Study population
The GECKO Drenthe birth cohort is a Dutch population-based cohort comprising around 3000 children born between April 2006 and April 2007. It is set up to study the determinants and development of children’s diet and childhood overweight and obesity. The design and methodology of the GECKO Drenthe birth cohort have been described elsewhere [27]. In short, all pregnant women in Drenthe with an expected delivery date between April 2006 and April 2007 were invited to participate in this study by their midwives, general practitioners, or gynecologists. After informed consent was obtained, these women were included during the third trimester of their pregnancy or within 6 months after delivery. The GECKO Drenthe birth cohort was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the University Medical Centre Groningen, the Netherlands (Medical ethical approval ID: 2005.260). Informed consent of participation was given by parents or guardians. The cohort is registered at www.birthcohorts.net (ID: 138).
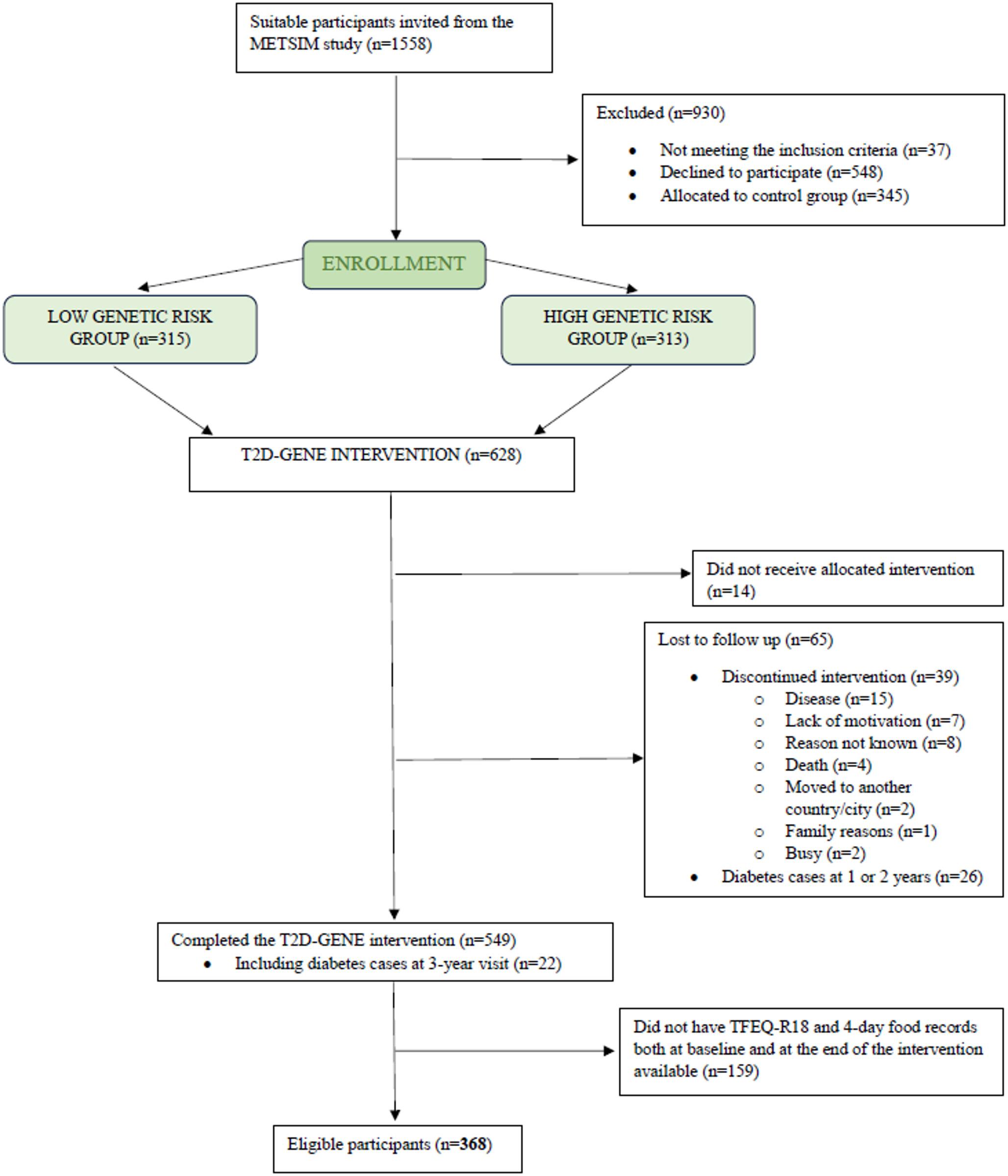
Out of 2684 children with valid dietary data (after correcting decimal default errors due to computer processing), 2552 were included in the study to monitor food intake; these children had more than two food intake assessments between 7 months and 3 years of age. Of these, 856 had dietary data at ages 10/11 years and were included in the analysis examining food intake and diet quality in middle childhood (see supplementary Fig. S1 for a flow chart). The number of children included in the dietary intake pattern analyses varied across food groups due to differences in the age at which specific foods were typically assessed (e.g., fruits and vegetables from 7 months, bread from 14 months, etc.). As a result, sample sizes varied by food group (supplementary Fig. S1).
