
Remember me
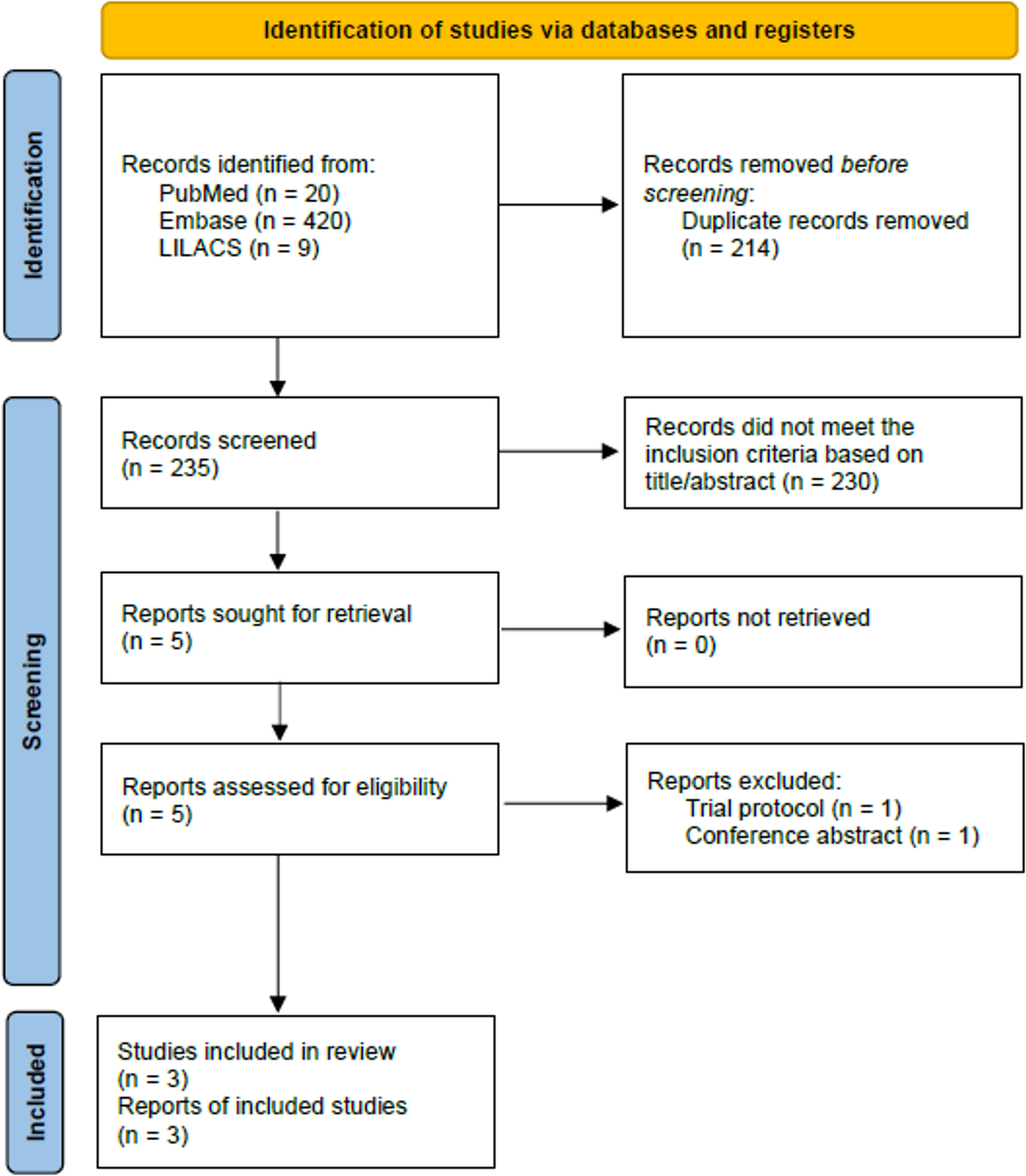
