
Remember me
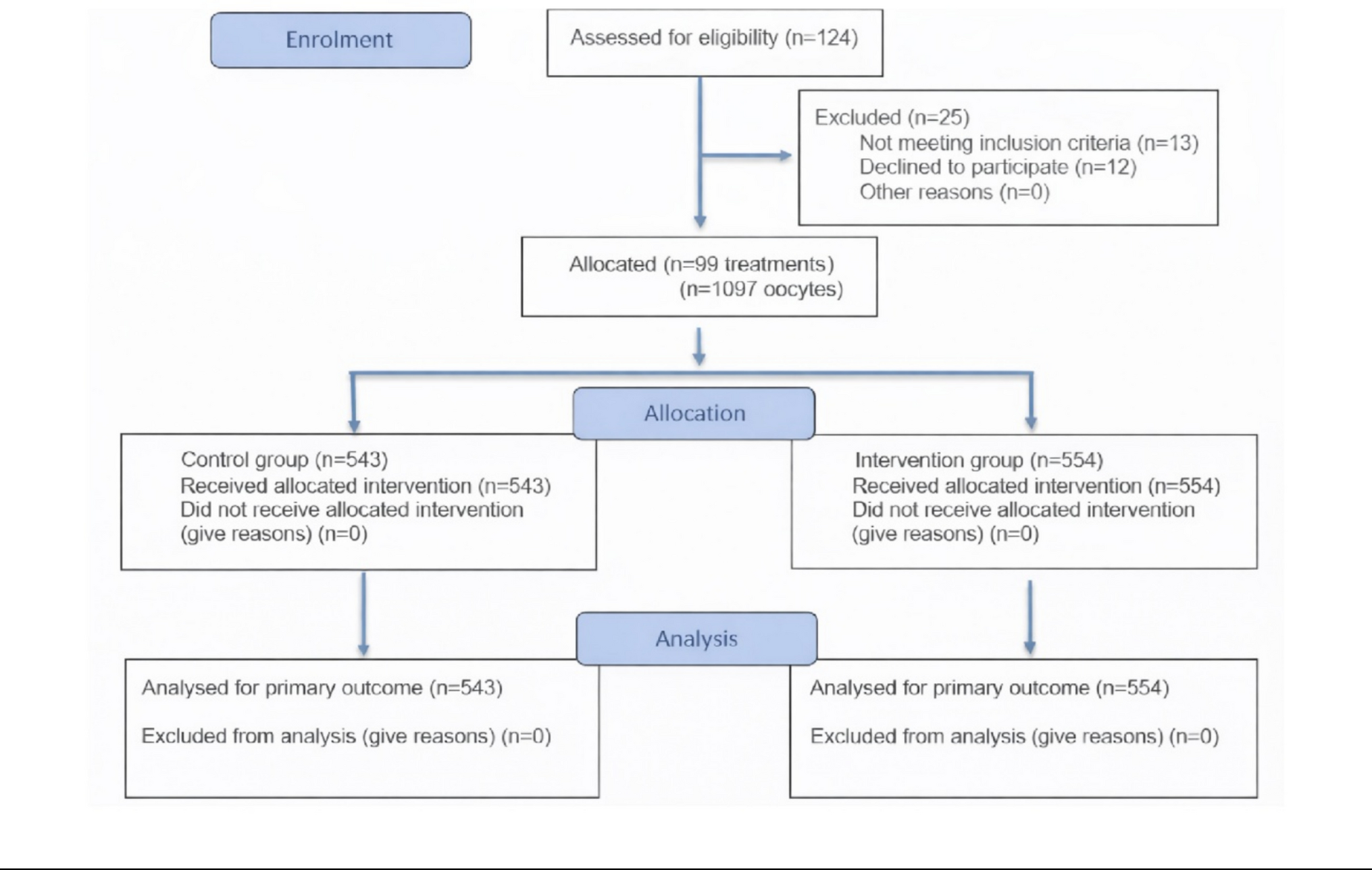

This prospective clinical trial was approved by the appropriate Ethical Committee for Drug Research and by an Internal Institutional Review Board. Eligible patients were informed about the study objectives and procedures, and those who provided signed informed consent were enrolled. No interventions deviating from standard clinical practice were performed prior to obtaining informed consent. The trial commenced in July 2022 and concluded in December 2024. This study included only patients with a medical indication for ICSI during their assisted reproduction cycle in the IVF laboratory and a BMI < 30 kg/m2. A total of 95 couples were enrolled, accounting for 99 treatment cycles and yielding 1097 mature oocytes. Of these, 543 oocytes were allocated to the control group and 554 to the intervention group. The mean age of female participants was 36.73 years in the intervention group and 36.69 years in the control group. Among male partners, the mean ages were 38.86 and 38.33 years in the intervention and control groups, respectively.
