
Remember me
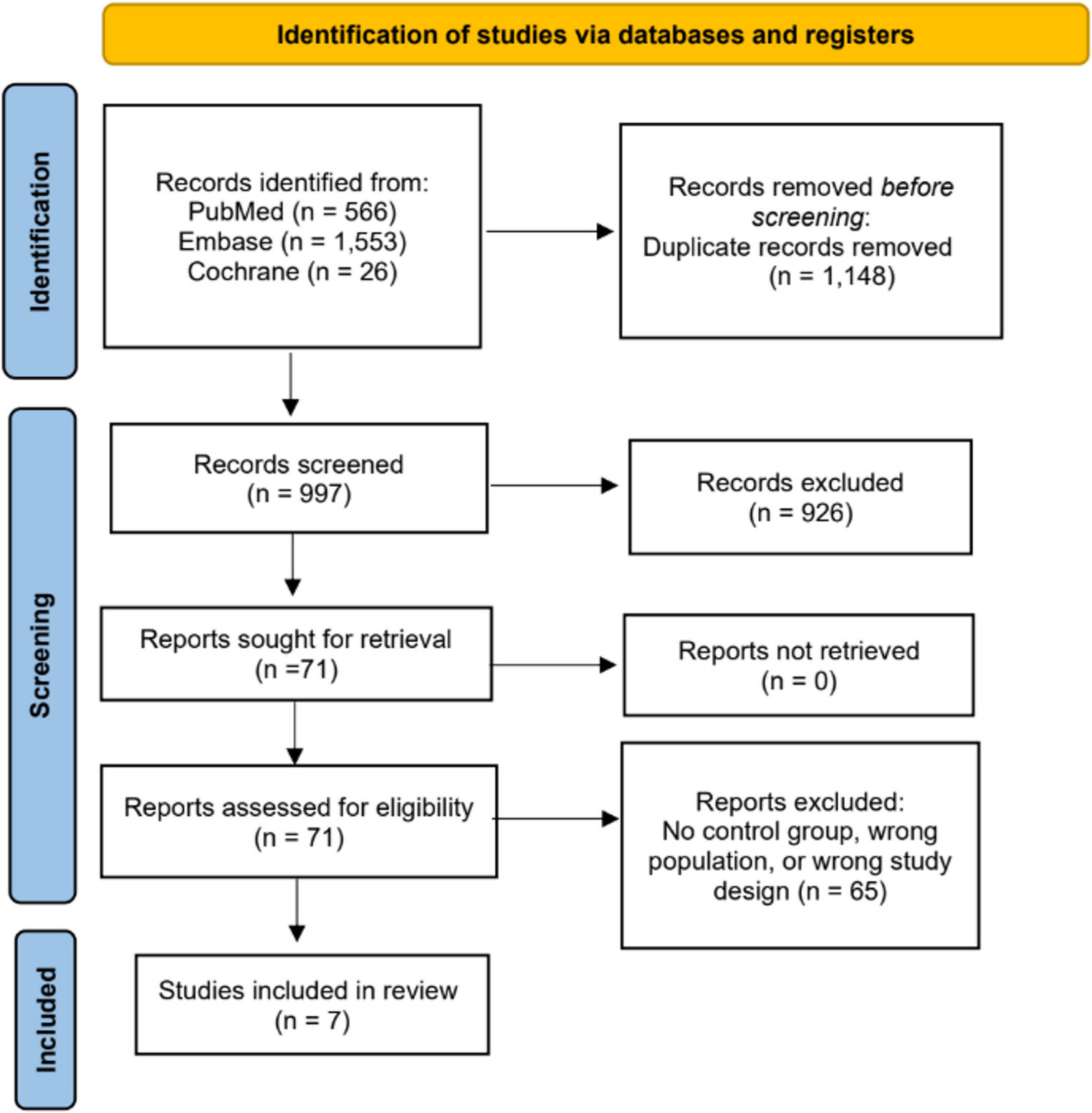
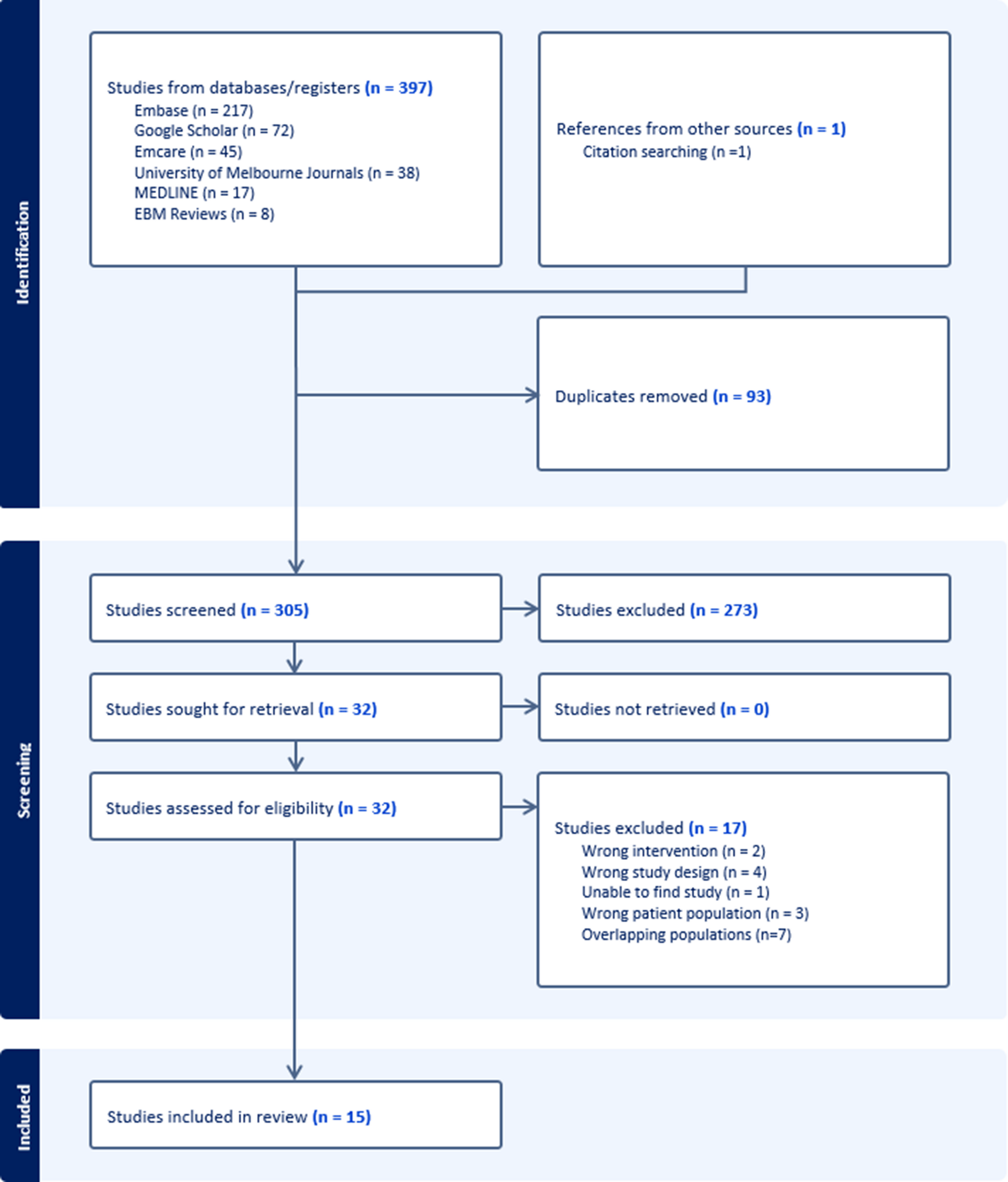
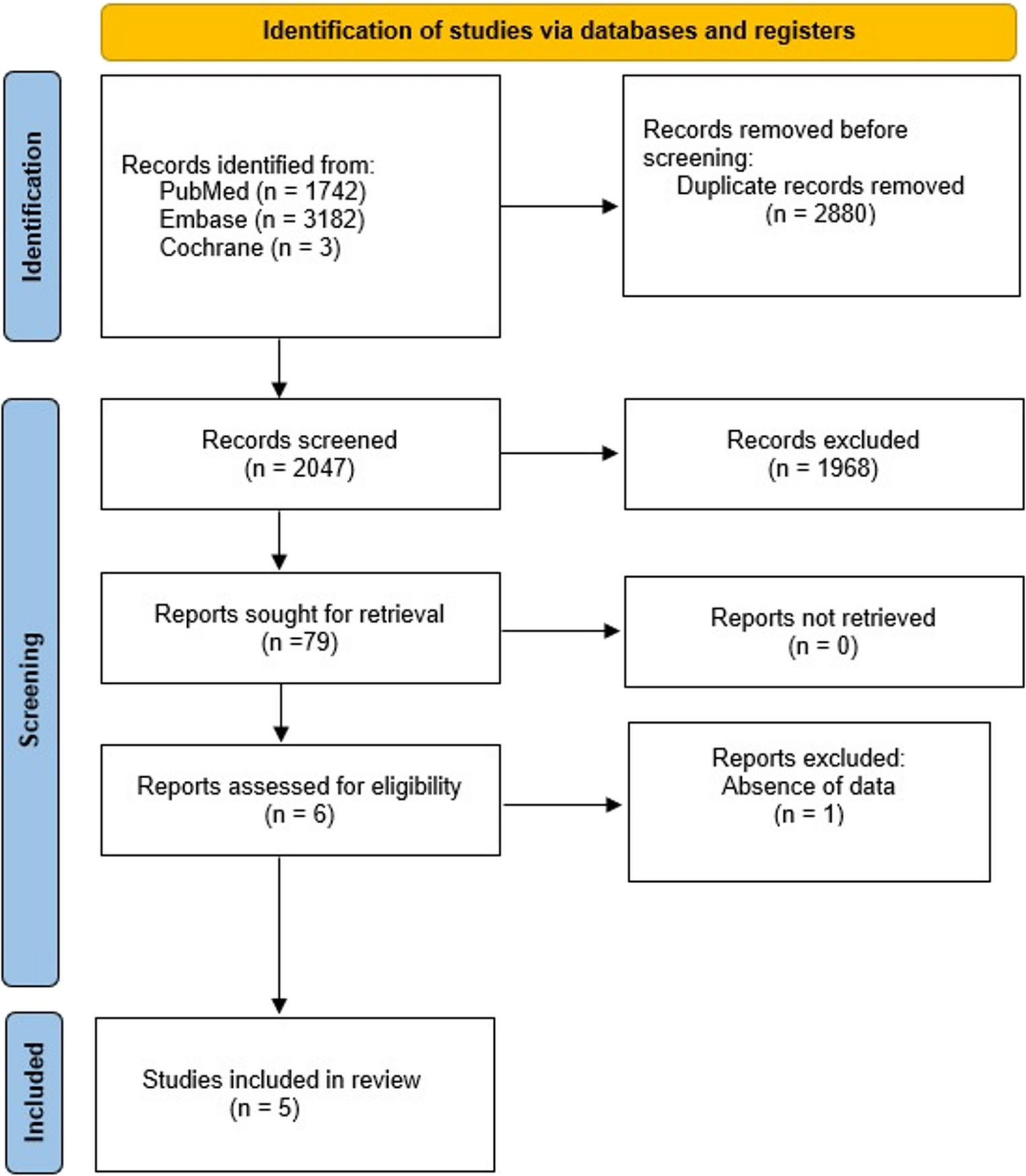
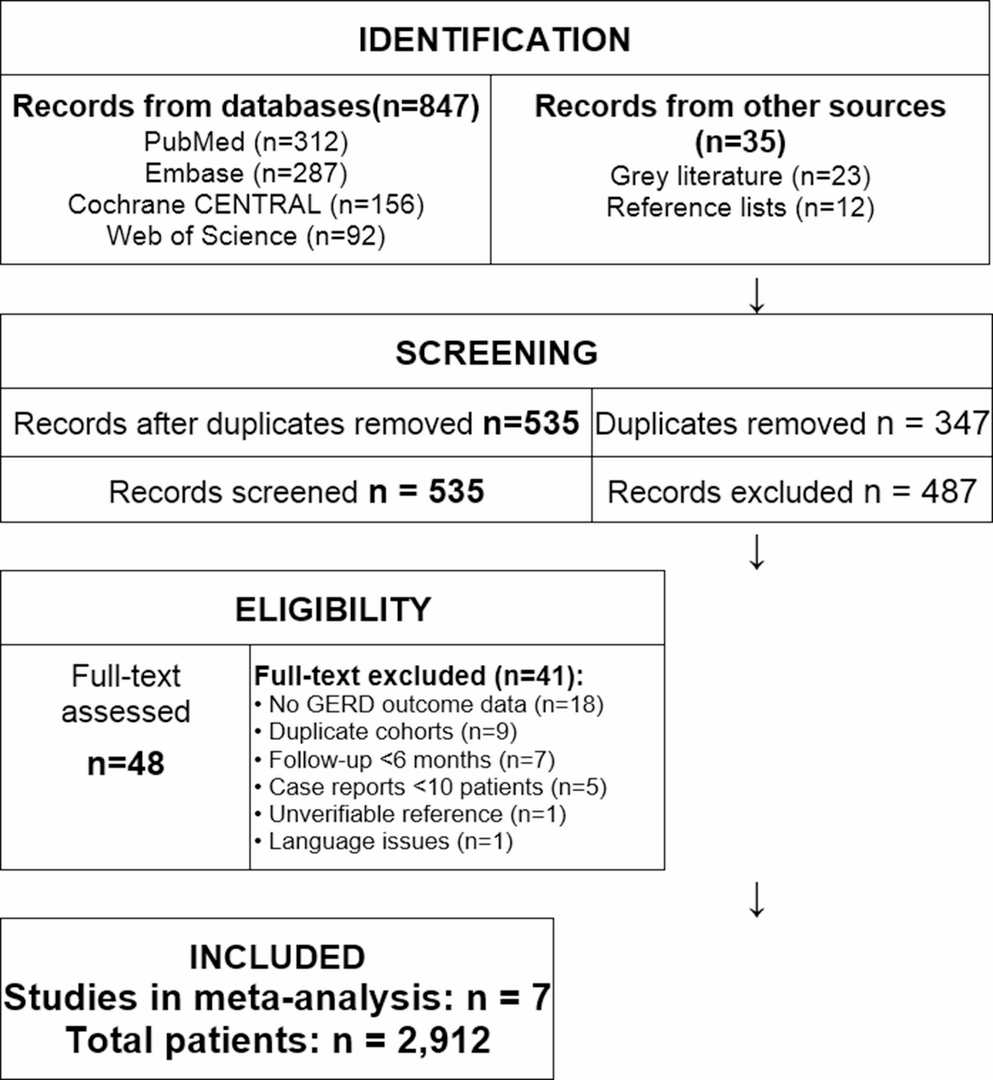
From the systematic search, we retrieved 997 studies, out of which 7 met the inclusion criteria for the final analysis. Figure 1 presents the PRISMA flowchart detailing the study selection process. Table 1 shows the details of the included studies published between 1995 and 2021. All 7 studies were observational comparative studies.
Fig. 1
PRISMA flowchart of study selection