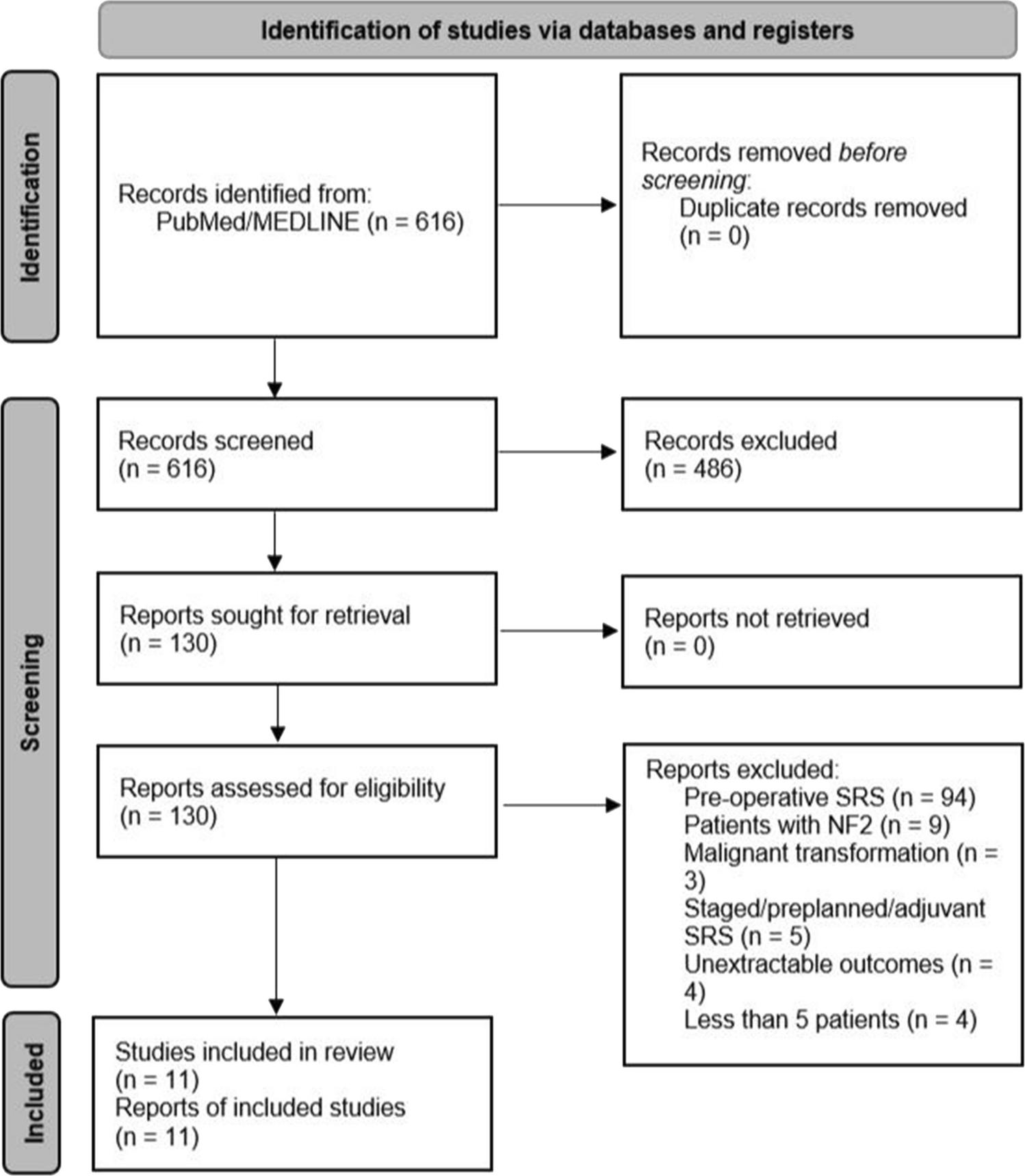
