
Remember me
This was a non-interventional, prospective, multi-center study aimed at assessing vaccination coverage among residents of eight long-term care facilities (LTCF) in the south of Poland, including both residential and nursing homes. Data were collected between January and June 2022 by trained medical staff. The criteria for participants’ inclusion were the ability to provide informed consent and residency in LCTF. All participants have provided informed consent. Each participant was asked to complete a survey, followed by the collection of a blood sample.
The questionnaire included several sections covering sociodemographic data, medical history (including medications, comorbidities, and lifestyle factors), issues related to aging such as mobility limitations, frailty assessment scale, Barthel Index, and questions related to COVID-19 and its complications. Previous symptomatic or asymptomatic COVID-19 cases, along with their severity, and vaccination status were determined on the basis of medical documentation. Participants without confirmation of SARS-CoV-2 infection were classified as uninfected.
For calculation of time between the last documented exposure to COVID-19 and blood collection we defined the “last documented exposure to SARS-CoV-2” as either the last dose of COVID-19 vaccine or SARS-CoV-2 infection.
The Barthel Index served as the basic tool to measure activities’ performance. Antibody levels of residents were analyzed according to subgroups based on the Barthel scale on the day of the examination:
1 – severe disability, < 40 points,
2 – moderate disability, 40–55 points,
3 –low disability, 60–85 points,
4 – no disability, 90–100 points.
Furthermore, participants were categorized on the basis of medical staff assessment into physically independent residents (IRs)—walking without any help, using walking sticks or crutches, using a walking frame, and physically dependent residents (DRs)—walking with assistance, using a wheelchair, or bedridden.
SerologyBlood samples from patients were collected in tubes without anticoagulant. After collection, the tubes were allowed to coagulate for 30 to 60 min at room temperature. Subsequently, the clotted blood was centrifuged for 8 min at 1250 rpm. The serum was then aliquoted and frozen at −80 °C until use. Anti-SARS-CoV-2 antibodies IgG were determined with commercial enzyme-linked immunosorbent assays (Euroimmun, Lubeck, Germany) according to the manufacturer’s instructions, using the microplate reader (BioTek ELx808 and Multiskan FC Thermo Scientific).
