
Remember me
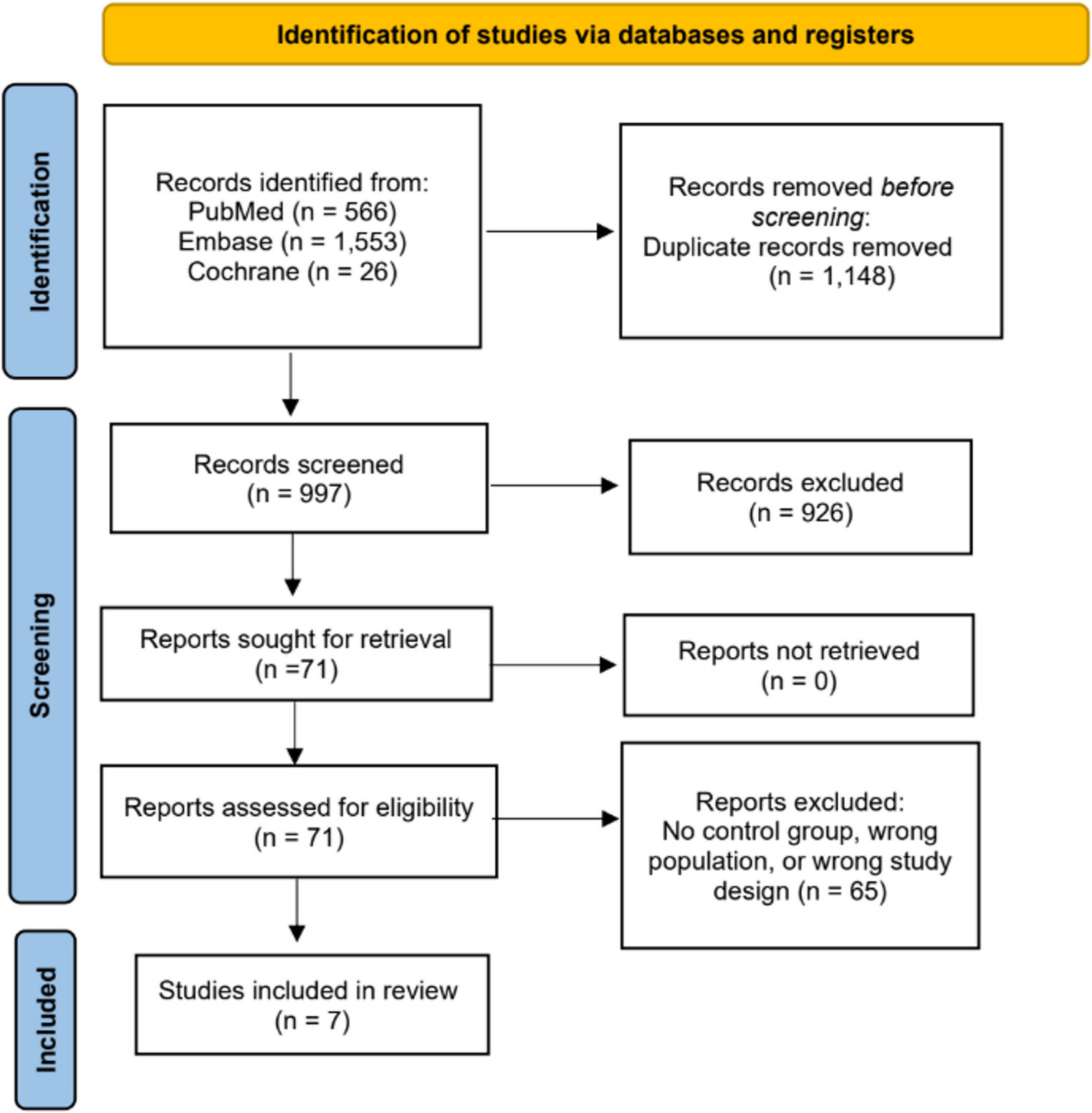
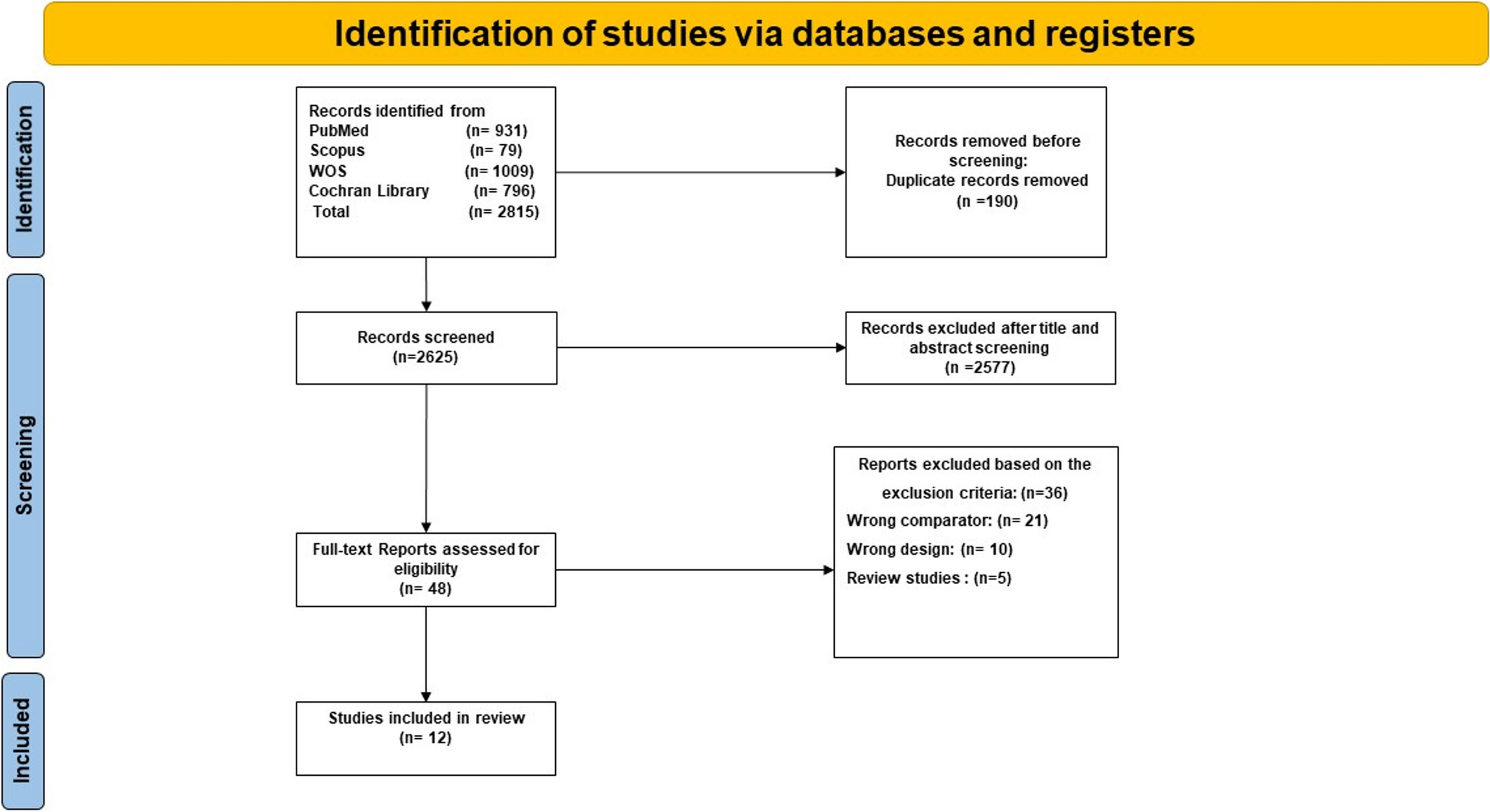
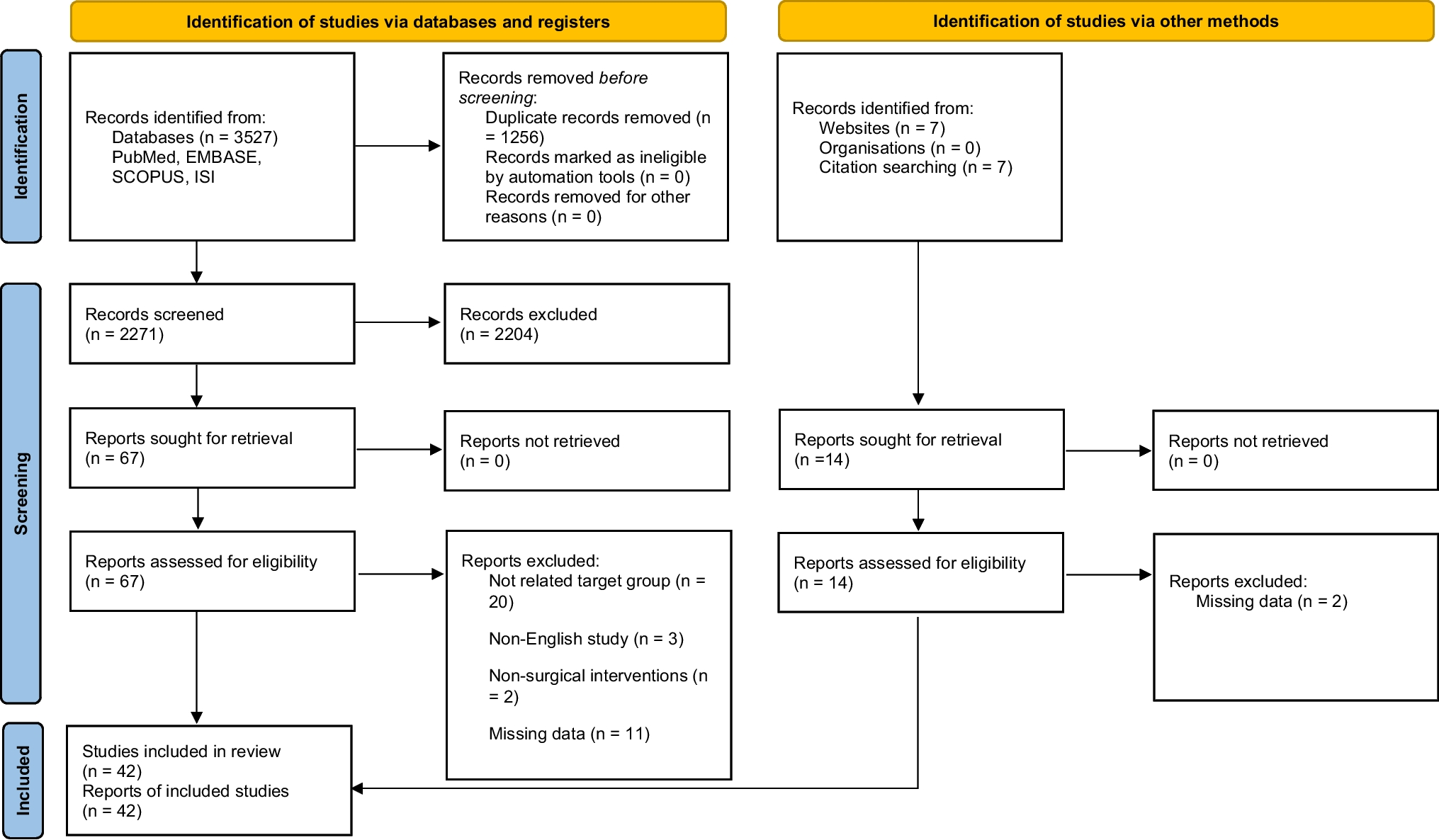
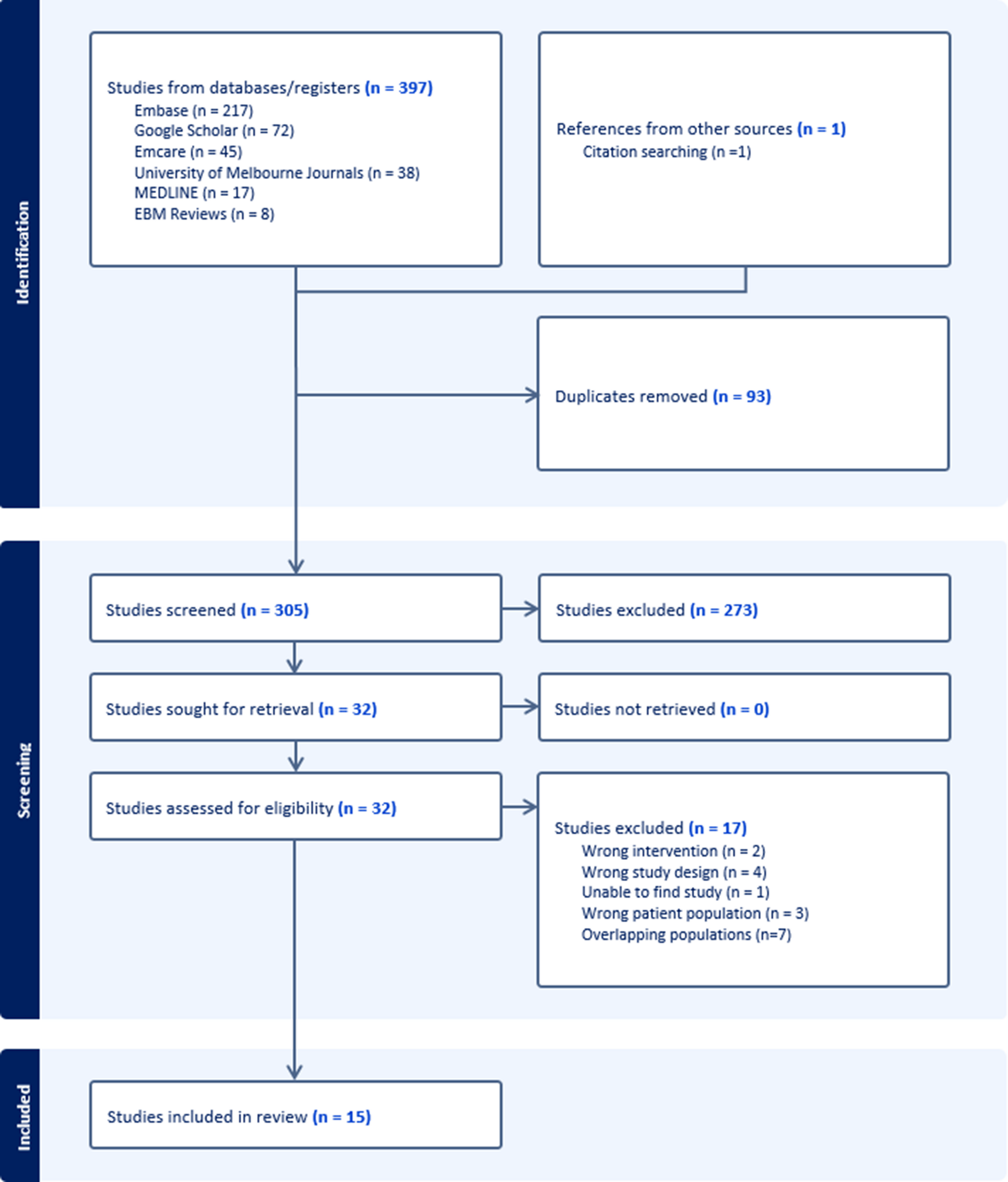
