As hypothesized, during the 3-year lifestyle intervention in aging prediabetic men, cognitive restraint (CR) scores increased, while uncontrolled eating (UE) and emotional eating (EE) scores decreased, even though the T2D-GENE intervention did not specifically target changes in eating behavior traits. Additionally, favorable changes were noted in the intake of various food groups, while the total energy intake did not change. Importantly, we found that changes in eating behavior traits were associated with dietary changes.
Our findings align with previous lifestyle interventions for individuals with or at risk for T2D, which have reported increased cognitive restraint and reduced overeating behaviors [31, 33, 34, 53], although they included smaller, mixed-sex samples and some even targeted eating behaviors [31, 53]. However, compared to other interventions utilizing the TFEQ-R18, the changes in eating behavior traits observed in our study were modest [53,54,55], possibly due to differences in study design, such as a specific emphasis on modifying eating behavior traits [53, 54], and population characteristics [53,54,55]. Our study involved a larger sample of older men, who typically exhibit higher CR scores and lower overeating tendencies, namely UE and EE, than younger individuals [25, 29, 56, 57], and baseline scores in our cohort reflected this pattern [53,54,55]. In our study, CR may have increased because of dietary counselling or an awareness of participating in an intervention. Future research should explore whether targeting eating behavior traits in interventions leads to greater changes in eating behavior traits in older men.
As total energy intake remained unchanged, the observed shifts in food consumption suggest a qualitative improvement rather than only caloric restriction. The dietary changes were sustained throughout the 3-year period, indicating a stable shift in dietary behavior. Particularly the changes in the increased intake of fiber-rich foods and improved quality of dietary fat can be considered beneficial for people at risk of T2D, due to their positive effect on improving insulin sensitivity [52, 58]. Our findings among older men are in line with previous lifestyle interventions among middle-aged men and women with prediabetes or T2D [35, 36]. Changes in eating behavior traits seem to have a role in dietary changes among older men, regardless of BMI. In previous interventions, the increase in CR has been associated with improvement of the diet quality such as increased intake of fruit [31] and decreased energy intake [30] and fat, especially saturated fat [32] among men and women. Interestingly, the increase in CR was inversely associated with whole-grain product intake, despite an overall rise in whole-grain consumption during the intervention. This unexpected finding may reflect the nature of CR, which involves limiting food intake to manage body weight [19]. Although whole-grain products were encouraged, heightened CR may have led to a general reduction in food intake, including healthy options. As whole-grain bread is typically preferred by middle-aged and older Finnish men, and intake in our study aligned with population norms [14], the inverse association may indicate a broader decline in bread consumption. This reduction could be explained by more regular meal patterns or the replacement of bread-based snacks with fruits or vegetables, both emphasized during the intervention.
UE shares similarities with external eating (i.e. eating in response to the presence of food) as measured by the Dutch Eating Behavior Questionnaire [59]. Previously, a decrease in external eating was associated with decreased intakes of energy and fat among men and women [32] whereas in our study, the decrease in UE was associated with decreased intake of pastries and chocolate, – foods high in fat and energy. UE is derived from the original Three-Factor Eating Questionnaire traits disinhibition (i.e. lack of restraint of eating in response to negative feelings or the presence of palatable food) and susceptibility to hunger (i.e. susceptibility to feelings of hunger) [60]. Both UE and the related traits have been associated with higher intake of energy-dense foods in cross-sectional studies among men and women [23, 25, 28, 41, 49, 61], also supporting our findings. However, a longitudinal study observed that decreases of disinhibition and hunger were associated with increased intake of vegetables among men and women [31]. In conclusion, promoting the reduction in UE may benefit dietary improvements, and could help prevent T2D among older men. A reduction in UE may reflect improved regulation of reward-driven eating behavior. Given its association with reward sensitivity [62] and hedonic responses to palatable foods [63], lowered UE could indicate diminished reliance on highly palatable, nutrient-poor foods for pleasure, thereby enhancing dietary quality. While the absolute changes in intake associated with decreased UE were modest, they consistently targeted energy-dense foods high in saturated fat and sugar, suggesting a qualitative improvement in dietary choices that may have cumulative benefits for metabolic health over time.