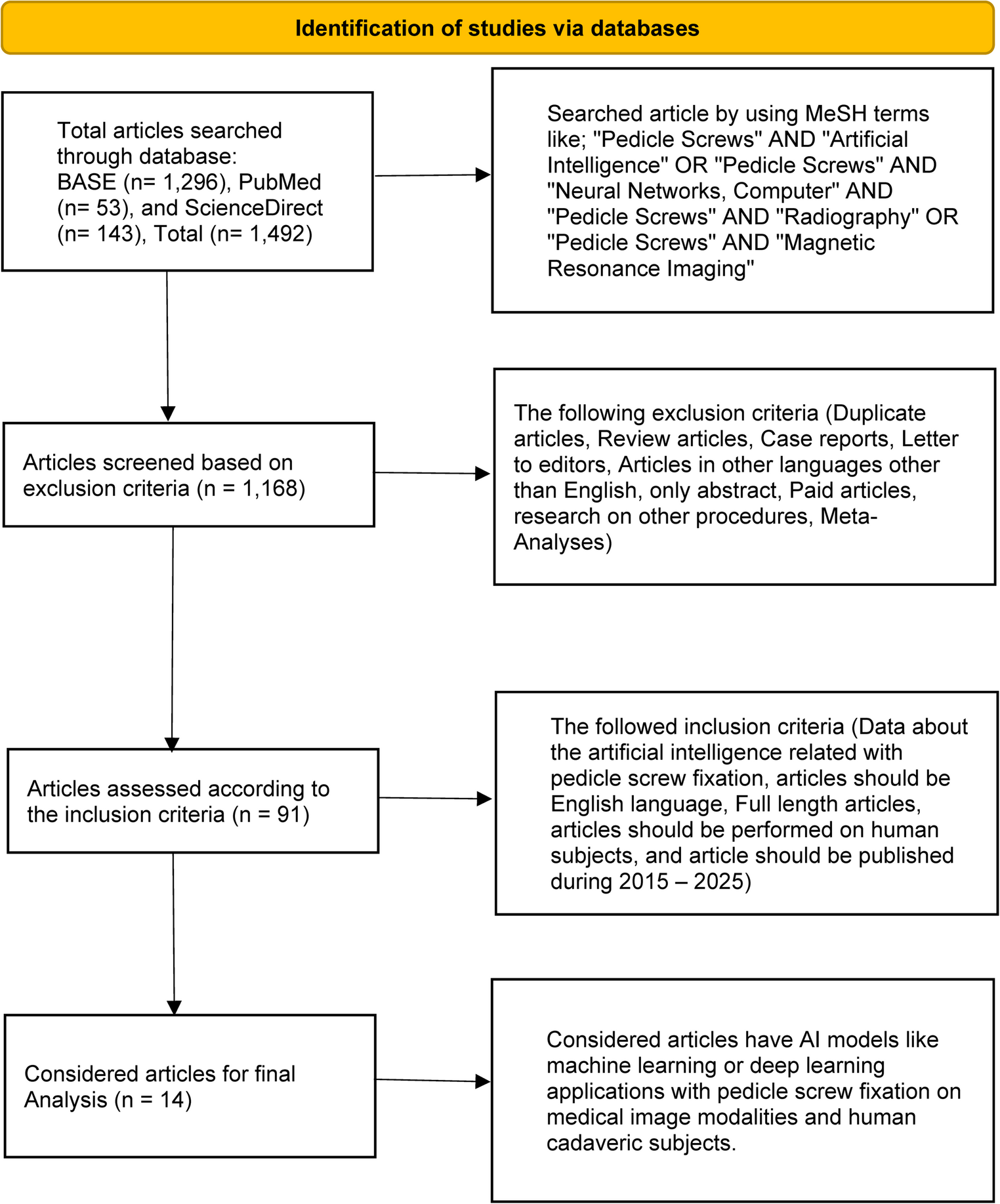
