
Remember me
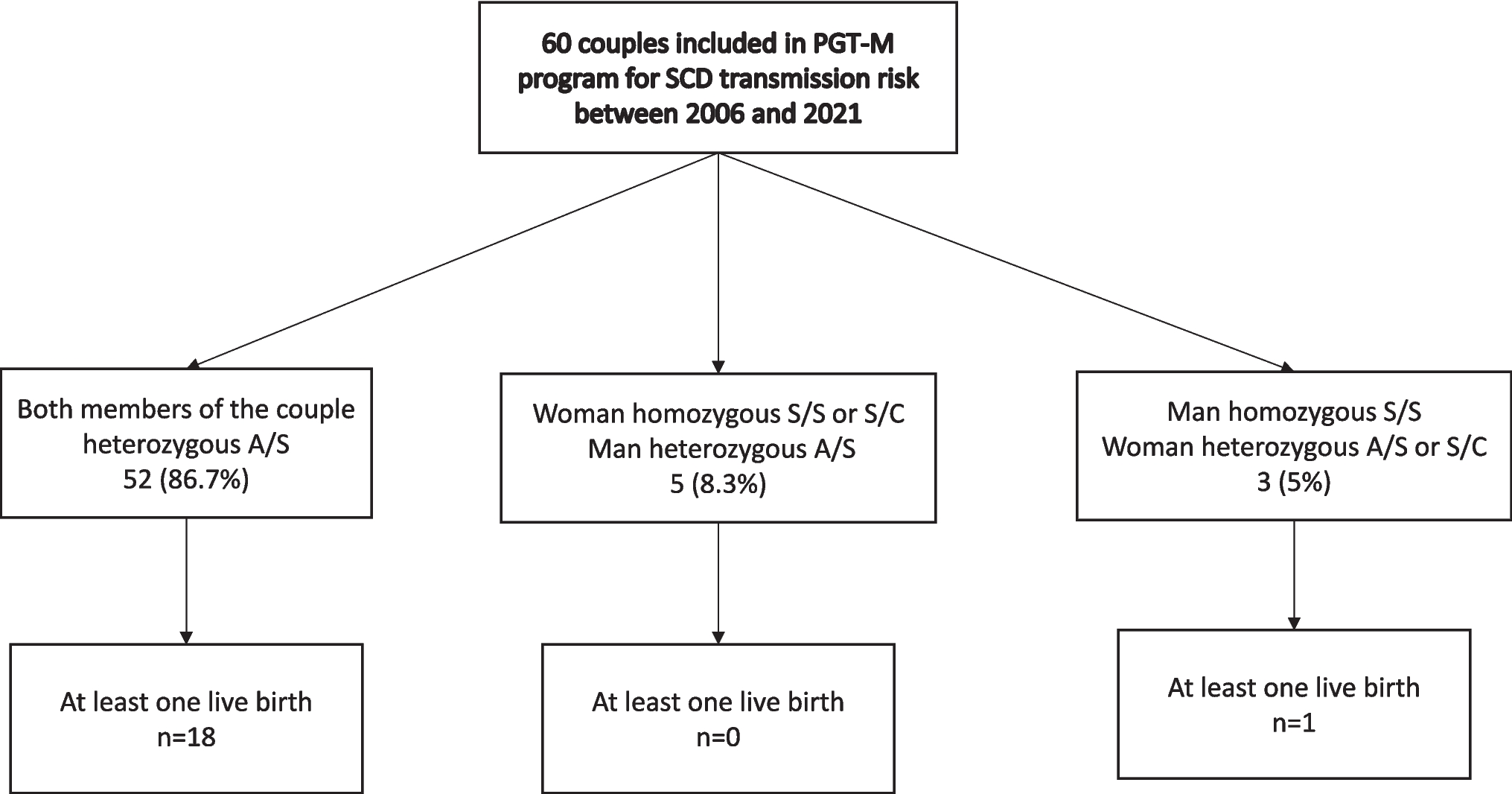

In total, 60 couples were treated under the PGT-M program for SCD transmission risk between 2006 and 2021 at our PGT center (Fig. 1). The population description and the characteristics of the couples at the start of PGT-M procedure are described in Table 1. For 8 couples (13.3%), one partner suffered from SCD (SS or SC Genotype) (5 women and 3 men), so that the theoretical transmission risk of SCD was 50%. The majority of women (n = 48; 80%) were of African origin. Before the PGT procedure, 35 couples (58.3%) had at least one child affected by SCD (SS), and 17 of them (48.5%) requested PGT with HLA typing. A total of 19 couples (32%) had previously undergone a pregnancy termination for SCD prior to starting the PGT-M treatment. At the time of the first stimulation, the median age of women was 33 [31–35] years versus 39 [33–40] years for the men.
