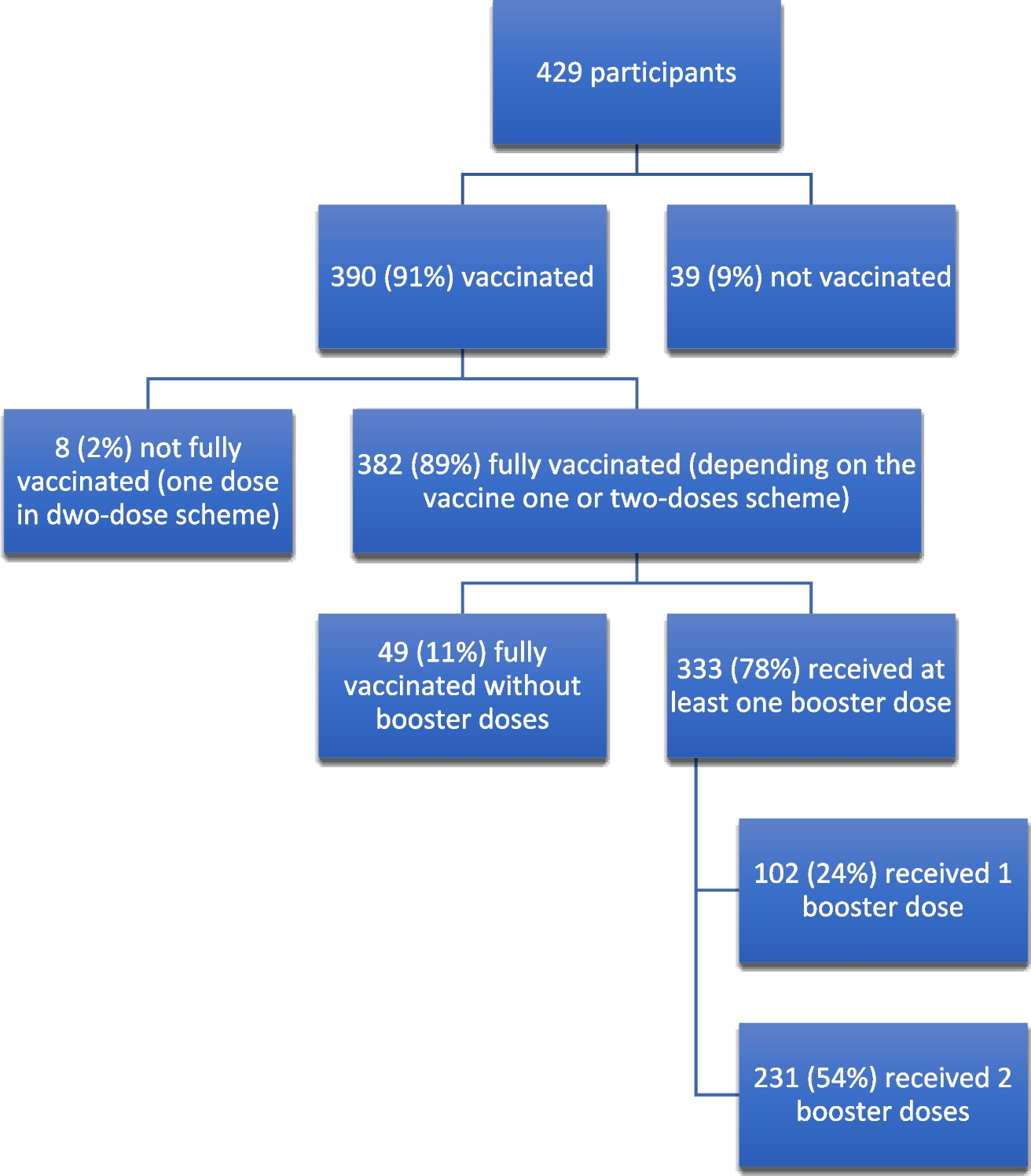
A non-randomized controlled intervention trial was conducted to examine the effects of the ‘10,000 Steps Duesseldorf’ intervention on two samples of adults aged 25 to 75 at baseline and after one year. At baseline, a total of 627 participants were enrolled, with 376 individuals as part of the intervention group in Duesseldorf and 251 of the control group in Wuppertal. After one year, follow-up assessments were conducted in 553 participants (330 in the intervention and 223 in the control group). The intervention targeted multiple levels, including the individual (e.g., website access), the organizational (e.g., physical activity promotion in companies), and the community level (e.g., media campaigns and environmental changes). This study replicated the ‘10,000 Steps Ghent’ intervention, preserving its core principles, while adapting it to the local context of Duesseldorf (Matos Fialho et al. 2022; Pischke et al. 2024).