Eligibility criteria required patients to undergo ovarian stimulation using their own fresh oocytes, yielding at least six mature (MII) oocytes. Additionally, embryo development to the blastocyst stage was mandatory, and semen samples had to be obtained via ejaculation and had the ability to adjust the concentration to 10 million/mL.
Exclusion criteria included the use of vitrified oocytes, retrieval of fewer than six mature oocytes, or sperm collection through testicular biopsy or puncture and donor samples. Patients were also excluded if an insufficient number of sperm successfully traversed the cumulus barrier during the selection process or if the final sperm concentration did not reach 10 million/mL, in which case conventional ICSI was performed instead.
The distribution of infertility etiology within the study population was categorized as follows. In the intervention group, the causes of infertility were classified as unexplained (11.0%), female factor (59.9%), male factor (11.7%), and combined factors (17.3%). In the control group, the corresponding proportions were 8.8% for unexplained infertility, 61.3% for female factor, 14.2% for male factor, and 15.7% for combined etiologies. Each oocyte was assigned to a study group using simple randomization, a method that ensures an equal probability of allocation to either group. This procedure minimizes selection bias and increases the likelihood that observed differences are attributable to the interventions rather than to pre-existing characteristics. Randomization was carried out using the!RNDSEQ macro of SPSS Statistics [14], so that both groups had the same probability of being assigned at each point in time. The enrolment details are represented in Fig. 1.
Fig. 1
Flow diagram of the progress through the phases of the study showing oocyte-level allocation of sibling oocytes to the two study groups, adapted from [15]
Sample size calculation and study variablesThe primary objective of this study was to assess the proportion of embryos resulting in a good-quality day-5 blastocyst (grades A and B) according to the criteria established by the Spanish Association for the Study of Reproductive Biology (ASEBIR) [16]. For the purposes of this study, good-quality blastocysts were defined as those considered suitable for embryo transfer and/or cryopreservation in routine clinical practice. Embryos were defined as fertilized oocytes presenting two pronuclei and two polar bodies (2PN + 2CP).
For the sample size calculation, we assumed a 45% proportion of good-quality blastocysts (among evaluable blastocysts) in the control group and anticipated an increase to 55% following cumulus cell-mediated sperm selection (10% absolute increase), based on results from a previous pilot study [12]. Under these assumptions, a total of 784 embryos (392 per group) were required to achieve 80% power with a two-sided α of 0.05. The corresponding estimate of 1288 oocytes was derived from assumptions regarding oocyte maturation, fertilization rates (70%), and losses during embryo culture (15%) and should therefore be considered an approximation. Across the 99 cycles included, a total of 1387 oocytes were retrieved, of which 1097 (79.1%) reached metaphase II (MII) and were eligible for allocation. These 1097 mature oocytes were randomly allocated at the oocyte level within each cycle by simple randomization, yielding 839 fertilized oocytes (2PN + 2 PB) available for embryo developmental assessment. Secondary variables encompassed fertilization rate, blastocyst formation rate, positive pregnancy rate, and the ongoing pregnancy rate, defined as pregnancies progressing beyond 12 weeks of gestation. The pregnancy test (β-hCG level) was assessed in blood samples taken 13 days post-ICSI in fresh transfers and 9 days post transfer in cryotransfers. According to routine clinical policy, embryo transfer is performed as single blastocyst transfer (SET), and double embryo transfer is not contemplated. Accordingly, all embryo transfers included in this study were single blastocyst transfers. This policy ensured unequivocal attribution of clinical outcomes to a specific embryo and its corresponding sperm selection group.