Fig. 1
Flowchart of all couples in PGT-M program for SCD transmission risk between 2006 and 2021
Table 1 Description of the population and characteristics at the time of the first PGD-M attempt (n = 60)Outcomes of the entire PGT programThe outcomes of the couples’ journey through PGT-M for SCD are detailed in Table 2 and Supplemental Table 1. During their PGT process, more than half of the couples (n = 34; 56.7%) underwent at least two ovarian stimulation cycles, while 45 couples (75.0%) had at least one fresh embryo transfer. A total of 21 frozen embryo transfers were performed for 13 couples (21.6.%). Four couples (6.7%) never had oocyte retrieval, and 11 couples (18%) were unable to have either a fresh or frozen embryo transfer. A total of 505 embryos were biopsied, and a diagnosis was obtained for 474 of them (93.9%). Among the diagnosed embryos, 261 (55.1%) were genetically unaffected, of which 172 (65.9%) were suitable for fresh or frozen embryo transfer. Detailed embryos results according to transmission risk are presented in Table 3.
Table 2 Flow of IVF–PGT-M cycles and outcomes according to sickle cell statusTable 3 Embryo’s outcomes according to the transmission riskAt the end of the PGT-M process, 19 couples (31.7%) had at least one live birth, including 4 couples who underwent PGT-M for SCD and HLA typing, of whom one had an HLA-unmatched embryo. Of the 19 couples who had a live birth, 15 achieved this after a fresh embryo transfer and the remaining four after a frozen embryo transfer.
PGT-M outcomes for affected womenFor five couples in the PGT program, the woman was affected by SCD, four of them having experienced at least one pregnancy prior to entering the program, and three already had one child. One woman had SC genotype, while the remaining four were SS. Two women presented with renal involvement and one had ophthalmic complications. None of the five women were receiving hydroxyurea at the time of the protocol, had previously undergone HSCT, or had received exchange transfusions prior to inclusion. All of these women were evaluated and cleared by their hematologists to become pregnant. They also benefited from personalized management protocols adapted to their clinical condition before COH. These protocols were developed in collaboration with hematologists and anesthesiologists and included specific preventive measures such as systematic hydration protocols and thromboembolism prophylaxis. Over the course of the program, a total of nine stimulated cycles with oocyte retrievals were performed across the five couples with SCD affected women, resulting in a total of 32 biopsied embryos (Tables 2 and 3). A conclusive diagnosis was available for 31/32 embryos and nine (29.0%) were diagnosed as genetically unaffected, for four out the five couples. Ultimately, six unaffected embryos were transferred for these four couples (five after fresh embryo transfer and one after frozen embryo transfer). The remaining three unaffected embryos were neither transferred nor vitrified.
However, none of these women achieved a pregnancy or live birth following the PGT program. Importantly, none of the women experienced VOC, ACS, or other SCD-related complications during ovarian stimulation.
PGT-M outcomes for affected menA total of three couples in the PGT program included a man affected by SCD; all were SS. Only one of the three men was receiving hydroxyurea treatment at the time of the procedure. He had cryopreserved sperm samples prior to treatment initiation which were used for fertilization due to subsequent azoospermia. The two other male partners had semen parameters compatible with ICSI, allowing the use of fresh sperm for fertilization. Across these three couples, nine stimulated cycles with oocyte retrievals were performed, resulting in 41 biopsied embryos. Of these, 13 embryos (31.7%) were genetically unaffected and transferred, either as fresh or frozen-thawed embryos and one live birth occurred (for the couple for whom cryopreserved sperm had been used) (Tables 2 and 3).
PGT-M outcomes for couples seeking for PGT for SCD and HLA typingIn the subgroup of the 17 couples seeking PGT for SCD with HLA typing, 33 ovarian stimulation cycles were initiated, and HLA-matched embryos were available in 11 cycles. Eleven fresh embryo transfers were performed in these couples, leading to 2 live births. Another live birth was achieved after a frozen embryo transfer. Overall, 3 HLA-matched births were obtained for the 17 requesting couples (17.6%). When a PGT-M cycle resulted in embryos that were healthy for SCD but not HLA-matched, the couples could choose whether or not to proceed with the transfer. As a result, a total of 11 embryo transfers were performed with embryos healthy for SCD but not HLA-matched, while 2 transfers were declined by couples due to HLA incompatibility. Thus, one couple had a healthy child but not HLA-matched.
Ovarian stimulation characteristics and outcomesA total of 123 ovarian stimulation cycles were initiated for the 60 couples included in the study. The characteristics and outcomes of these cycles are detailed in Table 4. The majority of ovarian stimulation cycles were performed using a programmed antagonist protocol pretreated with oral contraception (n = 62, 50.4%). Of the total cycles, 15 (12.2%) were canceled, with 14 due to insufficient ovarian response and one for personal reason.
Table 4 Ovarian stimulation and PGT-M outcomesAmong the 108 remaining cycles that led to oocyte retrieval, the median total gonadotropin dose was 2700 [1921–3300] IU, administered over a treatment period of 10 [9,10,11,12] days. Oocyte retrieval yielded a median of 11 [8,9,10,11,12,13,14,15,16] oocytes, 80% being mature. Embryo biopsy was successfully performed in 98 cycles (90.7%) for 54 couples, with a median of 4 [3,4,5,6,7] embryos biopsied per cycle. In 87 cycles (88.8%), at least one healthy embryo was obtained (for 52 couples). Fresh embryo transfers were performed in 73 cycles (for 45 couples) resulting in 15 live births (20.5%). Two twin pregnancies (3%) were reported, representing 12% of all live births after fresh embryo transfer.