The ‘10,000 Steps Ghent’ study included a process evaluation based on the RE-AIM framework (Glasgow et al. 1999) to assess the intervention’s reach, adoption, implementation, and maintenance. Specifically, heads of departments from 69 organizations completed an online survey to evaluate their awareness of the project, adoption of intervention strategies, the implementation processes, and their intention to maintain the intervention. Additionally, 755 citizens from the areas influenced by these organizations were surveyed to assess their knowledge of the project and their PA-levels (Van Acker et al. 2011).
Following this approach, in our study, we also conducted a process evaluation using the RE-AIM framework to ensure comparability with the original ‘10,000 Steps Ghent’ study. The evaluation examined the following key components: reach, effectiveness, adoption, implementation, and maintenance. Data were collected via a questionnaire distributed across multiple settings, including companies and senior citizen organizations.
Intervention adaptation
The study began with a six-month participatory phase aimed at recruiting key stakeholders from the city of Duesseldorf to form an advisory council that would support the research team in adapting and implementing the intervention. The relevant stakeholders included representatives from local communities, the public health service, the city's administrative departments for sports and social services, two mandatory health insurance providers, and the Chamber of Industry and Commerce (Industrie- und Handelskammer (IHK) of Duesseldorf, as well as various companies, the Medical Chamber, and the city's professional soccer club (Fortuna Duesseldorf)).
These stakeholders were invited to join the advisory council during the first two months of the participatory development phase. In the following four months, monthly meetings were held to adapt the intervention from Ghent to the context of Duesseldorf and to develop a collaborative strategy for its implementation. During these meetings, ideas pertained to intervention activities and the necessary steps for implementation were discussed and continually prioritized. The meetings continued throughout the implementation phase of the intervention.
Intervention components and implementationOrganization of events in Duesseldorf
A range of community events focusing on promoting PA were organized, including the ascent of the Duesseldorf Television Tower (Skyrun), a family event at the local soccer stadium with representatives from the soccer team, and city rallies with various local themes related to arts, culture, and history. Additionally, the project was linked to existing events, such as those organized by Duesseldorf’s Administrative Office for Sports, city marathons, and health promotion events hosted by other organizations. These events were publicized via press releases, the project’s website, the city of Duesseldorf website, and social media channels, including the project’s own Instagram channel and those of the stakeholder advisory board members. The main intervention message, “Every step counts” was disseminated through various media channels and displayed in public spaces to maximize its reach.
Website
The website's content incorporated various behavior change techniques, including goal setting, highlighting the gap between current behavior and target standards, self-monitoring, and social comparison. Information about the benefits of regular PA and tips on how to integrate more steps into daily routines were provided. Recommendations for step counters, trackers, and apps to monitor steps were also included. Current events in the city that promoted PA, planned as part of the project, were advertised on the website and regularly updated along with existing city-organized events. Additionally, users could create personal profiles to track daily steps, receive weekly summaries, convert other activities (e.g., swimming and cycling) into step equivalents, and compare their step counts with those of other participants in challenges or competitions organized by the research team. Participants (and organizations participating in the intervention) could also set up their own step competitions with family, friends, colleagues, or other registered users.
