
Remember me
This study was based on data from the Danish Diet, Cancer, and Health cohort (DCH). The DCH cohort has been described in detail elsewhere (18). Overall, 160,725 individuals were invited to participate if they lived in Copenhagen or Aarhus County, if they were between 50–64 years, and if they were not diagnosed with cancer registered in the Danish Cancer Registry (19). The initial data collection took place in 1993–1997 and resulted in a cohort of 57,053 participants. Participants completed questionnaires on diet and lifestyle, which were optically scanned at the study centre to check for errors and missing information. The self-administered questionnaire was developed specifically for the DCH cohort (19). Anthropometric and other biological measurements from participants were gathered at two study centres (19).
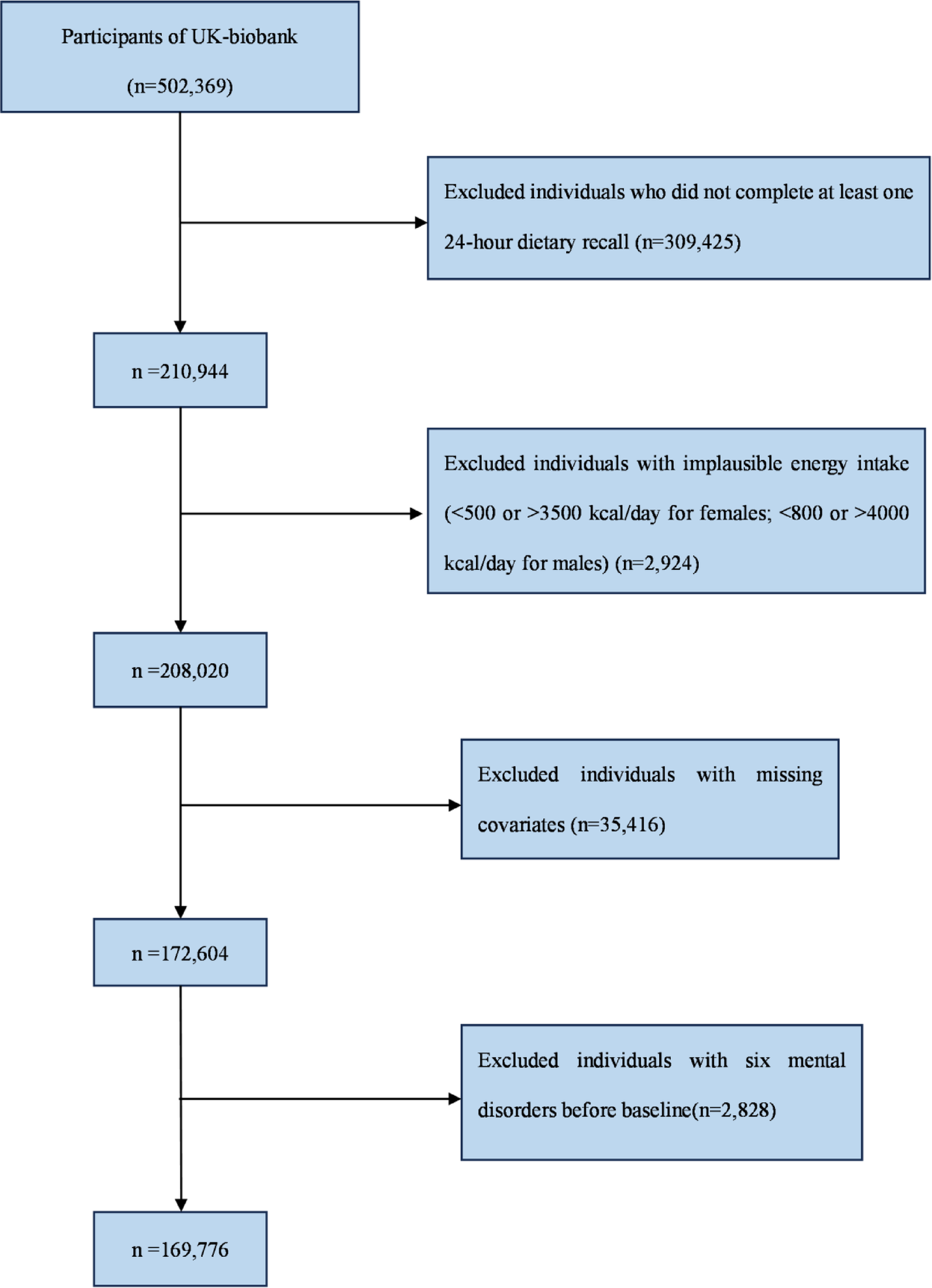
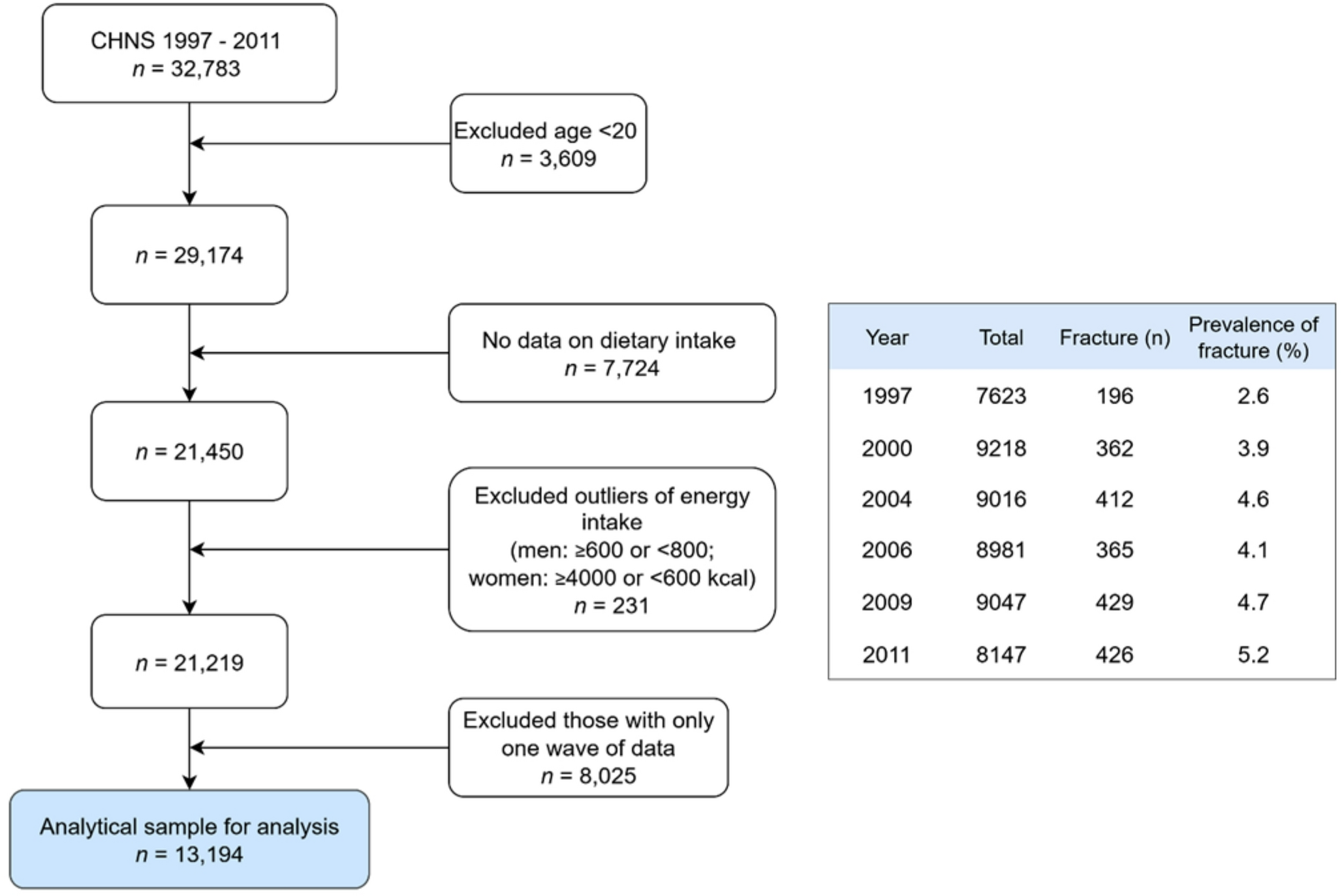
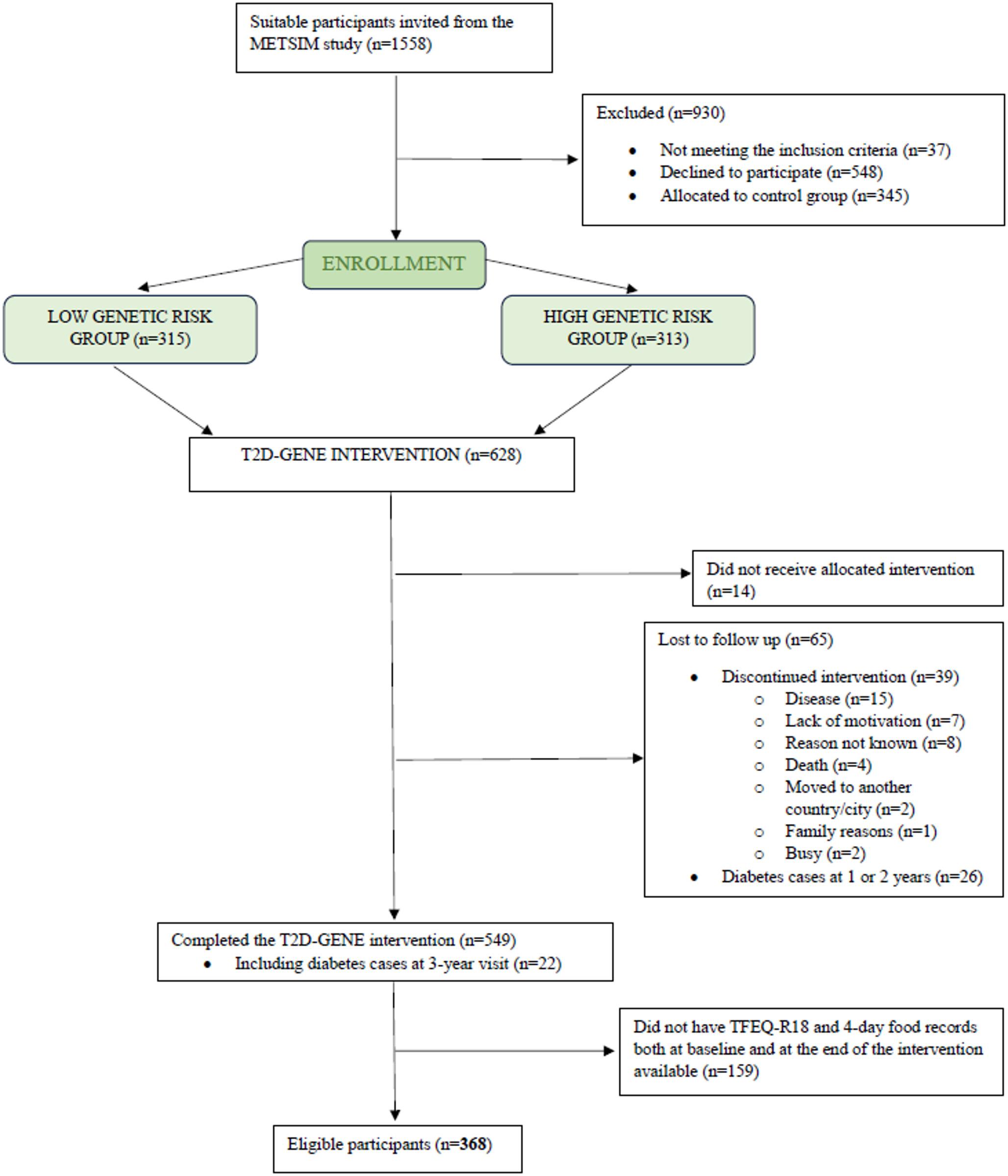
Participants with incomplete or missing data on diet, background information, and potential confounders were excluded in the present study (Fig. 1).