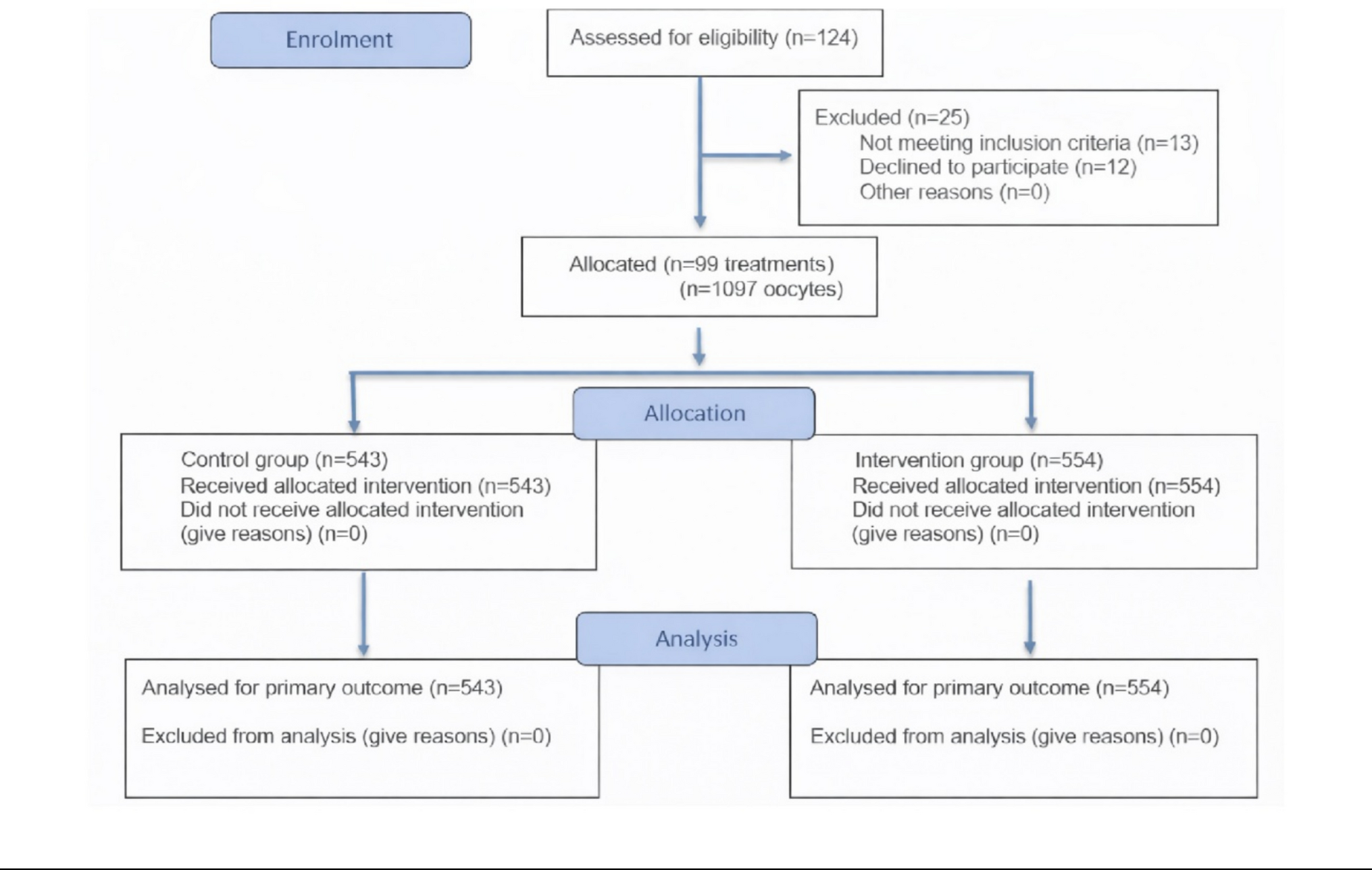
To assess the impact of sickle cell trait on ovarian stimulation response, we conducted a case–control study. Each cycle from a woman at risk of transmitting SCD was matched with two control cycles from women whose partners carried a chromosomal rearrangement. As only five women in the cohort had SCD, they were excluded to avoid bias, and the analysis was restricted to heterozygous women (sickle cell trait). In total, 99 cycles from heterozygous women were compared to 198 matched control cycles. Conditional logistic regression showed no significant differences in ovarian stimulation parameters between the two groups (Table 5).
Table 5 Comparison of the response to stimulation in heterozygous women and controls (partner of males with chromosomal rearrangement)
Comments (0)