Social media (Instagram/Facebook/Komoot)
We utilized social media platforms, specifically Instagram, Facebook, and Komoot, to promote PA goals according to the recommendations of the WHO and encourage participation in outdoor activities. Our approach involved posting identical content across both Facebook and Instagram to maximize our reach across different age groups, as studies suggest that distinct age demographics tend to favour one platform over the other (Laor 2022). Facebook attracts a more mature audience, while Instagram is particularly popular among younger individuals (Bui 2022). By posting on both platforms, we aimed to expand our outreach and better connect with diverse segments of our target audience.
The content shared on these platforms covered a wide variety of topics, primarily focusing on the achievement of PA goals. We highlighted how individuals can organize their daily PA in ways that are personalized to their lifestyles. A key component of this was the involvement of the ‘10,000 Steps Duesseldorf’ team demonstrating how everyday activities, such as walking, cycling, and other simple movements, can contribute to meeting PA targets. These contributions were collected in the form of short written sentences or reflections, offering authentic and diverse perspectives. This not only fostered engagement with the advisory council but also served to inspire the audience by showcasing real-life examples.
To keep the content engaging, we employed a variety of formats across both Instagram and Facebook, including photos, videos, stories, and guides. Each format was used to present different aspects of the initiative, from informational content about exercise (e.g., health benefits, recommended routes, and tips) to motivational messages designed to encourage a more active lifestyle. We also used these platforms to inform our audience about upcoming events, both organized by our team and by external partners. Events, such as the opening of a mobility station (an integrated transport hub that offers options, such as bicycles, scooters, public transport, and car sharing, to facilitate sustainable urban mobility), and the Volksgarten parkrun (a free, communal, weekly 5 km run or walk) were highlighted to keep the audience informed about local opportunities to participate in community events targeted at PA (full list of events in Table 1).
Table 1 10,000 steps eventsOur content strategy also included promoting our website, especially the step count challenges and step competitions that were available to our followers. These interactive elements aimed to engage the audience in friendly competition while promoting an active lifestyle. In addition to Instagram and Facebook, we utilized Komoot, a popular route planner and navigation app, to encourage participants to explore and create their own outdoor routes. Komoot serves as a social network for outdoor enthusiasts, particularly cyclists, hikers, mountain bikers, gravel bikers, and road cyclists. As part of our initiative, we created 30 routes, some in collaboration with steering committee members (working groups that developed strategies for implementing the intervention (Pischke et al. 2024)) and others with local partners. These routes varied in difficulty and length, offering options for different levels of fitness and interest.
Park signage and print media materials
As this is a replication study, the intervention materials (Pischke et al. 2024) were adapted based on the original study (De Cocker et al. 2007). Print media, flyers, booklet with step-count logs, stickers, and posters were created. The intervention material was available for download on the website and was distributed by student assistants at 3-month intervals in offices of general practitioners, physical therapists, pharmacies, newsstands and senior citizen centers located in the intervention city districts.
Baseline and follow-up assessments
The planned controlled intervention study aimed to recruit 399 participants each from Duesseldorf and Wuppertal, requiring initial contact with 2,500 people in each city. Due to a lower-than-expected response, possibly due to the COVID-19 pandemic, an additional 4,000 people were contacted, bringing the total to 9,000 potential participants. The baseline survey period started in May 2021 and ended in January 2022. Travel restrictions at the university hospital delayed the kick-off event marking the start of the intervention and the completion of the website. Eventually, 627 interviews were completed by March 17, 2022. The intervention was set to begin in January 2022, but was delayed due to the website's delayed launch, which finally went live on April 7, 2022, missing some planned functions. The feature allowing participants to create their own step competitions was completed by May 30, 2022, after which all intervention content was fully implemented. The follow-up period started in May 2023 and ended in October 2023. A total of 553 participants were interviewed in this phase, with the last interview conducted on October 30, 2023. Main results are reported elsewhere (Matos Fialho et al. 2025).