Patient CharacteristicsTable 1 provides a summary of the demographic characteristics of the patient populations across the studies. Across the included studies, six studies evaluated a total of 439 patients, with 276 undergoing fundoplication and 124 receiving Roux-en-Y gastric bypass (RYGB); 39 patients from Braghetto et al. were excluded from the analysis because they underwent a hybrid procedure that combined fundoplication with a distal gastrectomy and Roux-en-Y gastric bypass (FVDGRYGJ) for the treatment of long-segment Barrett’s esophagus (LSBE). The seventh study, Varella et al., used data from the University HealthSystem Consortium database using “International Classification of Diseases, 9th Revision” procedural and diagnosis codes for individuals with morbid obesity with GERD, evaluating a total of 27.264 patients’ medical records. Notably, the study by Varela et al. only examined early postoperative results and did not evaluate weight loss or the control of GERD.
The mean age of the entire cohort was 54.2 years, with fundoplication patients generally older compared to those treated with RYGB. The weighted average preoperative BMI was 35.6 kg/m², highlighting the predominance of patients with obesity, particularly in the RYGB cohorts, where BMI consistently exceeded 40 kg/m² in most studies. Women comprised most of the population, with an overall female prevalence of 75.7%, and proportions above 85% in several RYGB groups.
DeMeester ScoreWe pooled preoperative and postoperative data, comparing a total of 78 patients. Figure 2 shows there was no difference between fundoplication and RYGB (MD = −1.31; 95% CI −12.11 to 9.49; p = 0.81; I²= 4%) in preoperative DeMeester score. After surgery, fundoplication shows a slightly lower score (MD = 8.86; 95% CI 4.34 to 13.39; p = 0.0001; I² = 0%). The follow-up duration for objective reflux assessment via the DeMeester score reached a weighted mean of 42.3 months (range: 19.6 to 52.0) for the fundoplication group and 35.2 months (range: 14.6 to 49.0) for the RYGB group.