Fig. 1
Flow chart of the study population from the danish, diet, cancer, and health study eligible for statistical analysis in the present study. Participants included had no prior diagnosis of cancer at baseline and provided complete information on all covariates
In secondary analyses, the association between adherence to the EAT-Lancet diet and CRC in participants with diabetes at baseline was examined. Diabetes at baseline was defined if self-reported in the lifestyle questionnaire at baseline. The participants could answer ‘yes’, ‘no’, and ‘do not know’ if they had diabetes. Participants who answered that they did not know if they had diabetes and participants who answered that they did not have diabetes were treated as a separate group.
EAT-Lancet diet indexInformation on diet was collected at baseline with a food frequency questionnaire (FFQ), which was sent by letter. The FFQ gathered information on participants’ food and beverage intake over the past 12 months and contained 192 items in 12 categories ranging from never to more than eight times a day (19). The questionnaire was checked by interviewers and intake of specific foods and nutrients was calculated by the software program FoodCalc, which used specifically developed standardised recipes and portions sizes (18). The FFQ has been validated for assessment of food, energy, and nutrient intake and was compared with two seven-day diaries, where the subjects were instructed to describe all food items in as much detail as possible, and the food was weighed (19).
Adherence to the EAT-Lancet diet was based on participants’ average intake from the FFQ. The diet score used in this study was developed by Stubbendorff et al. (20). It consists of 14 components and points were given between 0–3 for each component in relation to the level of adherence. A score of 0 was given for intakes far from the recommended levels, while 1 and 2 represented partial adherence. A score of 3 was given when intake was within or above (for beneficial components) or below (for limited components) the recommended range. The components consist of whole grains, potatoes, vegetables, fruits, dairy, beef and lamb, pork, chicken, eggs, fish, legumes, nuts, unsaturated oils, and added sugar (Supplementary Table 1). It is possible to score between 0–42 points, where 0 is lowest adherence and 42 is highest adherence. The diet index was based on the EAT-Lancet reference diet (14).
Colorectal cancerThe outcome was diagnosis of CRC during the follow-up period, analysed both as a combined outcome and divided into CC and RC. Information on cancer diagnoses from the DCH study was obtained through register linkage to the Danish Cancer Registry using the unique personal identification number assigned to every Danish citizen at birth. Cancer was defined using International Classification of Diseases 10 codes: C18 (colon cancer), C19 (cancer in the rectosigmoid junction) and C20 (rectal cancer) (21, 22).
CovariatesInformation on potential confounders was collected via the self-administered lifestyle questionnaire at baseline and the FFQ. Potential confounders selected a priori based on previous literature and related to the EAT-Lancet diet and CRC were: age, sex, BMI, smoking status, physical activity level, alcohol consumption, education level, diabetes, energy intake, hypercholesterolemia and hypertension. Smoking status was categorised as ‘Never smoked’, ‘former smoker', ‘smoker 1–14 g tobacco/day’, ‘smoker 15–24 g tobacco/day’ and ‘smoker ≥ 25 g tobacco/day’. Physical activity level was dichotomised into less than 30 min of physical activity daily and at least 30 min of physical activity daily, based on recommendation from the Danish National Board of Health for adults (23). Education level was assessed in four categories: ‘vocational education (e.g., hairdresser or plumber), ‘short education’ (e.g., only primary school, high school or one or more short courses), ‘medium education’ (e.g., social worker or BSc degree) and ‘long education (e.g., MSc or higher degree from university). Information on alcohol and energy intake was assessed through the FFQ. Participants could answer ‘yes’, ‘no’, and ‘do not know’ to whether they had a history of hypertension and/or a history of hypercholesterolaemia. Participant height and weight were collected during the baseline visit to a study center by trained professionals. Height was measured to the nearest 0.5 cm without shoes, and body weight was measured with a digital scale, and recorded to the nearest 100 g, with the participant wearing light underwear. BMI was calculated as weight divided by height squared (kg/m^2) (19).