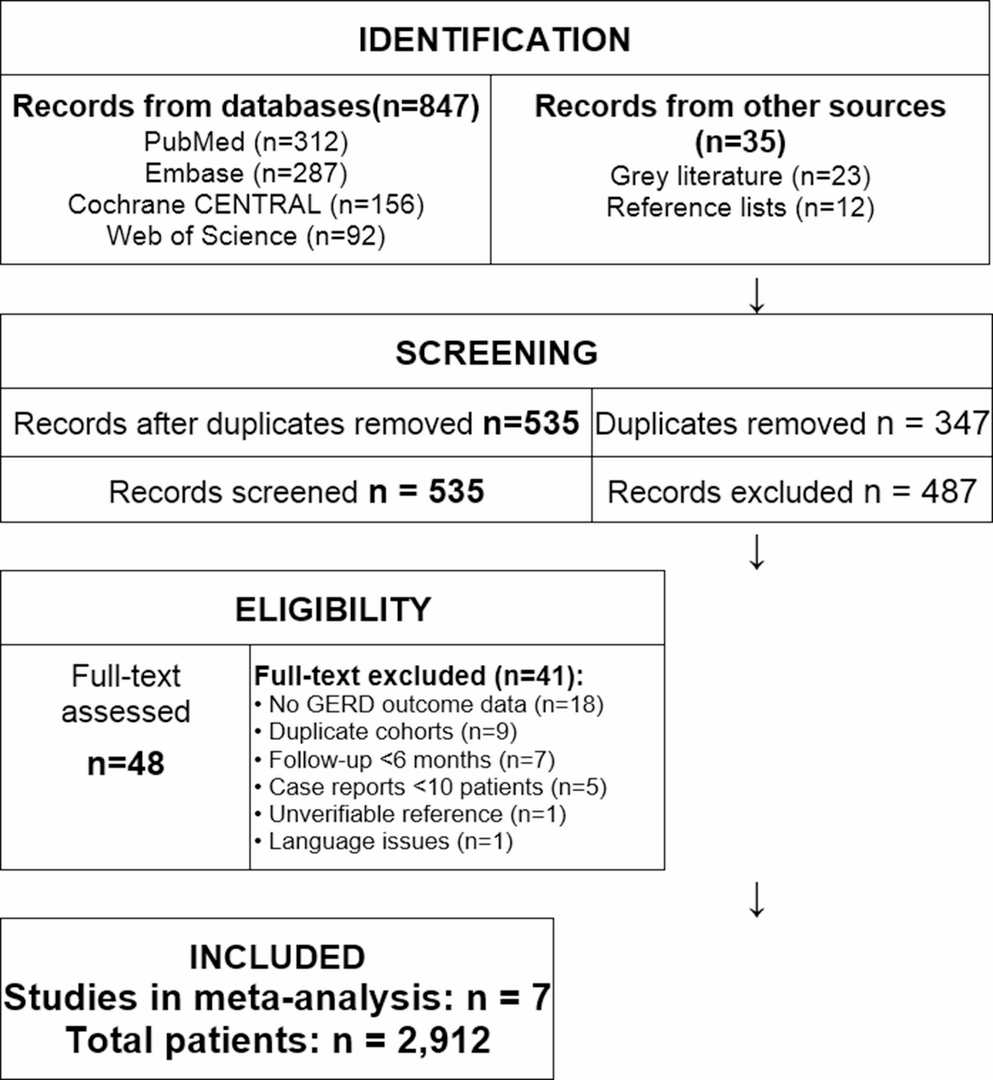
Our literature search identified 397 unique articles, with an additional article found via manual citation searching. Following screening by title and abstract, 32 articles progressed to full-text analysis. Of these, 15 articles satisfied the eligibility criteria and were included in this scoping review (Fig. 1).
Fig. 1
PRISMA flowchart depicting search strategy
Overview of Studies15 studies evaluated the role of GLP-1 RMs for use in patients with dumping syndrome post-MBSand were included in this scoping review [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30] (Table 1).