Data collectionAnthropometric measurements
The weight and height of the children were measured during routine health examinations conducted by trained staff of the Youth Health Care centers (YHC) at ages 3 and 10/11 years. Body weight was assessed using an electronic scale and rounded to the nearest 0.1 kg. Height was measured in the standing position against a wall and rounded to the nearest 0.1 cm.
Dietary data
We assessed the diets after the introduction of solid foods, which in the Netherlands is between 4 and 6 months of age. A total of 8 visits were conducted throughout the study; at the age of 7, 9, 11, 14, 18, and 24 months, 3 and 10/11 years. At ages 3 and 10/11 years, a validated food frequency questionnaire (FFQ) comprising 71 food items, specifically designed for Dutch children, was filled out by their parents [28]. Seven response categories ranging from ‘not used’ to ‘6–7 days a week’ were applied to assess the frequency of food consumption. Portion sizes were assessed with fixed unit portion sizes (e.g. slices of bread) or common household measurements (e.g. cups and spoons). Data were processed with the help of standardized portion sizes to calculate the total intake of each food item in grams per day. Subsequently, daily energy and nutrient intakes were calculated using the Dutch Food Composition Database 2011 [29]. For each food item, energy intake was calculated by multiplying the estimated daily intake (g/day) by its corresponding energy value (kcal per 100 g), and the total daily energy intake was obtained by summing the energy contributions of all food items. From the FFQ, data were extracted on the consumption of specific food groups, including fruit, vegetable, bread, dairy, meat and fish, convenience meals (including pizza, pancakes, and patat—French fries in Dutch—this group of foods indicates typical convenience meals for Dutch children), savory snacks, sweet snacks, and sugar-sweetened beverages (SSB).
Possible under or overreporting with the FFQ was excluded by the use of the Goldberg cutoff method, based on the ratio of the reported energy intake and the basal metabolic rate [30], calculated with the Schofield equation [31]. As a result, 58 children with an energy intake/baseline metabolic rate ratio below 0.87 (n = 55) or above 2.75 (n = 3). Moreover, 4 children with incomplete FFQ data were excluded from the final analysis.
In the younger ages, 7, 9, 11, 14, 18, and 24 months, the consumption of specific food groups was evaluated using a series of self-administered food intake questionnaires; questioning age-appropriate foods. These questionnaires contained questions about 1) the type and amount of fruit and vegetable (from 7 months onward), 2) the main type of bread consumed: white, brown (made from a mixture of refined flour and whole meal flour), or wholegrain (from 14 months onward),3) the amount of dairy (from 14 months onward), 4) the amount of meat and fish (from 18 months onward), 5)the frequency of convenience meals (from 18 months onward), savory snacks (from 18 months onward), sweet snacks (from 14 months onward), and SSB (from 18 months onward). More detailed information about these food intake questionnaires is presented in supplementary Fig. S2 and Table S1.