Statistical analysisDescriptive statistics for baseline characteristics were presented for all participants and across groups of adherences to the EAT-Lancet diet. Cox proportional hazards models, with age as the underlying timescale, were used to calculate hazard ratios (HR) with 95% confidence intervals (95% CI) for the development of CRC. Participants were considered at risk of developing cancer from their age at recruitment until age at diagnosis with CRC, loss to follow-up, change in personal identification number, emigration, death of other causes than CRC, or administrative censoring on December 31st, 2016, whichever came first.
The EAT-Lancet diet score was analysed as a categorical variable in five groups by dividing the distribution of EAT-Lancet diet score in the study population into approximate quintiles to ensure a balanced number of participants in each category (≤ 16 points, 17–19 points, 20–21 points, 22–23 points, and ≥ 24 points). It was also analysed as a restricted cubic spline variable, with knots automatically placed at percentiles dividing the distribution into four equal parts (16, 19, 21, and 25 points). The group of participants with the lowest diet index score was the reference group for the categorical analyses, while the reference for the cubic spline analysis was set at 10 points. The analysis was performed in four models. Model 1a was adjusted for age and sex and as strata-variables tertiles of enrolment date; Model 1b was further adjusted for diabetes, smoking status, physical activity level, alcohol consumption, history of hypercholesterolemia, history of hypertension and educational level; Model 2 was further adjusted for BMI and Model 3 was further adjusted for energy intake. Both overall incidence of CRC and subtypes, CC and RC were investigated. In the analysis of CC, participants who developed RC were censored at the time of their RC diagnosis, as only the first CRC diagnosis was considered. Similarly, in the analysis of RC, participants who developed CC were censored at the time of their CC diagnosis. The proportional hazards assumption was checked with a log-minus-log survival curve. The assumptions of independence between entry time and the outcome were checked and satisfied when stratifying entry dates into tertiles.
We analysed data on the additive scale using the pseudo-observational method with death as a competing event and calendar time as the time scale. The assumptions of independent entry time and censoring were checked and satisfied when we stratified pseudo-values into four separate strata based on quartiles of dates of enrolment as in a previous study (24). Because the pseudo-observations estimate the individual event status at a specified time point with no censoring, several time points were chosen in the analyses, including 5, 10, 15, and 20 years to investigate the patterns in associations over time. In the second step, we ran a generalised linear model of the pseudo-observations using the identity link function to estimate risk differences (RDs). Age was adjusted for in the models using a restricted cubic spline variable with five knots and additional confounders were included in model 2.
Because people with diabetes have a higher risk of developing CRC compared to healthy individuals, analyses were stratified according to diabetes status at baseline in a continuous analysis. Additionally, a categorical and continuous analysis was made on the entire study population, stratified by sex. All stratified analyses were supplemented with a test for interaction using a Z-test for the interaction term with the EAT-Lancet diet.
As a robustness check, we conducted a sensitivity analysis in which the EAT-Lancet diet was categorized into quartiles, ensuring approximately equal numbers of participants in each group. Hazard ratios for quartiles were estimated using the same Cox proportional Hazards models as in the main analysis. In another sensitivity analyses, we examined the risk of bias due to potential reverse causation by excluding the first 4 years of follow-up time. Additionally, a sensitivity analysis was performed to examine whether the estimates changed when including participants who answered ‘do not know’ if they have diabetes, in the analysis for participants with diabetes. The statistical significance was based on a two-sided P-value < 0.05. Programming was performed using Stata version 17.0.
Comments (0)