Table 1 Overview of StudiesOf these, 12 examined cases using GLP-1 receptor agonists, two used GLP-1 receptor antagonists, and one used a dual GLP-1 receptor agonist and glucose-dependent insulinotropic polypeptide (GIP). The majority were published in the United States of America (7/15, 46.67%) followed by Germany (2/15, 13.33%), the United Kingdom (2/15, 13.33%), Sweden, Kuwait, Italy and Colombia (all 1/15, 6.67%). The most common study design was case reports and case studies (8/15, 53.33%) followed by case series (4/15, 26.67%). Overall, these studies encompassed 107 individual patients. Despite variable reporting, most studies report a predominance of female participants with age ranging from 31 to 60 years, with an estimated mean around 44.2 years of age. The most common bariatric surgery performed was a gastric bypass (including Roux-en-Y gastric bypass) (9/15 studies, 60.00%). There was incomplete reporting of body mass index and weight lost variables.
Outcomes15 studies involving 107 patients were assessed which suggested some benefit including potential resolution or reduction in hypoglycaemic episodes and/or symptoms and/or glucose stabilising effects in all cases treated with GLP-1 RMs (Table 2). They were then separated in areas of interest into the modulation effect on GLP-1 – either receptor agonism, antagonism, or combined agonist with GIP.
Table 2 The use of glucagon-like peptide 1 receptor agonists in dumping syndromeHypoglycaemic EpisodesEight of the 15 studies (totalling 14 patients) demonstrated no episodes of hypoglycaemia after treatment with a GLP-1 RA [16, 17, 21,22,23,24,25,26]. Three studies (35 patients) showed a reduction in hypoglycaemic events and one case series showed a mix of 1–2 episodes (47% n = 7), complete resolution (40% n = 6) and no change (13% n = 2), however it is important to note that of the initially recruited 25 patients in this case series only 15 responded [18, 19, 21, 28].
Other Outcomes MeasuredSymptomsOther studies included the outcome of symptoms of dumping syndrome. These can include nausea and/or vomiting, abdominal distention, diarrhoea, sweating, feeling light-headed, or palpitations [31]. Seven studies (44 patients) had reduction or resolution of symptoms of dumping syndrome after the use of GLP-1 RM treatment [19,20,21,22, 24, 29, 30] Both the GLP-1 receptor agonist and 2 of the 3 antagonist modulators had subjective symptomatic relief in their outcomes (with the third antagonist case control series not reporting on symptoms as an outcome) [19, 21, 27].
Stabilisation of Glucose LevelsSeveral studies’ outcomes showed that GLP-1 RMs may have a stabilising effect on glucose levels. One crossover study of a GLP-1 receptor antagonist involving 16 people measured glucose peak time and rate of decline and found this to be in line with the control (non-surgical) group [19]. Another randomised placebo-controlled crossover trial of 18 subjects showed the same antagonist raised the glucose nadir by 21–26% depending on the dose (P.001 and 0.002) and decreased insulin peak by 21–23% (P 0.042 and 0.029) [20]. A third case control study of 24 participants using an antagnoist found that these effects of glucose stabilisation were stabilised more in those that had had MBS than those with no surgery [27].
In terms of GLP-1 receptor agonists (plus the mixed agonist-GIP modulator single case study), this similarly showed reduction in postprandial glucose peak and more appropriate insulin peak and timing after induction the intervention which subsequently responded to improved symptoms (total 7 patients) [29, 30]. Similarly, time spent with blood glucose level < 70 mg/dL was decreased from 12% to 1% in a case report that utilised continuous glucose monitoring after uptitration to full dose of an agonist [22].
Qualitative MeasuresOther outcomes were quality of life/mood improvement, included as an outcome in 3 case reports and appeared to have positive benefits associated with GLP-1 RMs [22,23,24]. These were all GLP-1 receptor aognists.
