
Remember me
Before outlining Victoria’s specific approach, we begin this section by outlining federal efforts to control and minimize HIV transmission, which apply to all Australian states and territories. At a federal level, overarching guidelines describe a staged public health approach to managing HIV transmission, intended to establish a consistent framework among all the states and territories (Commonwealth Government 2018). These guidelines, inter alia, set out a series of principles for managing transmission, assign roles and responsibilities, and outline a management framework (Commonwealth Government 2018). Moreover, a federal HIV taskforce—comprising representatives from the government, peak bodies, researchers, advocates, medical experts, and community organizations—has been charged with identifying HIV issues and trends to help end transmission (Commonwealth Government 2023).
Despite these federal efforts, much of the day-to-day management of HIV transmission rests with individual states and territories through the application of state-level legislation, policy, and public health initiatives. While approaches vary, jurisdictions broadly adopt a dual approach, involving both public health law (and policy) and criminal law. These two mechanisms serve distinct purposes. Public health measures—both legal and non-legal—are designed to safeguard the population (rather than just individuals) by managing and controlling the spread of infectious diseases (Carter 2016). Conversely, criminal law functions to respond to severe criminal conduct and serve as a deterrent (Carter 2016). Importantly, as discussed later in this article, these two approaches do not always operate in isolation and may intersect in practice.
For the remainder of this section, we focus specifically on Victoria’s approach to regulation. We begin with historical approaches, providing necessary context and tracing the evolution of the law, before focusing on current approaches. In setting out the current framework, we do not seek to be exhaustive and have necessarily confined our discussion. We acknowledge that other areas of law—such as migration, privacy, and newly enacted affirmative consent laws—may also be relevant to the implementation of phylogenetic analysis but fall outside the ambit of this article.
Historical Approaches to Regulating HIV Transmission in VictoriaEarly approaches to managing HIV transmission in Victoria embodied HIV exceptionalism— a phenomenon that arose partly because an HIV diagnosis at the time was considered akin to a death sentence, and tight regulation was seen as necessary. Even though medical science advanced, and preventative treatment options became increasingly available, the law failed to keep pace, resulting in a form of exceptionalism whereby legislative provisions specifically targeted individuals living with HIV. In Victorian criminal law, the now repealed section 19A of the Crimes Act 1958 (Vic) made it an offence for a person to “intentionally cause[] another person to be infected with a very serious disease.” Unlike similar offences found in other Australian jurisdictions at the time, the legislative definition of “very serious disease” in Victoria applied solely to HIV (Carter 2016). Thus the Victorian offence although framed generally—couched in the terms “very serious disease”—in effect operated as an HIV-specific offence.
Section 19A was introduced in 1993 following several armed robberies where victims were threatened with syringes containing blood (Legislative Assembly, 15 April 2015, 954). It carried a harsh maximum penalty of twenty-five years’ imprisonment—harsher than other offences targeting transmission of disease or causing serious injury, both of which attracted maximum penalties of twenty years (Legislative Assembly, April 15, 2015, 954). Opposition to section 19A was widespread (Carter 2020). This opposition stemmed from concerns about stigma, its potential to disincentivize the disclosure of HIV, and the fact that the penalties were disproportionate to the harm caused (Carter 2020). After years of criticism, the provision was finally repealed in 2015. The repeal reflected recognition that the law was out of step with society’s evolving understanding of HIV risk and was motivated by a desire to reduce stigma and discrimination, and promote equality (Legislative Assembly, April 15, 2015, 954).
HIV exceptionalism was also evident in public health law. For instance, special requirements attached to HIV testing prior to their removal in 2019, with their removal described as “a major step towards driving down stigma and discrimination” (Premier of Victoria 2019). Similarly, in 2022, amendments were made to further reduce stigma and discrimination by removing explicit mention of HIVFootnote 2 in public health legislative provisions, including those relating to blood donations, tissue donations, and closure of courts and tribunals (Public Health and Wellbeing Amendment Act 2022 (Vic).
Current Approaches to Regulating HIV Transmission in VictoriaThe current approach to regulating transmission in Victoria is thought to better reflect modern scientific and societal views. While HIV is no longer deemed a death sentence and most people living with HIV are not seen as a risk to public health, it has been suggested that the behaviour of a small number of individuals may contribute to transmission and pose a public health risk (Victorian Government Department of Health 2021). Accordingly, HIV transmission continues to be subject to regulation and oversight that relies on both a public health response and criminal law, both of which are discussed below.
Public Health ResponseThe prominent regulatory response to HIV transmission adopts a public health lens, engaging the legislative and administrative powers of the state via public health officials with the intention of safeguarding population health (Carter 2016). In Victoria, the primary regulatory tools include the Public Health and Wellbeing Act 2008 (Vic) (“PHWA”) and the Victorian Guidelines for Managing HIV Transmission Risk Behaviours (2021), which are applied by the state’s Chief Health Officer (CHO).