Additional parameters such as maternal and paternal age, ovarian stimulation protocol, duration of stimulation, type of ovulation trigger, infertility etiology, and semen sample quality were also recorded. A statistical subanalysis is included to assess the impact of maternal and paternal age on these primary and secondary outcomes.
Ovarian stimulationThe controlled ovarian stimulation (COS) protocol was personalized by a fertility specialist, who selected the type, dosage, and duration of gonadotropin treatment based on each patient’s clinical profile, BMI, and ovarian reserve markers like antral follicle count and AMH levels. Protocols were adjusted according to ovarian response, and some patients used oral contraceptives in the months prior to stimulation.
Stimulation protocols vary by hormone type and cycle phase at treatment initiation. Mild protocols use lower gonadotropin doses, sometimes combined with oral agents. Final oocyte maturation was triggered with either hCG or, in antagonist protocols, a GnRH agonist to stimulate endogenous LH and FSH.
Follicular development was monitored via transvaginal ultrasound. When at least two follicles reached ≥ 18 mm, the trigger was administered. Oocyte retrieval occurred 36 h later under sedation via ultrasound-guided transvaginal aspiration.
Development and structure of the ICSI dishThe sperm selection device utilized in this study was an ICSI dish with two channels (Oosafe® ICSI Dish with Sperm Selection Channels, CE mark pending, patent publication number EP4303299, Fig. 2), a specialized tool designed to enhance sperm selection for assisted reproduction. The device used was evaluated and approved by an Ethical Committee for Drug Research and by an Institutional Review Board and is manufactured using embryo-tested materials under MD Regulation (EU) 2017/745. The product is made in ISO 13485:2016 & ISO 9001:2015 certified facility. Every batch undergoes Gamma sterilization and is tested for Mouse Embryo Assay, Endotoxin (LAL), and Human Sperm Survival and motility after manufacturing. This dish integrates two main compartments to streamline sperm selection and intracytoplasmic sperm injection (ICSI): an upper section dedicated to the ICSI procedure and a lower section consisting of two parallel lanes (Fig. 3).
Fig. 2
Oosafe® ICSI dish with sperm selection channels
Fig. 3
Dish functioning. a ICSI dish with the 3 wells (A, B, and C). b Upper lane with CCs in the B well and bottom lane without CCs, semen samples (PRE samples) are deposited in Well A. c After 1 h incubation at 37 °C, spermatozoa are collected from Well C (POST-samples)
Each lane runs longitudinally across the dish and is divided into three distinct wells, labelled A, B, and C:
Well A: Located at the right end of each lane, Well A is used for the deposition of processed semen samples prepared via density gradient centrifugation.
Well B: Positioned in the center of each lane, Well B is designed for the placement of cumulus cells freshly harvested previous oocyte denudation. In this study, cumulus cells were not included in the channel of the control group.
Well C: Found at the left end of each lane, Well C collects spermatozoa that successfully traverse the cumulus cells placed in Well B. The selected spermatozoa in Well C are considered optimal candidates for subsequent fertilization via microinjection.
A notable feature of the dish is the presence of one lane that serves as a control, devoid of cumulus cells. This control lane enables a direct comparison of sperm motility and selection in the presence versus absence of cumulus cells (Fig. 3b).
The upper compartment of the dish facilitates the ICSI process, allowing for a seamless workflow. Selected spermatozoa from Well C can be directly microinjected into oocytes within the same dish, minimizing handling and preserving sample integrity.
This precise configuration ensures a standardized and efficient sperm selection process, providing a reproducible platform for advanced assisted reproduction protocols.
Preparation of seminal sampleSemen samples were collected in sterile containers on the day of follicular puncture after a 2–3 days period of sexual abstinence, obtained through masturbation. Upon liquefaction at room temperature, each semen sample underwent analysis in a Makler chamber to evaluate sperm concentration and motility. Subsequently, all samples included in the study underwent DGC. Following completion of the gradient, sperm concentration was adjusted to 10 × 106 spermatozoa/mL.