Fig. 2
DeMeester score before and after surgery
ComplicationsIn our analysis of complications, we evaluated intraoperative complications, postoperative complications, and dysphagia (Figs. 3, 4 and 5). The reporting and classification of complications varied across the included studies. Betzler et al. employed the most rigorous methodology, utilizing both the Clavien-Dindo classification and the Comprehensive Complication Index (CCI) to record events during the initial hospitalization and at the 3- and 12-month follow-ups. Similarly, DuCoin et al. used the Clavien-Dindo system to categorize both in-hospital complications, such as leaks and perforations, and post-discharge outcomes, including hernia recurrence. In contrast, Varela et al. relied on an administrative model from the UHC database, which uses a complication profiler and comorbidity software to assign disease severity levels (minor, moderate, or major) and identify specific adverse events prior to discharge. The remaining studies (Braghetto et al., Colvin et al., Joseph et al., and Patterson et al.) did not utilize universal scoring systems like Clavien-Dindo, instead basing their findings on direct clinical reports, reoperation rates, hospital readmissions, and observed operative morbidity.
Fig. 3
a. Intraoperative complications. b.Intraoperative complications excluding the study by Varela et al
Fig. 4
a. Postoperative complications. b.Postoperative complications in prospective studies excluding the study by Varela et al
Fig. 5
Betzler et al. defined preoperative complications as GERD-related risks like aspiration and esophagitis, while postoperative events included intraoperative injuries (pleural/esophageal) and follow-up issues such as dysphagia, leaks, and ulcers. Braghetto et al. viewed preoperative complications as esophageal ulcers or strictures resulting from Barrett’s, with postoperative outcomes focusing on dumping syndrome, diarrhea, and surgical leaks. Colvin et al. highlighted Barrett’s esophagus and cancer as preoperative concerns, whereas postoperative complications involved marginal ulcers, bloating, and the need for dilation. Joseph et al. considered esophagitis and adenocarcinoma as preoperative complications, noting a “complicated hospital course” involving respiratory issues postoperatively. Ducoin et al. described preoperative complications through chronic respiratory symptoms (cough/dyspnea), while postoperative events included hernia recurrence, intestinal obstructions, and arrhythmias. In contrast, Patterson et al. noted no postoperative complications in their small sample, despite preoperative comorbidities like sleep apnea. Finally, Varela et al. used a broad administrative definition, categorizing postoperative complications into procedure-related (e.g., perforation, bleeding) and non-procedure-related (e.g., pneumonia, thromboembolism) based on illness severity.
Intraoperative complication rates (Fig. 3) demonstrated a significant reduction in patients undergoing RYGB compared with fundoplication (RR = 0.66; 95% CI 0.53 to 0.81; p < 0.0001; I² = 0%). This finding indicates greater intraoperative safety associated with the bariatric approach. Conversely, postoperative complications (Fig. 4) were more frequent in the RYGB group (RR = 1.68; 95% CI 1.34 to 2.10; p < 0.00001; I² = 0%).
Importantly, the study by Varella et al. accounted for 98.4% and 82.3% of the total complications, and due to its database design, we conducted a sensitivity analysis excluding this trial. After removal, no statistically significant difference was observed between groups, suggesting that the initial finding was predominantly driven by this large database (Figs. 3a and 4a).
Finally, dysphagia outcomes are presented in Fig. 5, where pooled results highlighted no consistent differences between procedures (RR = 0.84; 95% CI 0.35 to 1.99; p = 0.69; I² = 0%). Across the analyzed studies, the definition and assessment of dysphagia varied significantly. Colvin et al. utilized a dual approach, defining clinically significant dysphagia as that requiring endoscopic dilation, while also tracking symptom severity via GERSS. Betzler et al. assessed the condition through the ‘Eating/Drinking Problems’ domain of the QOLRAD questionnaire, whereas Joseph et al. relied on specific patient-reported dysphagia scores. In contrast, DuCoin et al. and Braghetto et al. evaluated dysphagia as a binary variable based on clinical reports. Lastly, Varela et al. and Patterson et al. did not provide a formal definition for this symptom, focusing on major complications or objective reflux scores.
Operative Characteristics OutcomesWe conducted a pooled analysis of length of stay (LOS), operative time, and reoperation rates to compare operative characteristics between RYGB and fundoplication (Figs. 6, 7 and 8). No statistically significant difference was observed in LOS between the two groups (MD = 0.86 days; 95% CI − 0.58 to 2.30; p = 0.24; I² = 95%). After performing a sensitivity analysis by removing the Varela et al. study (Fig. 6A), the results remained stable (RR = −1.54; 95% CI −9.96 to 6.88; p = 0.72; I² = 99%). Similarly, operative time did not differ significantly (MD = 6.76 min; 95% CI − 47.74 to 61.27; p = 0.81; I² = 81%).
