According to the 2022 WHO and International Clinical Consensus (ICC) classifications, the diagnosis of BP in CML occurs when there are more than 20% blasts in peripheral blood and/or bone marrow cytology or extramedullary tumors with blast proliferation. However, there is a discrepancy among the classifications regarding the number of detectable lymphoblasts. In the ICC, the criterion for lymphoid BP is the presence of > 5% of morphologically apparent lymphoblasts, while in the WHO classification, it is characterized by the presence of increased lymphoblasts in peripheral blood or bone marrow, with no optimal cutoff [2, 5, 6].
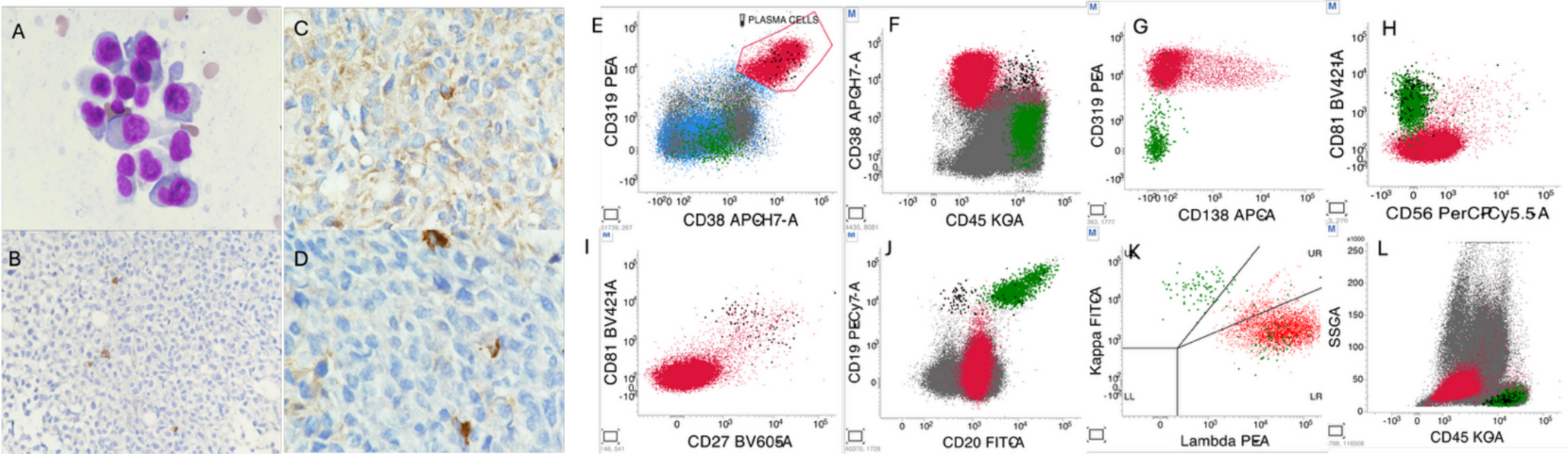
Although the clinical relevance of very low percentages of lymphoblasts remains a matter of debate, accumulating evidence indicates that even minimal populations of aberrant lymphoblasts detected by flow cytometry may carry significant prognostic implications [7]. In a large cohort of newly diagnosed patients with chronic-phase chronic myeloid leukemia, Jiang et al. demonstrated that a flow cytometry–based aberrant lymphoblast (ALB) cutoff of 0.4%, determined by X-tile analysis, effectively stratified patients according to the risk of progression to lymphoid blast phase. Patients with ALB ≥ 0.4% exhibited a markedly increased cumulative incidence of lymphoid transformation, whereas those without detectable ALB showed excellent transformation-free survival. Notably, lymphoid transformation occurred early during tyrosine kinase inhibitor (TKI) therapy and was not observed below this threshold [7].