EE has similarly been associated with increased consumption of hyperpalatable foods in cross-sectional studies [22, 25, 40,41,42, 61]. However, in our study, the decrease in EE was associated with an increased intake of vegetables, fruit, and berries and weakly with a reduced intake of fatty cheeses. This inverse relationship to the consumption of healthy foods, such as vegetables, is less commonly observed [64] making the results unexpected. Emotional eaters tend to regulate their emotions by excessive consumption of hyperpalatable foods, rich in fat and sugar, that provide an immediate reward and reduce the effect of stress [65]. The regular intake of hyperpalatable foods seems to gradually displace the consumption of health-promoting foods, such as vegetables and fruit [66], potentially explaining our findings. Our findings suggest that reducing EE may support better diet quality, but confirmation requires further research. To the best of our knowledge, no prior longitudinal studies have reported significant associations between changes in EE and diet.
Both UE and EE are associated with impulsive and emotion-driven eating, where food choices are often automatic or motivated by comfort-seeking [67, 68]. Thus, reductions in these traits may enable more conscious and deliberate food decisions, supporting healthier dietary patterns. We cannot confirm the effect of the intervention due to the absence of control group data, but during the additional meetings targeted at participants with higher BMI, topics such as mindful eating, flexible restraint, and identifying triggers for overeating, were emphasized. These strategies may have contributed to the observed changes by enhancing inhibitory control and promoting more intentional food choices. These findings support the potential of targeting impulsive eating traits in dietary interventions aimed at preventing T2D.
Our study adds to the limited body of research on eating behavior traits among aging men, an underrepresented population in this field. To our knowledge, no previous longitudinal studies have focused exclusively on men. As women typically score higher on measures of CR, UE, and EE compared to men [37,38,39] and given that the associations between eating behavior traits and dietary outcomes may differ by sex [21, 22], it is plausible that similar changes in eating behavior traits could have resulted in greater or qualitatively different dietary changes among women. Some cross-sectional studies have suggested that the associations between EE and sweet energy-dense foods may be stronger in women compared to men [23, 42], which could help explain the lack of such associations in our study. This may be attributed to sex differences in food preferences. A previous study indicated that EE is the main driver for snacking behavior at workplace, but among women it is more strongly reflected in the consumption of sweet energy-dense snacks [69]. Additionally, it has been found that women tend to prefer sweet comfort foods whereas men prefer more savory and meal-type foods, for example, pizza or pasta [70]. Furthermore, some cross-sectional studies have reported associations between EE and non-sweet energy-dense foods exclusively among men [25, 42]. Our results may provide some support for this, since the change in EE was directly, but weakly, associated with the change in the intake of fatty cheeses, which may be classified as non-sweet energy-dense foods, or at least, common ingredients in high-fat meals. Understanding the possible sex-specific aspects of eating behavior traits is crucial for more personalized prevention or treatment of non-communicable diseases such as T2D.