Fig. 6
a. Length of stay in days b.Length of stay in days in prospective studies excluding the study by Varela et al
Fig. 7
Operative time in minutes
Fig. 8
a. Reoperation rates b. Reoperation rates excluding the study by Varela et al
Reoperation rates were slightly higher for the RYGB group in the overall analysis, also (RR = 1.43; 95% CI 0.75 to 2.71; p = 0.27; I² = 0%; Fig. 8). This trend persisted in the sensitivity analysis excluding Varela et al. (Fig. 8A), although the difference was statistically no longer significant (RR = 2.02; 95% CI 0.82 to 4.99; p = 0.13; I² = 0%).
%TWLTo assess weight loss, we evaluated the percentage of total weight loss (%TWL) at follow-up at 12 months post-surgery. RYGB was associated with significantly greater %TWL compared with fundoplication (MD = 25.09; 95% CI 20.56 to 29.62; p < 0.00001), although substantial heterogeneity was observed (I² = 88%) (Fig. 9).
Fig. 9
Total weight loss at 12 months
Patient-Reported OutcomesAcross studies, both fundoplication and RYGB significantly improved reflux-related symptoms; however, the durability and magnitude of the effects varied. In the propensity-matched analysis by Betzler et al., reflux symptom regression at 3 months was significantly higher after RYGB compared with fundoplication (92.3% vs. 25%; p = 0.0223), although the difference was not statistically significant at 1 year. Importantly, RYGB patients reported superior postoperative quality of life as measured by the BQL and QOLRAD sleep domains (p = 0.0183). Similarly, Colvin et al. demonstrated significant improvement in GERD-HRQL and GERSS scores after both laparoscopic Nissen fundoplication (LNF) and RYGB. GERD-HRQL decreased from 29 to 1.5 in the LNF group and from 36 to 9 in the RYGB group (both p < 0.01).
GERSS scores showed parallel improvements, with a trend toward lower mid-term scores after LNF, although this was not statistically significant. Conversely, Joseph et al. observed more durable symptom control at follow-up: at 2 and 5 years, GERD-HRQL scores were significantly better after fundoplication compared to RYGB (4.9 vs. 10.2, p = 0.045; 3.3 vs. 9.0, p = 0.041), suggesting potential superiority of fundoplication for selected patients. Patterson et al. confirmed that both procedures effectively reduced heartburn, with no significant difference postoperatively. However, preoperative symptom severity was greater in the fundoplication group, which showed greater relative improvement.
Esophageal Physiology and ManometryManometric findings varied across studies. Braghetto et al. had 3 groups, to maintain clinical homogeneity and strictly compare standalone procedures, patients from the Braghetto et al. study who underwent the hybrid FVDGRYGJ procedure were excluded from this analysis. This specific group combined fundoplication with distal gastrectomy, which does not align with the primary objective of comparing primary fundoplication versus standard RYGB. Despite this, abnormal acid reflux remained uncommon after RYGB (9.5%), compared with 24% after fundoplication in hypotensive LES patients.
In contrast, Patterson et al. observed normalization of LES resting pressures after both LNF and RYGB. Mean LES improved from 12.9 to 35.5 mmHg after LNF (p < 0.003), and from 23.6 to 29.7 mmHg after LGB, though the latter was not statistically significant. Both groups achieved postoperative LES pressures within the normal range. However, it is important to note that this specific analysis included only 12 patients. While providing objective data, the small sample size in this subset limits the statistical power to draw definitive conclusions regarding manometric changes.
Barrett’s Esophagus and Endoscopic OutcomesRegarding Barrett’s esophagus, Braghetto et al. documented that metaplasia regressed in 51.9% in the fundoplication group and in 61.9% in the RYGB group, with no progression to dysplasia observed in either group. These findings support both fundoplication and RYGB as effective interventions for controlling disease progression, though mechanisms differ (anatomical reinforcement vs. acid diversion).
Risk of BiasThe risk of bias assessment of the included non-randomized studies, conducted using the ROBINS-I tool, revealed that most of the available evidence presents significant methodological limitations, resulting in an overall high risk of bias. Specifically, five out of seven studies were rated as having a critical risk of bias (Betzler et al [6], Colvin et al [7], DuCoin et al. [8], Joseph et al. [9], Patterson et al. [10]), one as serious (Braghetto et al. [11]), and only one as moderate (Varela et al. [12]). The domains most frequently associated with elevated risk were due to confounding, outcome measurement, and missing data.
Comments (0)