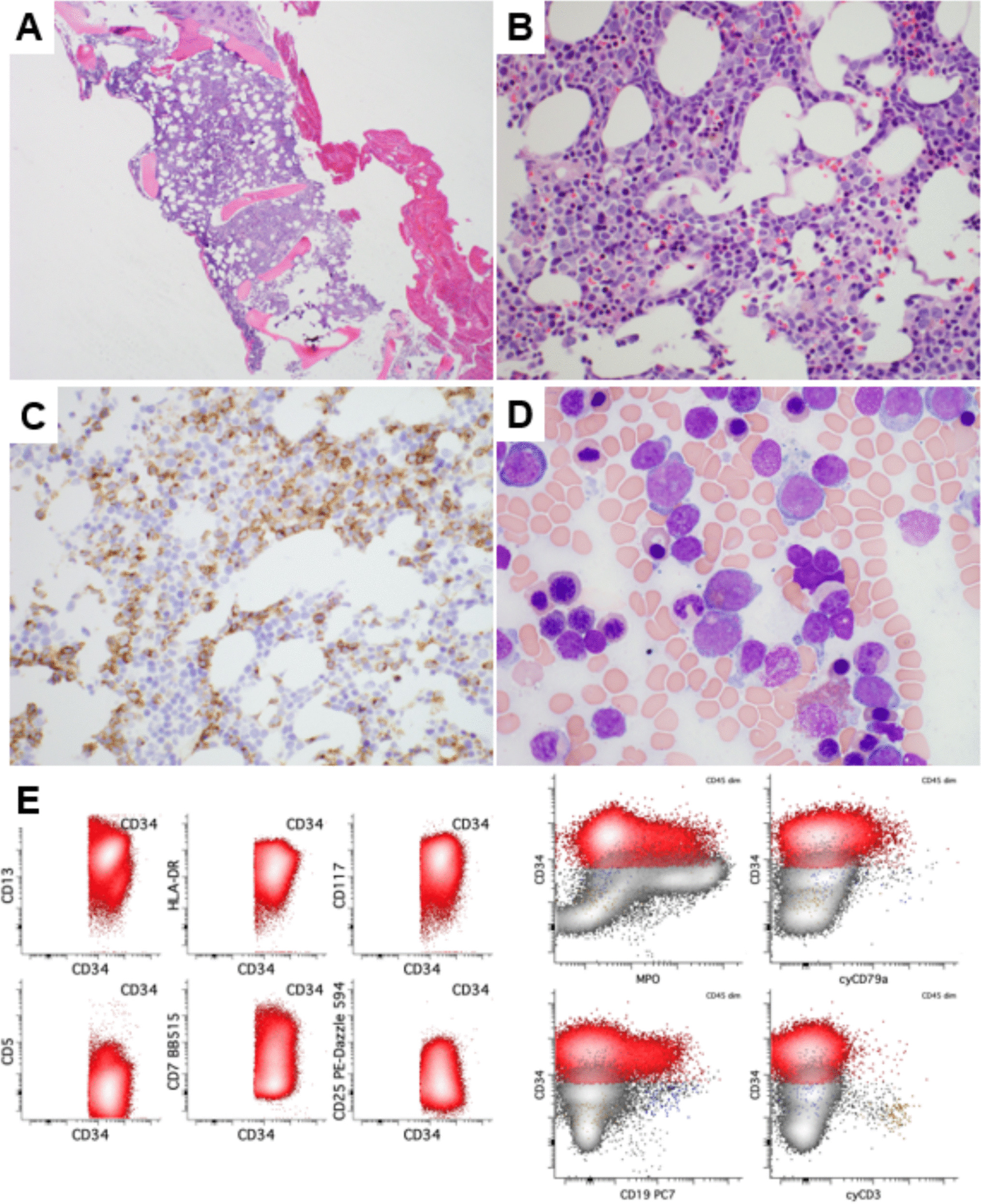
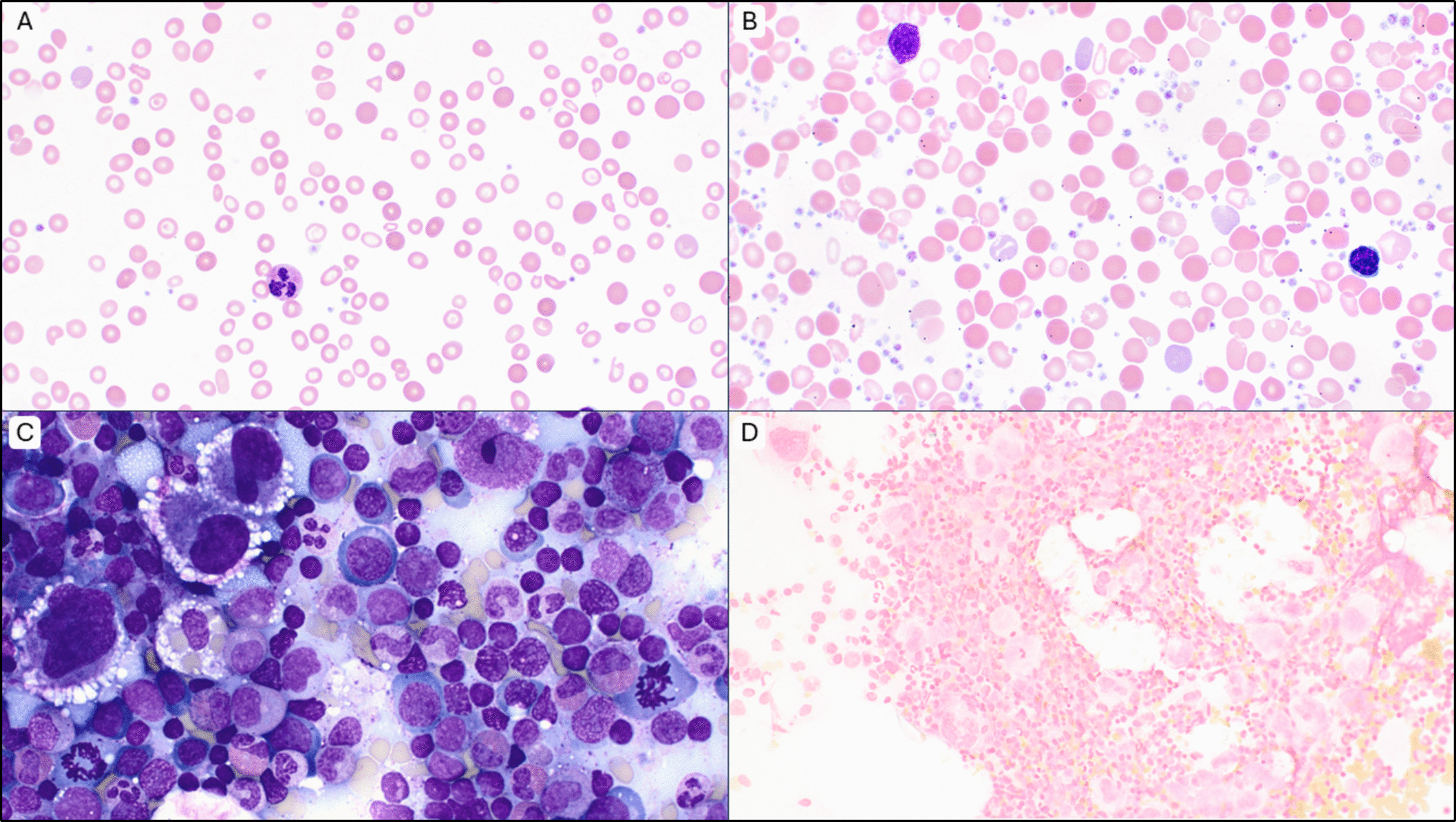
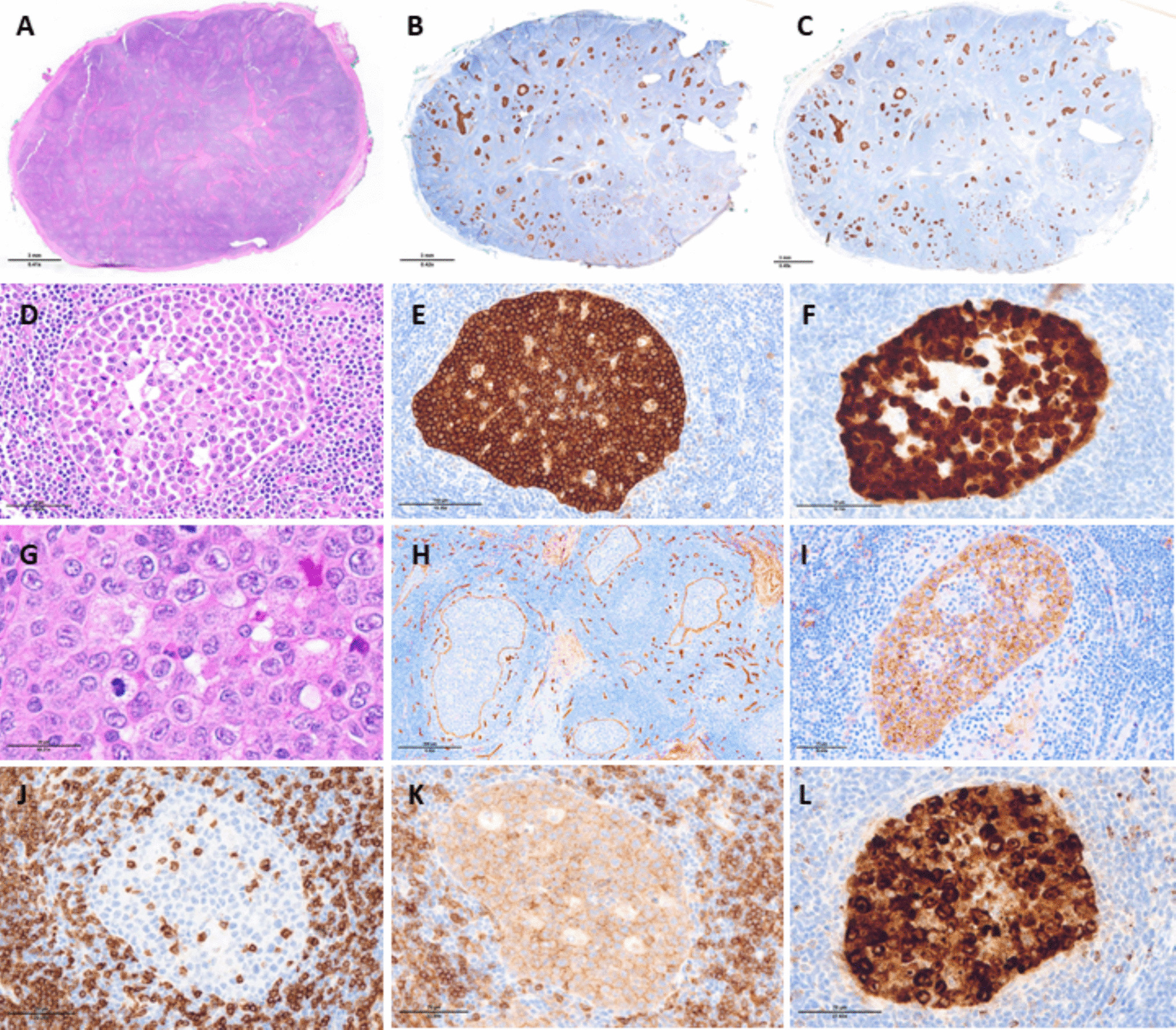