Preparation of cumulus cellsFollowing follicular puncture, Cumulus-Oocyte Complex (COCs) were incubated at 37 °C in Global Total® for fertilization culture medium (LifeGlobal, CooperSurgical, Denmark) under low oxygen pressure until the decumulation process. COCs exhibiting normal morphology were selected for the study. A high-quality COC was defined as one presenting an expanded and loosely organized cumulus mass, indicative of appropriate oocyte maturation. Specifically, COCs displaying a compact cumulus structure or the presence of blood clots were excluded [17]. Between two and four COCs were selected per patient, depending on their size and morphological quality. Before extracting cumulus cells, the complexes were transferred to a 60-mm Petri dish filled with Global Total with HEPES® medium (LifeGlobal, CooperSurgical, Denmark) heated in an incubator at 37.0 °C for 30 min before use. Mechanical extraction of cumulus cells was performed using needles coupled to syringes, with a portion of the cumulus cells removed and stored in Global Total with HEPES® medium for subsequent dish preparation. Despite mechanical dissection, the structural and functional integrity of the cumulus cells was preserved, maintaining their extracellular matrix architecture until the moment they were penetrated by spermatozoa.
Sperm selection on the dishFirst, lanes of the dish were filled with 10 µL of the same buffer medium, Sperm Washing medium® (Irvine Scientific, Fujifilm, Japan), with which the semen sample had been processed. Next, cumulus cells were deposited, completely filling the widened central part of the lanes (Well B, only in the study group, Fig. 4) and then, 3 µL of previously adjusted to 10 mill/mL semen sample were added to the right part (Well A). On the top of the dish, microdrops of Global Total with HEPES® medium were placed for subsequent ICSI. Additionally, two drops of Polyvinylpyrrolidone (PVP) with HSA—7% (Irvine Scientific, Fujifilm, Japan) were added to facilitate the control of the ICSI pipette. Subsequently, the dish was covered with approximately 4 mL of mineral oil (Lite® Oil, LifeGlobal, CooperSurgical, Denmark) and carefully placed in an incubator for 60 min at 37 °C.
Fig. 4
Enlarged view of the lane corresponding to the study group. A Semen sample added. B Sperm is passing through the cumulus cells. C After 1 h, spermatozoa are ready for collection and subsequent microinjection
Intracytoplasmic sperm injection (ICSI)After 60 min of incubation, the oocytes were carefully placed onto the dish for ICSI. Microinjection was performed on oocytes using spermatozoa selected either by cumulus cells (allocated to the study group lane) or exclusively by DGC (allocated to the control group lane), as determined by the randomization table. Following microinjection, the oocytes were transferred to culture dishes with microwells and subsequently incubated within the Geri® time-lapse system (Genea Biomedx, Australia). Embryonic culture conditions were maintained under controlled low oxygen pressure, ensuring stable temperature and humidity levels.
Fertilization and embryo developmentFertilization was confirmed by the presence of two pronuclei and two polar bodies. Only properly fertilized oocytes were evaluated for embryo development on days 3 and 5 post ICSI. Following ICSI, embryos were cultured in a time-lapse incubation system under low oxygen and CO₂ pressure with controlled humidity, for a total duration of 5–6 days, using uninterrupted culture in Global Total® LP medium. Blastocysts were graded according to ASEBIR [16] considering blastocyst expansion, trophectoderm cell number at the equatorial plane, and the compactness of the inner cell mass. Embryo selection and categorization were conducted by senior embryologists without taking into account the experimental group allocation, ensuring unbiased evaluation.
Statistical analysisFor categorical variables, a descriptive analysis was performed using frequency and percentage. For the univariate statistical analysis of comparison between study groups, the Chi-square test or Fisher’s exact test was used.
Numerical variables were presented as number of cases, mean, and standard deviation. For the evaluation of normal distributions, the Shapiro–Wilk test was performed. if the variable had a normal distribution, the univariate analysis was performed by Student’s t-test and otherwise by the Wilcoxon rank sum test.
In addition, a stratified analysis by maternal (26–35, 36–39, and 40–45) and paternal (20–30, 31–39, and 40–53) age ranges was performed. Age was not used as a covariate in each other group as there were no significant differences in the mean age of the groups.
Values of p < 0.05 were considered statistically significant.
Statistical analysis was performed with R statistical software, version 4.4.2 and Statistical Product and Service Solutions software, version 23.0 (SPSS, Chicago, IL, USA).
Comments (0)