Study characteristics and patient demographics
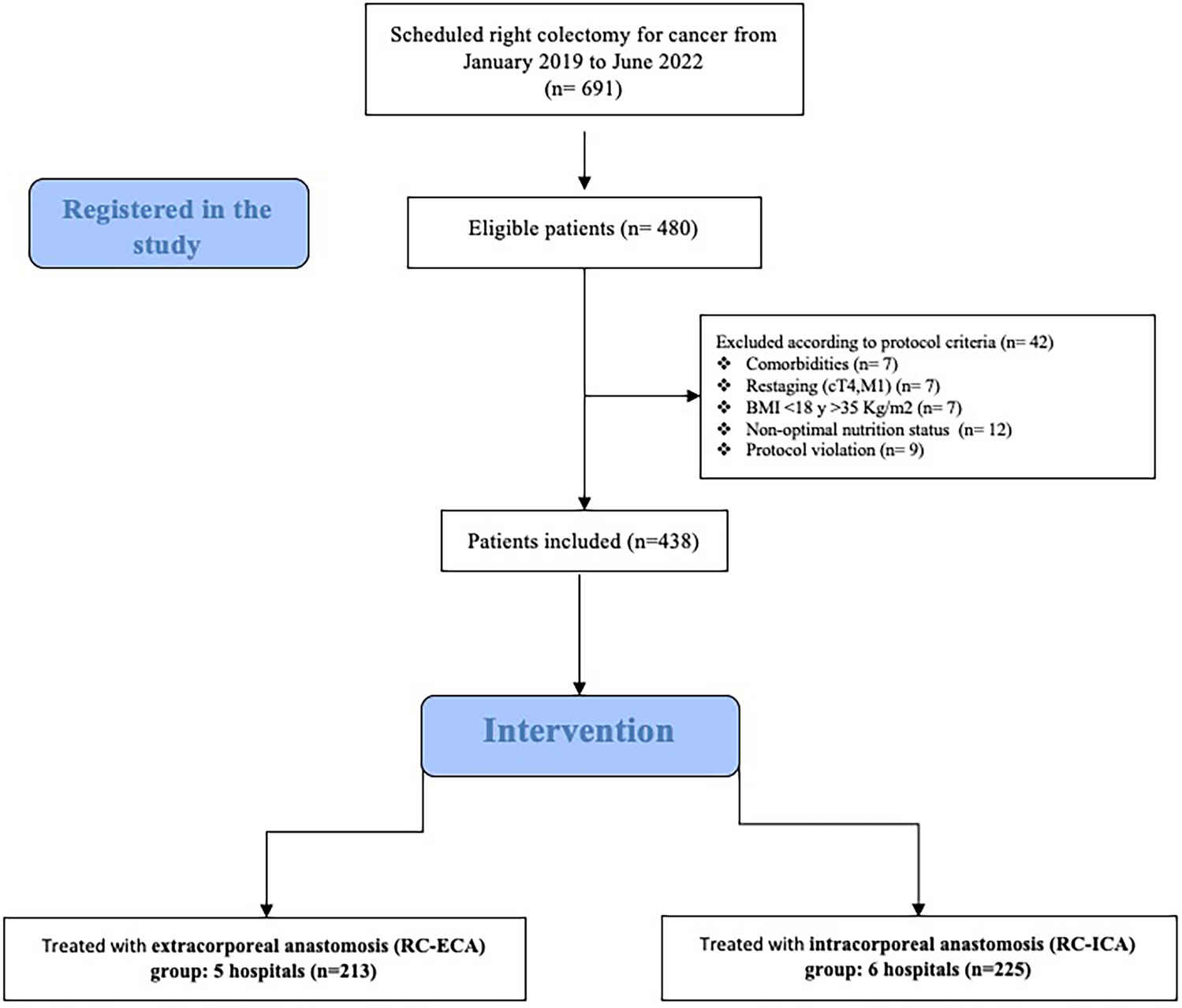
The initial search yielded 404 records, of which 16 studies met the inclusion criteria following de-duplication and screening (Fig. 1). The majority of studies were retrospective in design (81.3%, n = 13) [10,11,12,13,14,15,16,17,18,19,20, 23, 25] and conducted in the United States (56.3%, n = 9). [10,11,12,13,14,15,16, 21, 22] First authors predominantly (93.8%, n = 15) had established publication history in robotic surgery [10,11,12,13,14,15,16, 21, 22, 24, 25]. Sample sizes within robotic cohorts ranged from 6 to 109 patients (median = 31; IQR = 46).
Of the included 16 studies, CD was listed as an indication in 12 papers [10, 12,13,14,15,16,17,18, 22,23,24,25], UC in 8 papers [13, 16, 19,20,21, 24, 25]. Four studies [16, 21, 24, 25] included mixed IBD cohorts, where both CD and UC were listed as indications. Robotic ileocolic resection (robotic ICR) was the most performed procedure (50%, n = 8) [10,11,12,13,14,15]. Comparator arms included laparoscopic surgery (31.3%, n = 5) [16, 19, 20, 22, 23], open surgery (6.3%, n = 1) [10], while 62.5% (n = 10) were single-arm studies [11,12,13,14,15, 17, 18, 21, 24, 25]. All studies reported age and sex. Pooled mean patient age was 41.15 years (SD = 7.82), mean body mass index (BMI) was 23.62 kg/m² (SD = 2.07; reported in 14 studies) [10,11,12,13, 15,16,17,18,19,20,21, 24, 25], and males constituted 49.5% (SD = 19.5%) of cohorts. Prior abdominal surgery was reported in half (n = 8)11–16,19,20, though details were inconsistently documented. Only one study (6.3%) reported on surgeon training, noting that cases were performed during the surgeons’ robotic learning curve [20]. Risk of bias assessment indicated 14 studies at low risk and 2 at moderate risk, common limitations included short follow-up (≤ 30 days) and inadequate baseline matching.
Surgical setup
The da Vinci platform was predominantly used (93.75%); one employed the Medtronic Hugo system (6.25%) [25]. Preoperative planning was described in five studies (31.3%) [16, 20, 21, 23, 24], with platform selection driven primarily by robotic availability in 12.5% (n = 2) [16, 20]. Preoperative imaging guided surgical planning in three studies (18.8%) [21, 23, 24].
For colectomy and ICR, patient positioning was reported in 25% (n = 4), [11, 21, 23, 24] the most common being modified lithotomy (n = 2) [19, 23], left lateral decubitus (n = 1) [21], and Trendelenburg (n = 1) [11]. Robotic docking strategies were specified in 18.8% (n = 3) [22,23,24] all utilising left-sided approaches. Double-docking was employed in 12.5% (n = 2) [23,

Comments (0)