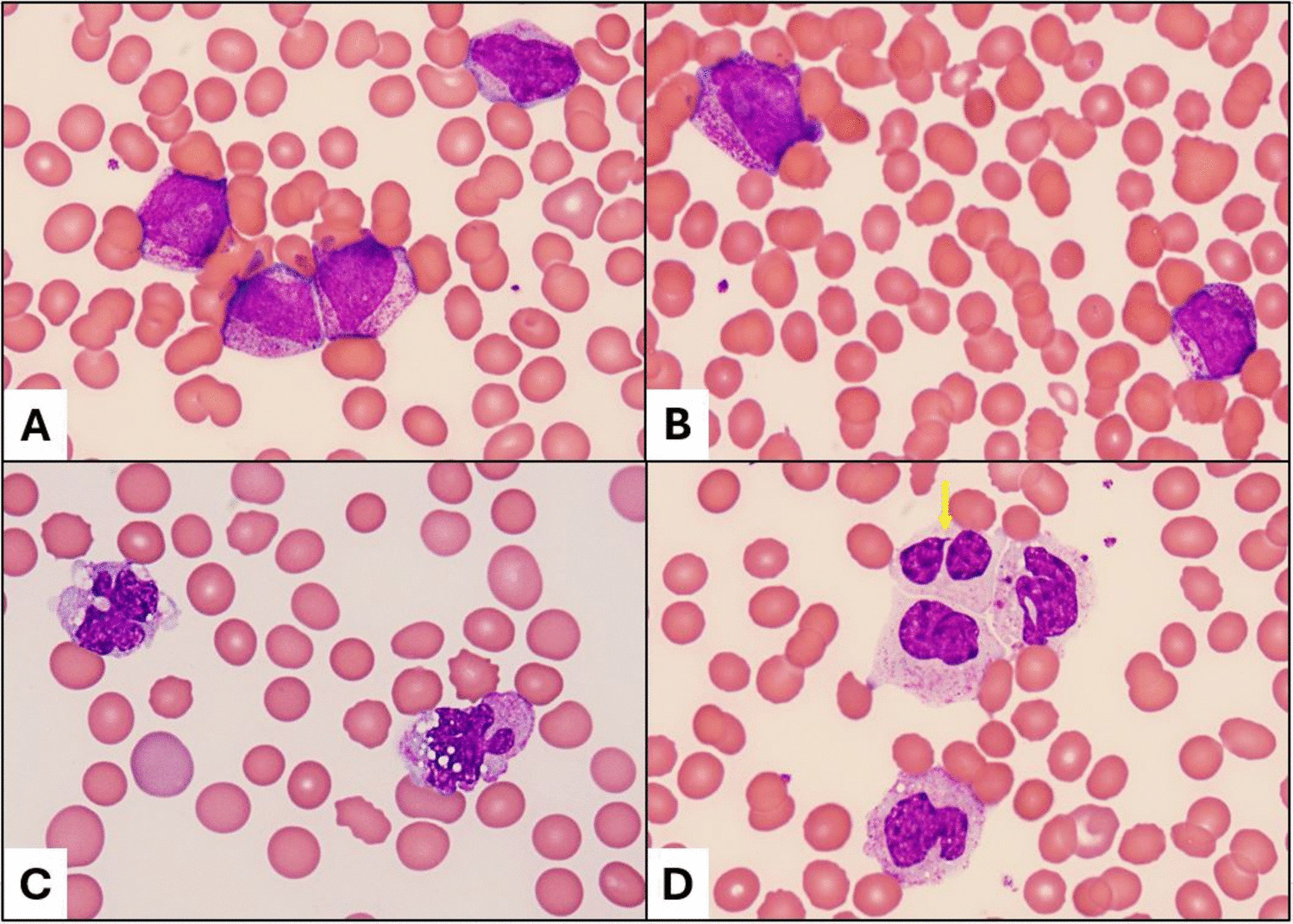
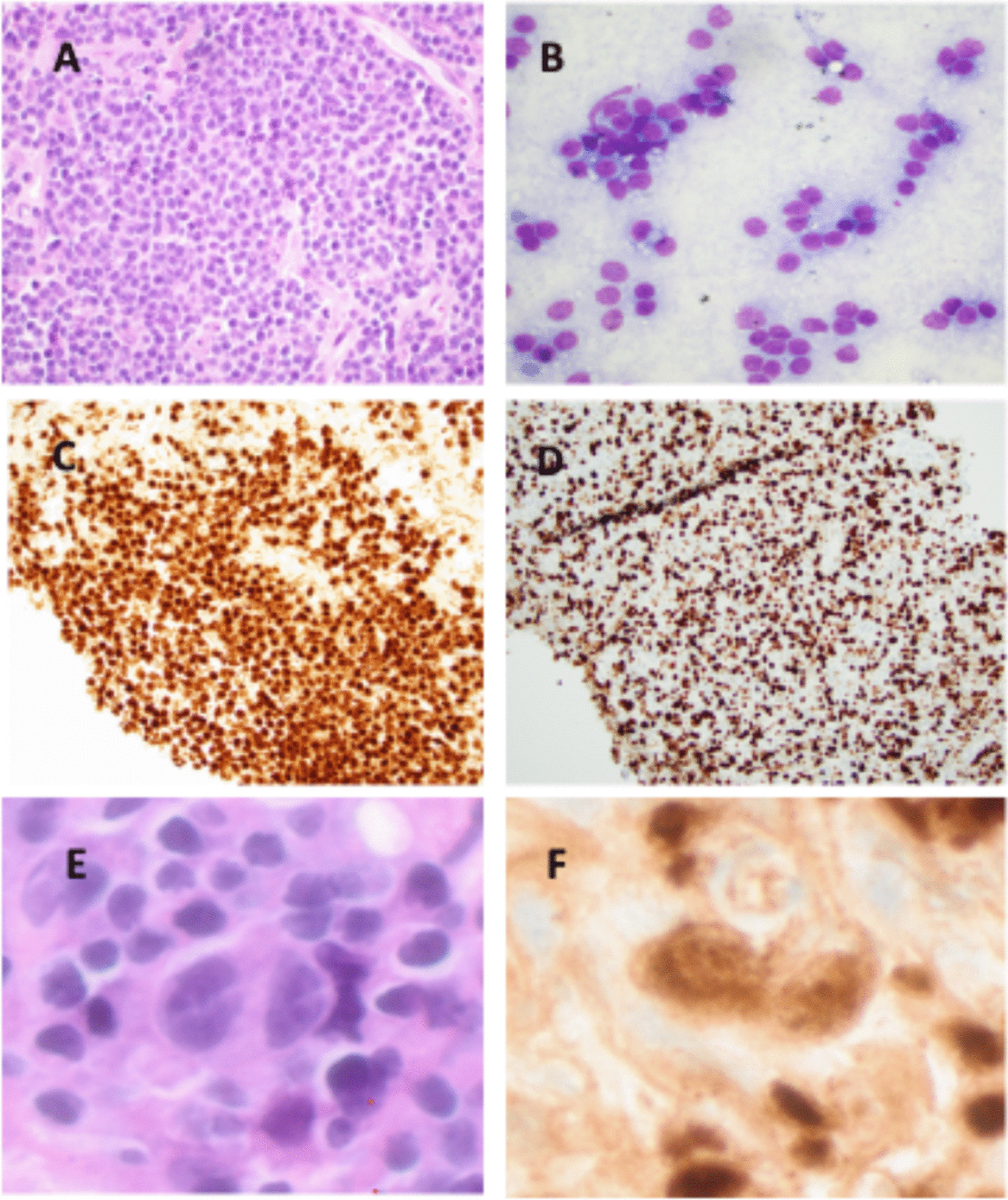
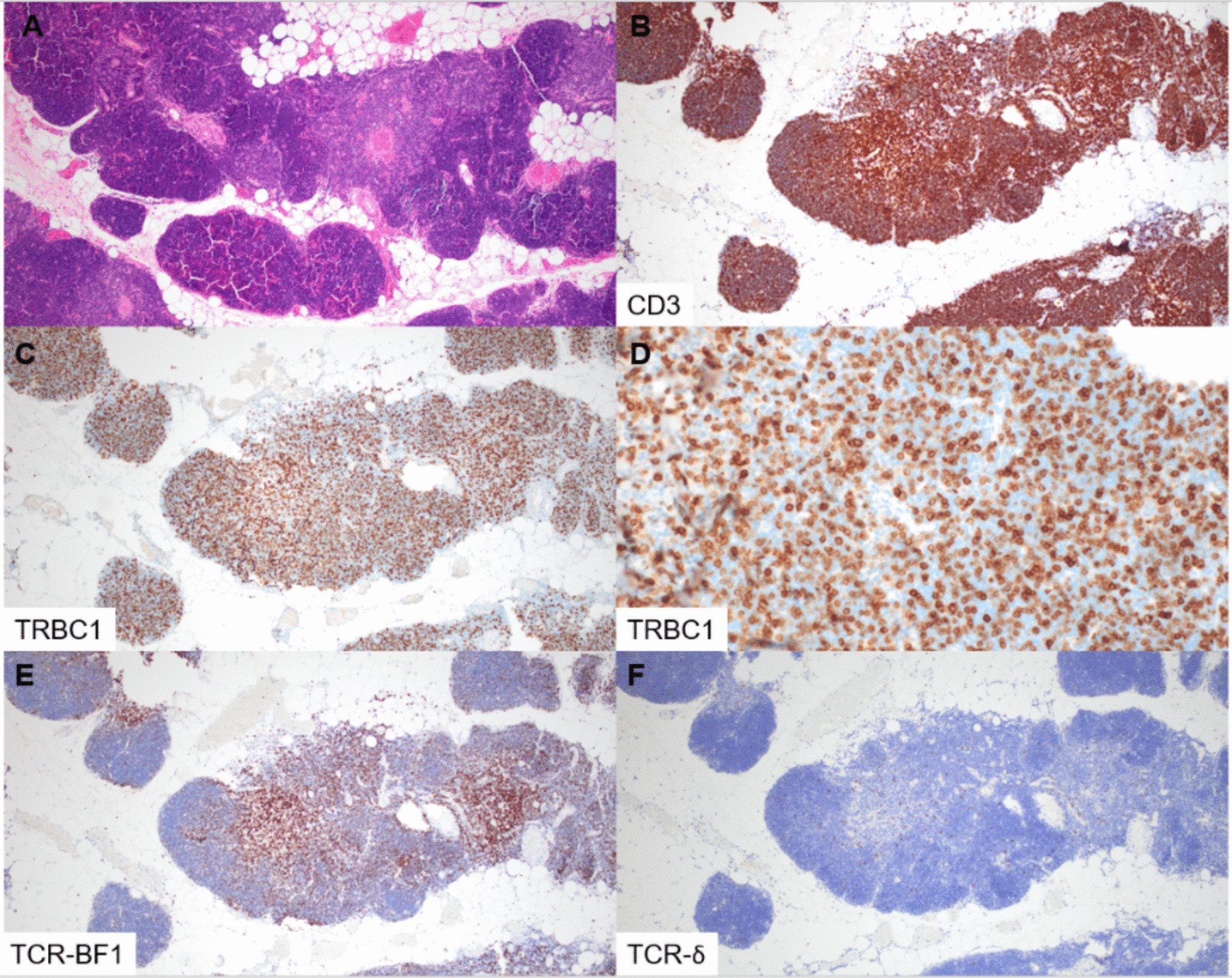