The PHWA contains general provisions that apply to infectious diseases including HIV. Section 111 sets out guiding principles aimed at minimizing the spread of infectious diseases and identifying the shared responsibility of the state and community members. The legislation acknowledges personal responsibility—that a person who has or is suspected of having an infectious disease should take steps to eliminate or reduce transmission risk— while recognizing that others also hold responsibility for taking reasonable precautions to avoid contracting the disease.
Reflecting the administrative nature of the provisions, the PHWA grants the CHO a wide range of powers to manage and control infectious diseases, including testing and examination orders (s 113) and public health orders (s 117) that may require a person to take—or refrain from—specific actions to prevent, as far as possible, the infectious disease constituting a serious risk to public health. (Box 1 outlines the list of conditions that may be specified in public health orders.) The Act requires that, in cases where there are alternative measures available that are equally effective at minimizing a risk that a person poses to public health, the CHO chooses the measure that is least restrictive of the person’s rights (s 112). To issue an order, the CHO must believe the person has, or has been exposed to, an infectious disease and constitutes a serious risk to public health (ss 113,117). The CHO must believe that there was a reasonable attempt to provide the person with information about the effects of HIV on their health and its associated public health risk before an order is issued, unless it is impractical to do so (ss 113,117). The person subject to a public health order has a right to review the order through an internal review mechanism (via the CHO) or external review (via the Victorian Civil and Administrative Tribunal) (ss 121,122). The penalties associated with non-compliance are generally less severe and carry less social weight and stigma than those found in criminal prosecutions (Rush 2009; Scamell and Ward 2009). Nonetheless, public health measures can still be severe (e.g., detention), and, in rare cases, the criminal justice system can be engaged even when a person is being managed under a public health response.
Box 1 List of Conditions Specified in Public Health Orders (s 117)
- Participate in counselling, education, or other activities
- Undergo an assessment by a specified psychiatrist or neurologist
- Refrain from carrying out certain activities and behaviours (or only carry them out when specified conditions are met)
- Refrain from visiting a specified place (or class of place)
- Reside at a specified place of residence at all times or during specified times
- Notify change of name or place of residence
- Submit to the supervision of a nominated person (e.g., by attending meetings, receiving visits, or providing information)
- Receive specified prophylaxis
- Undergo specified pharmacological treatment
- Submit to being detained or isolated (or both).
HIV-specific guidelines issued by the Victorian Government work in concert with the PHWA. These guidelines provide content to the legislative provisions and operationalize the law by setting out a framework for managing the behaviours of people living with HIV. Like the PHWA, the guidelines seek to strike the right balance between mitigating the risk of HIV to the community and protecting the rights of individuals. Accordingly, the guidelines are only applied when there is a perceived risk to the public and do not apply in cases where a person has taken reasonable steps to minimize transmission. While the guidelines do not offer an exhaustive list of what would constitute reasonable steps, they do provide some examples. These include having a sustained undetectable viral load (less than 200 copies/mL), consistent condom use with lubricant, consistent disclosure of HIV status to sexual partners, and seeking confirmation from sexual partners that they are taking PrEP before engaging in sex (Victorian Government Department of Health 2021).
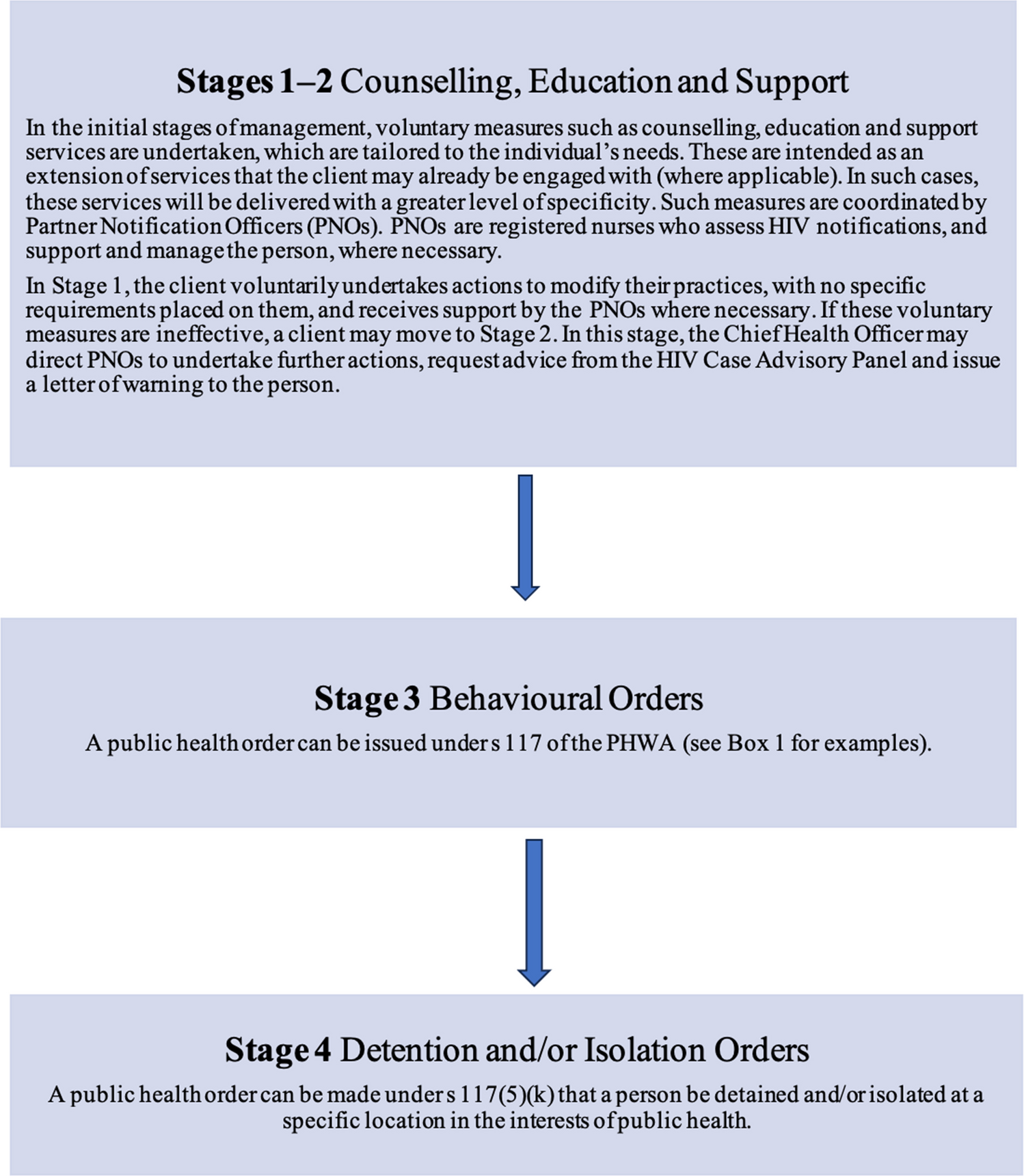