Development of dietary intake temporal patterns
The information reported in the food intake questionnaires from 7 months to 3 years was used to track the trends of diet across several food groups: fruit, vegetable, bread type (white, brown, wholegrain), dairy, and a combined ‘meat and fish’ category (due to meat and fish being assessed together in a single question and the relatively low consumption of fish at this age [32]), as well as convenience meals, savory snacks, sweet snacks, and SSB. For fruit and vegetable, jarred and fresh forms were analyzed separately, reflecting common Dutch practices of initiating complementary feeding with ready-to-eat jarred products. Dietary intake temporal patterns were established separately for each food groups. For bread, patterns were defined by the predominant type consumed, whereas for other food groups, patterns were based on food intake level (g/day), categorized as low, medium, or high. The cut-offs for each food group are presented in supplementary Table S2. The cut-offs were divided according to frequency and relevance. Taking fruit, for example, one jar of fruit is equivalent to 194 g and one piece of fresh fruit is equivalent to 120 g. To standardize one portion of fresh and jarred fruit within the same food group, we classified fruit consumption into three categories: < 100 g as low, 101–200 g as medium, and > 200 g as high.
Diet quality indices
Based on the dietary data obtained with the FFQ at age 10/11 years, three different types of diet quality indices were calculated: the lifelines diet score (LLDS), the dietary approaches to stopping hypertension (DASH) score, and the Mediterranean diet score (MDS), all representing a different dimension of diet quality.
The LLDS, developed based on international evidence on diet-disease relationships outlined in the 2015 Dutch Dietary Guidelines, serves as a reliable indicator of Dutch dietary habits [33]. Methods for calculating this diet score have previously been developed and described [33]. LLDS includes eight health-positive food groups (vegetable, fruit, whole grain products, legumes and nuts, fish, oils and soft margarine, unsweetened dairy, and tea), and three health-negative food groups (red and processed meat, butter and hard margarine, and SSB). Daily consumption in g/1000 kcal of each food group is divided into quintiles, scored on a scale of 0–4 (reverse for health-negative food groups), and summed, with higher scores indicating better diet quality.
The DASH diet is specifically designed to maintain healthy blood pressure [34]. Recent research involving a sample of 425 Iranian children aged 6 to 18 years [35] and 1570 Canadian children with a mean age of 12.4 years [36] suggests that adherence to the DASH diet may play a substantial role in the prevention of overweight in children. To calculate the DASH diet score, five food groups (vegetable, fruit, whole grain products, legumes, and nuts; and low-fat dairy) with positive health effects, and three food groups (sodium, red and processed meat, and SSB) with negative health effects were identified. All intakes were adjusted for energy. Each food group is divided into quintiles based on intake, scoring 0–4 (the opposite for negative groups) and summed, with higher scores indicating a better diet quality. The details to calculate this diet score have been previously described [37].
The MDS assesses adherence to the traditional Mediterranean diet, which has demonstrated protective effects on the incidence of cardiovascular diseases [38]. Studies have shown that compliance with the Mediterranean diet is associated with the prevention and control of childhood obesity in the pediatric population [39]. In the MDS, fruit, nuts, vegetable, legumes, grains, potatoes, and fish are classified as beneficial components of the Mediterranean diet, while meat and dairy products are classified as detrimental components. All intakes were adjusted for energy. A score of 0 or 1 point is assigned according to the median intake of beneficial or detrimental components, respectively. Except for fish intake, children who did not consume fish are assigned a value of 0 and those who did are assigned a value of 1. Fat intake is scored based on the ratio of monounsaturated to saturated lipids. The final MDS score ranged from 0 to 9 points, with a higher score indicating better diet quality. The details of this score have previously been described [40].