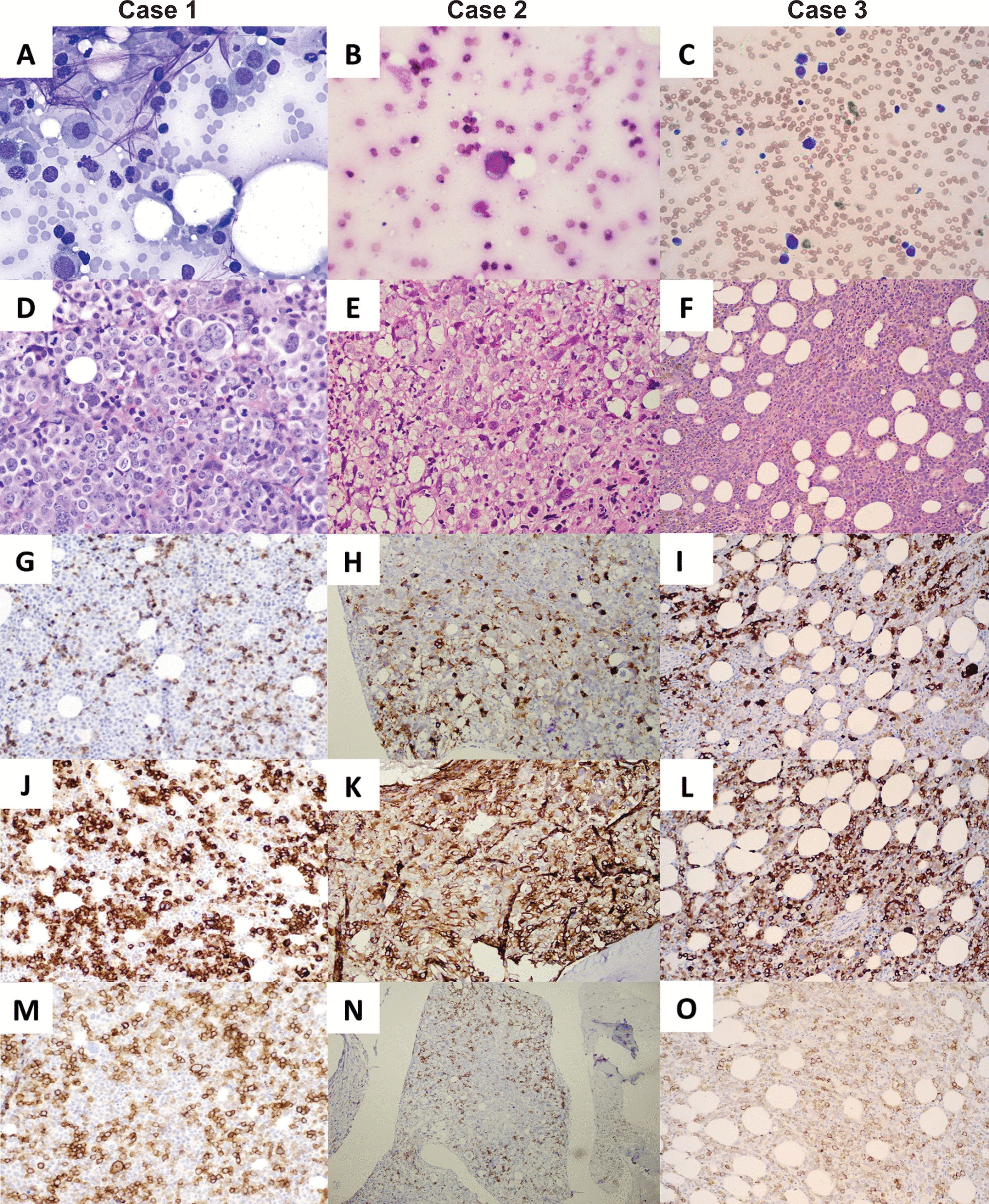
In the present case, only the biopsy, but not the smear, could confirm the presence of BP. The microscopic findings suggestive of blast crisis of a lymphoid lineage included the presence of large sheets of mononuclear cells, which could correspond to the accumulation of immature cells in extramedullary sites. Confirmation was made through an immunohistochemical study, with the expression of specific markers of lymphoblasts.
