, there are 20–25 fewer premature deaths annually due to the congestion charging policy introduced in 2005. Public support for the policy rose sharply after it was implemented compared to 2005 when the policy was introduced. Further, congestion charging generates public revenue to reinvest in sustainable transport such as public transport, which could further result in indirect positive effects on health (Eliasson 2014). However, although effective for emission reduction, congestion charging has limited direct effects on urban greening, unless revenues are explicitly allocated to public space redesign.
Investments in public transport and active mobility deliver broader and longer-term benefits. Scenario analyses for the city of Barcelona show that replacing 40% of car trips by cycling and public transport could prevent around 76 premature deaths annually through combined effects of reduced air pollution and increased physical activity (Rojas-Rueda et al. 2013). In cities such as Granada and Ljubljana, the implementation of integrated low-traffic and public transport improvement measures, including the closure of streets to private vehicles, renewal of bus fleets, and reorganisation of public transport routes, resulted in substantial air quality benefits, with reductions of up to 72% in local black carbon (BC) and 30% in PM10 concentrations (Pelgrims et al. 2024).
School Streets interventions consistently demonstrate localised air quality benefits and associated health improvements: specifically, a 23% decrease in NO2 peak exposure was observed outside of schools in London, alongside a 25% decrease in NO2 concentration in Paris between 2021 and 2023, with this reduction in peak exposure in Flanders being associated with a decrease in airway inflammation among children near the school environment (Pelgrims et al. 2024).
Car-Free Sundays, as a form of local traffic restriction, have demonstrated significant public health benefits, achieving substantial localised NO2 reductions ranging from 63% to 83% in parts of Brussels and 27% to 56% in Paris. This was associated with an estimated reduction in paediatric asthma incidence up to 34% in heavily trafficked areas of Brussels, if those local traffic restrictions were implemented permanently.
Further, there is considerable potential in finding space for nature and green areas in cities by converting redundant car parking:for example, reducing the number of parking spaces in a city or converting parking spaces to underground parking spaces (Croeser et al. 2022). This is associated with a range of physical and mental health benefits including reducing loneliness and obesity (Croeser et al. 2022). Urban green infrastructure, such as street trees, parks, and green roofs, provides benefits in both air quality and well-being (World Health Organization Regional Office for Europe 2017).
In the city of Paris, it was demonstrated that reducing lane capacity (for cars) by percentages up to 50% resulted in a modal shift towards active mobility without an overall increase in congestion (Natterer et al. 2025). This is presumably resulting in a wide range of health benefits, from both reduced pollution and increased physical activity. Reducing lane capacity also allows for the implementation of more urban green spaces.
The increasing number of cities that have successfully implemented these measures indicates that these strategies are feasible and politically achievable under a range of local conditions. While implementation costs can vary, many interventions—such as LEZs, congestion charging, and School Streets—rely primarily on regulatory and organisational changes rather than large infrastructure investments. Moreover, measures that generate revenues (e.g., congestion charges) or co-benefits across multiple policy domains such as investments in public transport and active mobility (e.g., health, climate, equity, economy) tend to be cost-effective in the long term.

Comments (0)