Family characteristics
During the pregnancy period, comprehensive demographic and family characteristics were collected through a detailed questionnaire completed by both parents. Furthermore, data were supplemented by midwives, gynecologists, and clinical records. The variables used for this analysis included maternal and paternal education level, age at birth of the child, occupational status, smoking habits during pregnancy, pre-pregnancy height and weight, household income, and the presence of siblings at birth. Maternal and paternal characteristics were analyzed separately. Education levels were divided into three categories: low (no education, primary school, lower vocational or lower general secondary education), middle (intermediate vocational training or higher secondary education), and high (higher vocational or university education). Parental age at birth of the child was categorized into four groups: 16–25 years, 26–30 years, 31–35 years, and 36 years and older. Occupational status was dichotomized as employed (employed, or self-employed) or unemployed (unemployed, student, domestic tasks, inactive, or other receiving benefits or pension). Pre-pregnancy weight status was classified according to Body Mass Index (BMI) as follows: not overweight (BMI < 25 kg/m2), overweight (25 ≤ BMI < 30 kg/m2), and obesity (BMI ≥ 30 kg/m2). Smoking behavior during pregnancy and the presence of siblings were dichotomized as: yes or no. Household income in this study was defined by the “Equivalized Household Income Indicator (EHII),” a standardized, cross-cohort comparable income indicator developed by Pizzi et al. that provides a direct measure of material resources [41]. Based on tertiles of estimated household income, income levels were categorized into three groups: low (< €1752/month), middle (€1752–2216/month), and high (> €2216/month).
Statistical analysis
To describe the temporal patterns of dietary intake of the different food groups, LCA was applied to the food intake levels from 7 months to 3 years of age to identify unique patterns. We evaluated latent class models with 2 to 5 classes to determine the optimal number of classes. The optimal number of classes was determined by evaluating the fit, interpretability, parsimony, and stability/identification of the model. The model fit indices, including the Akaike information criterion (AIC) values, the Bayesian information criterion (BIC) values, and the entropy. The analysis relied on a variety of fit criteria, of which the BIC has been shown in simulations to perform particularly well in selecting the ‘correct’ latent class model [42]. Each child was assigned to the class corresponding to their highest posterior probability. Classification uncertainty inherent to probabilistic assignment was acknowledged.
To explore if the dietary intake temporal patterns of healthy or unhealthy food groups in early childhood predict food intake in middle childhood, we employed chi-square tests for categorical variables, non-parametric Kruskal–Wallis test and Mann–Whitney U test for continuous variables with a skewed distribution. Next, linear regression analysis was conducted to examine the association between dietary intake temporal patterns and diet quality, measured by the LLDS, the DASH score, and the MDS. In this analysis, potential child-related confounders (child’s sex and age) were added to the model. To determine to what extent family characteristics explained the association between dietary intake temporal patterns and later diet quality, maternal education level, maternal smoking during pregnancy, and the presence of siblings at birth were included in the model. 17 children with missing data for at least one covariate were excluded from the analysis.
To evaluate how SES and family characteristics are related to children’s dietary intake temporal patterns, multinominal logistic regression analysis was employed to explore the associations between socioeconomic and parental factors and dietary intake temporal patterns in early childhood. A backward stepwise approach was used to select significant factors. Variables were chosen based on existing literature [43,44,45] as anticipated predictors of dietary intake temporal patterns or exposures, including parental education level, occupational status, weight status, smoking status during pregnancy, age at birth, household income, and the presence of siblings at birth. Due to the high correlation between maternal and paternal characteristics, these factors were analyzed separately to investigate their contributions to dietary intake temporal patterns.
For a sensitivity analysis, linear regression analysis was repeated using recalculated diet quality scores that excluded the component corresponding to the food groups of interest. This applied to fruit, vegetable, dairy, meat and fish, and SSB, as these were the food groups included as components of the diet quality score. For example, when examining associations between temporal patterns of fruit intake and overall diet quality, the fruit component was omitted from the score. This approach allowed us to investigate the independent contribution of specific dietary intake temporal patterns to overall diet quality, while minimizing potential inflation from the intake of the group under investigation.
Children with missing values in multiple covariates were excluded from the regression analysis. Assumptions for regression analysis were verified and collinearity between variables was assessed. Data analysis was performed with IBM SPSS Statistics version 28 and R version 4.4.1. Statistical significance was set at p < 0.05.

Comments (0)