It is known that some patients with CML in chronic phase will progress to a BP. This may be due either to tumor genomic changes or to patients’ pharmacogenetic profiles of resistance to therapy [8]. The presence of BP at diagnosis is particularly uncommon (less than 5% of cases), with a higher prevalence (2–3 times) of myeloid BP compared to lymphoid [9, 10]. From a pathophysiological point of view, evolution to lymphoid BP does not appear to be associated with additional copies of the Ph chromosome or trisomy 8, but rather with specific additional mutations in genes such as IKZF1, CDKN2A/B, and BCORL [8].
The diagnosis of lymphoid BP, albeit uncommon, can be relatively straightforward if there is a clear lymphoblastic component evident in the bone marrow aspirate [11]. It is also possible the finding of different disease stages between the medullary study (showing chronic phase) and extramedullary tissue (showing lymphoid BP) [12, 13]. However, to the best of our knowledge, the simultaneous detection (“collision”) of the two components (chronic phase and lymphoid BP) in the same bone marrow biopsy sample of CML is very rare. Furthermore, the role that the biopsy played in the present case is noteworthy, since the initial percentage of blasts detected on BM smear and flow cytometric analysis was low. In this setting, a retrospective study of 508 patients with CML demonstrated that bone marrow biopsy was essential or helpful for diagnostic evaluation in 25% of cases. The need for biopsy was indeed more common in patients with BP, compared to the chronic phase of the disease, and in cases where aspirates were insufficient [14]. A possible explanation for the discrepancy in findings between our biopsy and bone marrow aspirate includes the presence of reticulogenesis. Also, the biopsy enabled examination of an undiluted, much larger sample of hemopoietic tissue that could disclose localized sheets of lymphoid blasts which comprised one-third of the area of the section. So, the distribution of the blasts was not homogeneous.
The immunohistochemical study in lymphoid BP of CML usually shows positivity for TdT and CD34 in lymphoid precursors, in addition to pan-B markers such as PAX-5 and CD79a in the case of “B” lymphoid crises [2]. Sometimes, a differential diagnosis between CML in lymphoid BP and Ph-positive acute lymphoid leukemia (ALL) is warranted, which is challenging and must take into account a combination of clinical, morphological, and molecular findings. In this sense, in the former, evidence is needed to support CML (presence of leukocytosis with maturation arrest of the granulocytic series, small and hypolobulated megakaryocytes). In contrast, the presence of small breakpoint mutations in BCR genes, patients of a younger age group, and no previous history of CML favor ALL [15].
The therapeutic strategy in CML consists of TKI in the chronic phase. As for patients in the BP who have not been previously treated, a complete hematological response with TKI occurs in only 50% of cases, and the addition of other drugs such as prednisolone and vincristine is often necessary in lymphoid BP. Despite this, responses are short, and relapses may occur in these patients after a few months, making it necessary to schedule an allogeneic bone marrow transplant if the patient is eligible [4]. In our case, the bone marrow biopsy was crucial for an accurate diagnosis, as it made it possible to include the patient in a more intensive treatment group, despite the final dismal outcome.

Comments (0)