Process evaluation
As part of a process evaluation, the scope and intensity of intervention activities at each level of the complex intervention were documented over a one-year period. Data were collected via an online questionnaire distributed across various settings, including companies and senior citizen organizations. The five framework components were measured in detail following Van Acker et al. (2011); however, full calculations were hindered by limited and incomplete survey participation. Originally, the following approach was foreseen: Reach would be assessed by calculating the proportion of people aware of the intervention compared to those unaware. Adoption would be gauged by determining both the proportion of organizations that implemented the intervention (and those who chose not to) and their representativeness. Implementation fidelity for each of the nine intervention components was to be assessed, with a calculated implementation score (ranging from 0 to 100) to reflect the degree of adherence. Finally, maintenance was to be assessed by calculating the proportion of organizations intending to sustain the intervention. The questionnaire comprised four main sections: (1) characteristics of the respective organization and knowledge of the intervention, (2) adoption of the intervention and reasons for or against adoption, (3) implementation of the intervention, and (4) long-term maintenance of the intervention. Examples of survey items included are shown in textbox 1 (Matos Fialho et al. 2022).
Textbox 1 Example items of the web-based questionnaire used in the process evaluation (Matos Fialho et al. 2022).
1. Characteristics of the respective organization and knowledge of the intervention
• In which organization do you work?
• How many permanent employees does your organization have?
2. Adoption of the intervention and reasons for or against adoption
• Did your organization participate in 10,000 Steps Duesseldorf?
• What contributed most to the decision to carry out 10,000 Steps Duesseldorf?
• What are the main reasons why 10,000 Steps Duesseldorf was not implemented?
3. Implementation of the intervention
• How many employees worked on the implementation of 10.000 Steps Duesseldorf?
• What was or is the total investment, excluding staff costs, for your organization to implement 10,000 Steps Duesseldorf?
• Did you distribute the intervention materials (stickers, brochures, flyers) of 10,000 Steps Duesseldorf?
• Which media channels did you use and at what cost?
4. Long-term maintenance of the intervention
• Does your organization intend to plan further intervention activities in the future following the past or current 10,000 Steps Duesseldorf activities?
• Why are no 10,000 steps Duesseldorf intervention activities planned for the future?
The first step in the data collection process for the evaluation of the ‘10,000 Steps Duesseldorf’ intervention was to establish a core sample population. Given the nature of this process evaluation, the entities to be surveyed were selected from specific city districts in Duesseldorf (Flingern Nord, Flingern Sued, Oberbilk, Friedrichstadt, Gerresheim, Eller, and Wersten). The focus was primarily on companies, medical practices, and non-profit organizations. Information and addresses of these entities were sourced from the official website of the City of Duesseldorf. To refine the target group, only companies and medical practices with at least 20 employees were included. The collected data were compiled in a structured database which included details, such as addresses and the number of employees for each entity.
a.) Telephone-based interviews: The survey questions were adapted based on the process evaluation by Van Acker et al. (2011) allowing for the development of relevant and tailored questions for this evaluation. These questions were then programmed into the survey software Qualtrics and included in the overall assessment of the study via telephone-based interviews (Matos Fialho et al. 2022).
b.) Online-survey and in-person interviews: The primary component of the process evaluation consisted of interviews with organizations which were conducted through online surveys. This approach was adopted to replicate the methods employed in the original study (Van Acker et al. 2011). The evaluation process took place from May 2023 to January 2024. The organizations were contacted via email, and those responsible for the sector were requested to respond. However, due to the low response rate, a new approach was adopted. Instead of receiving responses via email, the selected addresses were visited in the districts by interviewers. After providing a brief introduction to the project, they requested participation in the survey. Agreed-upon interviews were conducted on-site with the designated contact persons. After each contact attempt, the results were systematically recorded. General information, such as the date and name of the organization, was documented, along with details on whether an interview was conducted. When an interview was not completed, the reasons were categorized. Entries were marked as "not found" when the address appeared incorrect or when it was unclear if the organization was present (e.g., no visible doorbell or unanswered door). The category "no contact person/no time" was used when initial contact was made, but the organization declined participation. This categorization helped to provide an overview of response patterns and informed strategies to reduce the refusal rate. The dataset of completed surveys was exported and processed using Qualtrics.

Comments (0)