Adverse EffectsA case series of three patients using GLP-1 receptor agonists reported that one out of three participants developed post prandial vomiting, however this resolved with education on only eating to satiety and subsequently resolved without any dose reduction [15]. One case study of a GLP-1 RM used in conjunction with Acarbose (an alpha-glucosidase inhibitor) reported unintentional weight loss (amount not disclosed) however this stabilised with regular meals [23]. 12 studies (85 participants) did not report on adverse effects [16,17,18,19,20,21,22, 24,25,26,27,28].
Further reports on GLP-1 receptor agonists include a case series of five patients reported some potential rebound symptoms in those who either ceased or reduced their GLP1-RA, both of which resolved after recommencing or downtitrating to previous dosing [26]. One experienced subjective palpitations and nausea which transitioned to abdominal pain and nausea on switching from Liraglutide to Exenatide so treatment with GLP1-RM was ceased despite its good results with dumping syndrome (symptoms and frequent hypoglycaemic episodes have subsequently returned). The fifth case in this particular series also experiences nausea and headache when dose of the GLP-11 RA (monotherapy) was uptitrated to aim to cease all hypoglycaemic episodes (having already had markedly reduced). Therapy was switched to a different GLP1-RM and side effects resolved without any further hypoglycaemic episodes [26].
One study of a GLP-1 receptor antagonist found that there were no increased adverse events in the 28 days period the intervention was applied [20]. In another, investigators had to intervene in the placebo group (not the antagonist) due to low plasma glucose levels so although this is not a safety effect profile of the drug itself, it does indicate some risk that should be considered given the recommendations into further research this scoping review provides [19]. The third antagonist study did not comment on side effects or safety [27].
The combined agonist-GIP therapy cited insurance issues with getting Tirzepatide for longer than 6 weeks, after which symptoms of dumping syndrome returned [30].
Type of Dumping SyndromeOf the studies meeting inclusion criteria, nine (57 participants or 53.27%) looked at late dumping syndrome, five (49participants or 45.79%) did not report on the kind of dumping syndrome studied and one case study looked at both early and late dumping syndrome [15,16,17,18,19,20,21,22, 24,25,26,27,28,29].
Methods of Collecting Data On Dumping SyndromeStudies utilised variable methods to collect data on diagnosis of dumping syndrome. Nine studies used only a single method, six studies included multiple measurements, and two case reports did not disclose how they collected their data. Unfortunately, the largest study with 27 participants plus one other case report did not disclose how they diagnosed dumping syndrome [15, 28]. However, the next two largest studies (totalling 42 participants) used the Mixed Meal Tolerance Test (MMTT) to diagnose dumping syndrome which was an equal amount of people overall who were diagnosed using symptoms across other studies (also 42) [15,16,17,18,19,20, 25, 27, 28]). The Oral Glucose Tolerance Test (OGTT) was used in 35 patients through four studies [18, 19, 21, 29]. Then, continuous glucose monitoring was the next most used method of measuring outcomes with 30 total patients [16, 17, 20, 22,23,24,25,26, 30]. Of these, two case reports used flash continuous glucose monitoring where participants were required to manually scan the monitor to get blood glucose levels, and the rest were continuously updating [22, 24]. Finally, point of care testing was completed in six patients although in both cases they had multiple other measures, and self glucose monitoring was measured in the study of 18 people in conjunction with other testing methods [16, 20, 26].
Type of GLP-1 Modulator Used and Dosing RegimenRegarding GLP-1 receptor agonists, Liraglutide was the most used in the studies with 45 (42.06%) subjects in total [15, 21, 23,24,25,26, 28, 29]. Its dosing regimen ranged from 0.6 mg subcutaneously daily for two days, to up to 3 mg daily. Smaller amounts of cases used Semaglutide (2 case studies), both starting at 0.25 mg weekly and one uptitrating to 0.5 mg weekly after a month of 0.25 mg [16,
Comments (0)