Strengths and limitations
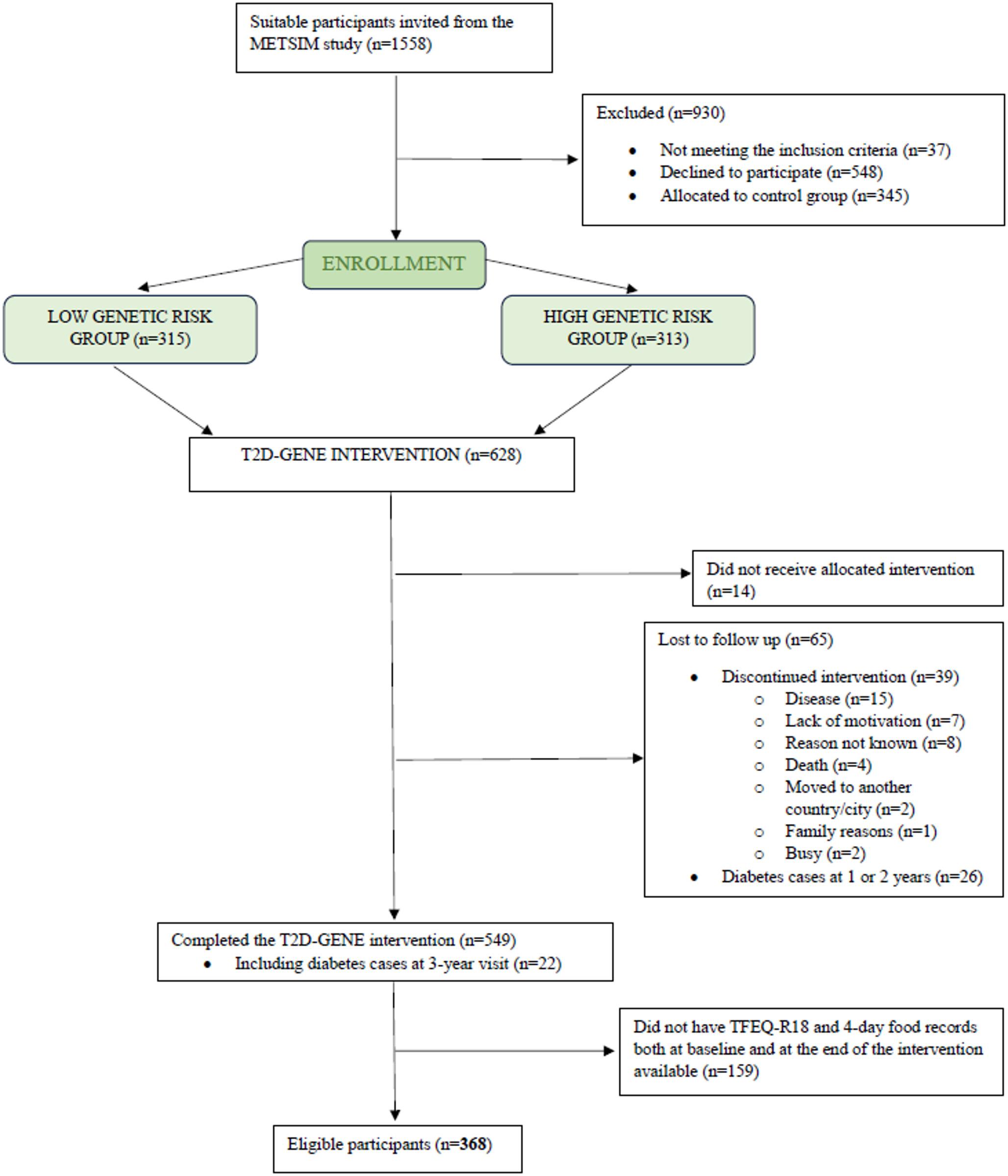
Our participants were aging prediabetic men with overweight or obesity, and thus the results might not be generalizable to all. However, individuals similar to our participants are those who need new effective ways to prevent T2D. Aging men are rare in an eating behavior study, and thus the results are novel. The number of participants stayed high although the food records and/or the TFEQ-R18 (from baseline and at three years) were not returned by all participants. Thus, this paper may lack statistical power to detect all possible changes and relationships. The absence of TFEQ-R18 and dietary data in the control group limits causal inference and prevents definitive attribution of observed changes to the intervention. However, this does not affect the validity of the observed associations between changes in eating behavior traits and dietary intake within the intervention group. These associations provide insight into how psychological factors may relate to dietary changes and help identify potential targets for future interventions.
The participants were likely more motivated to make dietary changes than the general population, as they were volunteers recently being made aware of their prediabetic status. Consequently, similar changes may be more difficult to achieve and maintain in less health-conscious or more diverse populations. This should be considered when interpreting the generalizability of the findings.
Previous studies on the associations between eating behavior traits and diet are mainly cross-sectional. We used a 3-year longitudinal analysis, providing more insight into causality than cross-sectional studies. In studies with a higher number of participants, food frequency questionnaires are more commonly used to assess the habitual food intake. We used 4-day food records that provide more accurate information of the actual food intake. Food records that include a weekend day and are kept for at least three days are commonly considered to represent the usual food intake [71]. Furthermore, the strength of food records is that they do not rely on participants’ memory. However, the amounts of foods might not be perfectly accurate because they are reported by the participants. We tried to increase accuracy with clear instructions before filling out the food records and checking them upon return with the participant. Another limitation is that the participants may change their usual eating habits or underreport due to the recording. However, this is more common among women and people with obesity [73,73,74].
Different eating behavior questionnaires are not entirely comparable even though they intend to assess the same phenomena. TFEQ-R18 has been validated among many populations [19, 22, 48] and it was developed to make it quicker and easier to measure eating behaviors [19]. Longer questionnaires, such as the original TFEQ with 51 items, might be too extensive for the participants to read or answer all questions accurately [60].

Comments (0)