The framework employs a four-stage approach (see figure 1 for an overview), establishing a hierarchy of measures (non-legislative and legislative) to manage HIV transmission. In most cases, the framework operates primarily through escalation, employing less coercive measures aimed at modifying behaviours (e.g., education, counselling, and support) in the first instance, followed by more coercive practices (public health orders, including behavioural, detention, and/or isolation orders). These more coercive measures are intended to be reserved for exceptional cases where less coercive measures have been exhausted or deemed ineffective. However, it is also recognized that measures may be applied in a non-sequential order in exceptional cases (or when required) (Victorian Government Department of Health 2021, 20).
Figure 1
Four-Stage Approach to HIV Management (The figure was created by the authors, drawing on Victoria’s Guidelines for Managing HIV Transmission Risk Behaviours (Victorian Government Department of Health 2021).)
While the public health and criminal law approaches serve distinct functions, they do not operate in isolation. In exceptional cases, where a person fails to comply with public health orders, or where risky HIV transmission practices are continued with clear intent to cause harm—or with serious disregard for the wellbeing of others—a referral to police may occur (Victorian Government Department of Health 2021, 26).
Criminal LawWhile Victoria’s approach to regulating the transmission of HIV is predominately public health based, criminal law continues to play a regulatory role beyond cases of non-compliance with public health orders. Although HIV-specific offences no longer exist, general criminal provisions may still apply. The use of general criminal law rather than HIV-specific offences receives qualified endorsement by various United Nations bodies, alongside strong caution that criminal law should only be employed in exceptional circumstances where there is actual and intentional transmission of HIV (UNAIDS Reference Group on HIV and Human Rights, 2023).
While there are potentially a range of criminal offences that may apply to HIV transmission, in practice, the offences relied on fall into two broad categories. These are assault offences, which depend on HIV transmission having occurred, and endangerment offences, which apply to potential rather than actual transmission. Table 1 provides an overview of relevant Victorian criminal provisions that may be (and, in some cases, have been) applied in the context of HIV.
Table 1 General Criminal OffencesLike the more coercive measures of the public health response, engagement with the criminal justice system is intended to occur only in exceptional cases and as a measure of last resort, consistent with the federal and state guidelines previously discussed (Commonwealth Government 2018; Victorian Government Department of Health 2021). In this sense, criminal law can be characterized as a “mop up strategy” used when public health interventions have been ineffective (Rush 2009). However, as will be further discussed below, concerns have been raised that criminal law is being applied outside of these circumstances and engaged independently of the public health response.
To secure a conviction, the prosecution must establish criminal responsibility. To prove intention or recklessness, the requisite mental element must be established—the person must have known that they have HIV (Woodroffe 2009). This contrasts with the public health response, which recognizes that preventing transmission is a shared responsibility and that every individual, irrespective of their HIV status, has a responsibility to engage in safer sex practices to reduce transmission, including by maintaining a low viral load (in the case of a person living with HIV) or taking preventive measures (in the case of a person not living with HIV) (Woodroffe 2009). Instead, criminal laws inadvertently punish those who are aware of their HIV-positive status, even though this cohort is much less likely to transmit HIV (Hall et al. 2012). Such an approach may encourage HIV status ignorance (strategic or otherwise) and may serve as a deterrent to testing.
Comments (0)