The data were interpretated on the basis of the manufacturer’s recommendation using the Ratio factor. The recommended interpretation of the results was as follows: < 8 relative units per milliliter (RU/ml) – negative, ≥ 8 to < 11 RU/ml – borderline, ≥ 11 RU/ml – positive. Owing to the low negative outcome total count, in further analysis that variable was used as a continuous variable.
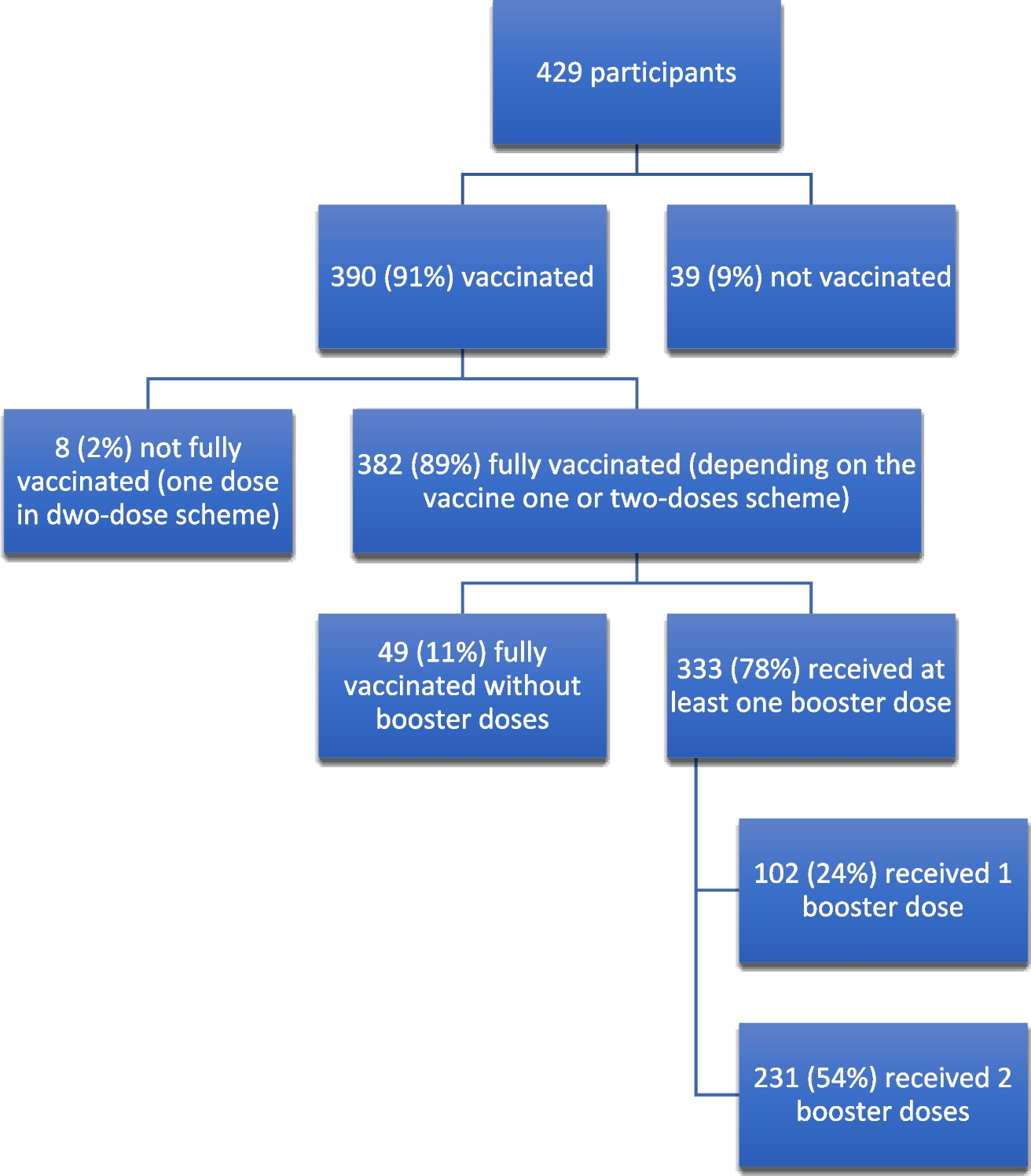
VaccinationAll residents were vaccinated with mRNA vaccines or vector vaccines: 94% received Comirnaty (BioNTech and Pfizer), 3.7% received Jcovden (Janssen), 1.6% received Vaxzevria (AstraZeneca), and 1% received Spikevax (Moderna) (Fig. 1). According to WHO recommendations the basic vaccination with Comirnaty was given at a schedule of two doses (30 µg, 03 ml each) 3 weeks apart, Spikevax also two doses (100 µg, 0.5 ml each) 8 weeks apart, similarly Vaxzevira two doses (0.5 ml each) 8 weeks apart and one dose (0.5 ml) of Jcovden (p. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines) (COVID-19 vaccines n.d.). All booster doses were given with the Comirnaty (BioNTech and Pfizer) vaccine.
Fig. 1
Prevalence of vaccination against COVID-19 considering number of doses among resident of long-term care facilities
A follow-up study was conducted in September–December 2022. We collected additional data about COVID-19 cases and booster doses administered after blood collection. We put together residents who received one booster dose with residents who received two booster doses, as only six participants received two booster doses before blood sample collection.
StatisticsIn the statistical analysis, relative and absolute frequencies were used for nominal variables, and the mean value with standard deviation for quantitative variables. For non-normal distribution of data, median with interquartile range (IQR) was used. The chi-squared test and Student’s t-test were employed to compare patient groups (with Yates correction). The analysis was conducted using the International Business Machines Corporation Statistical Package for the Social Sciences, version 29 (IBM Corporation, Armonk, USA). In all analyses, the significance level was set at α = 0.05.
Comments (0)