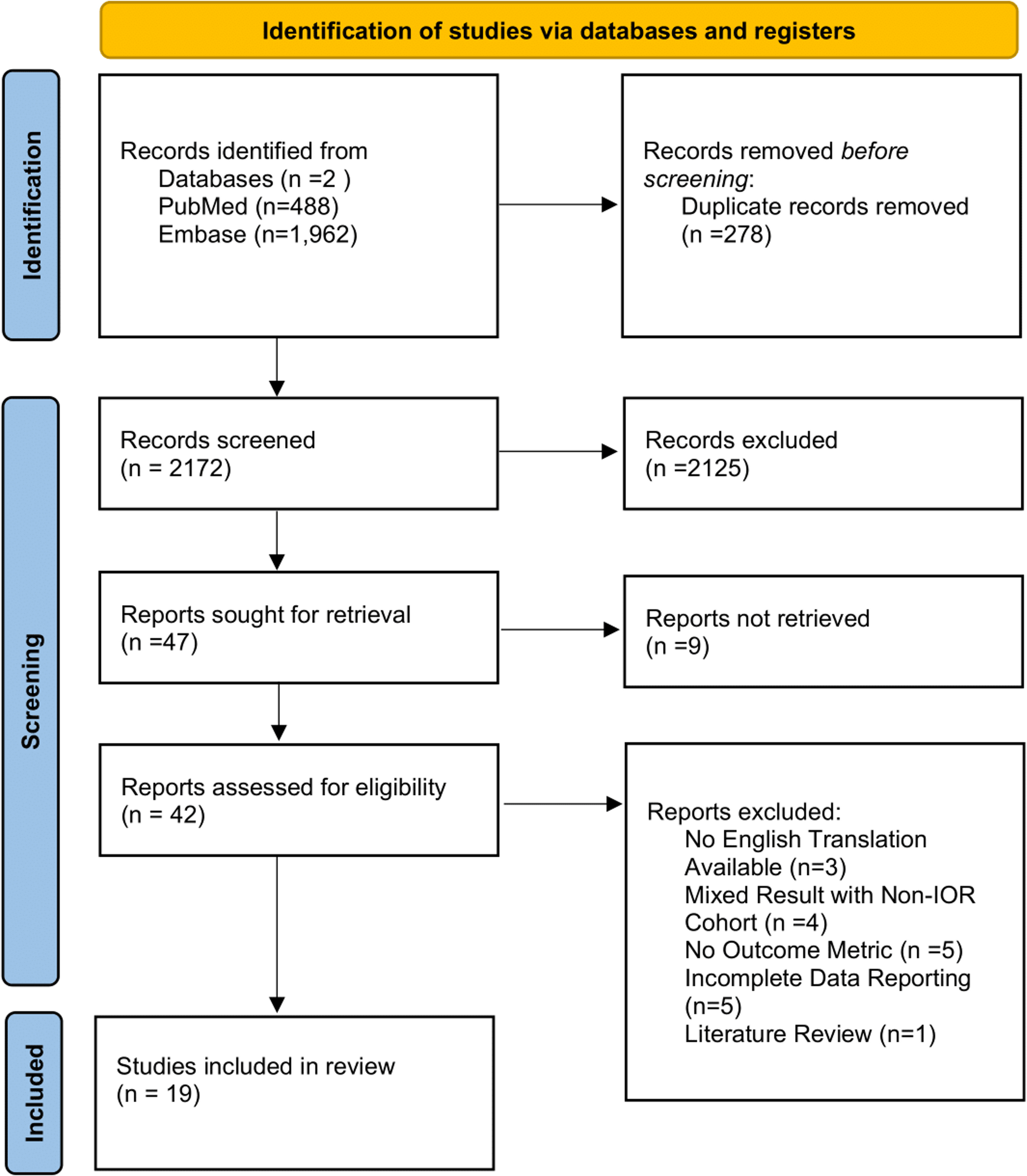
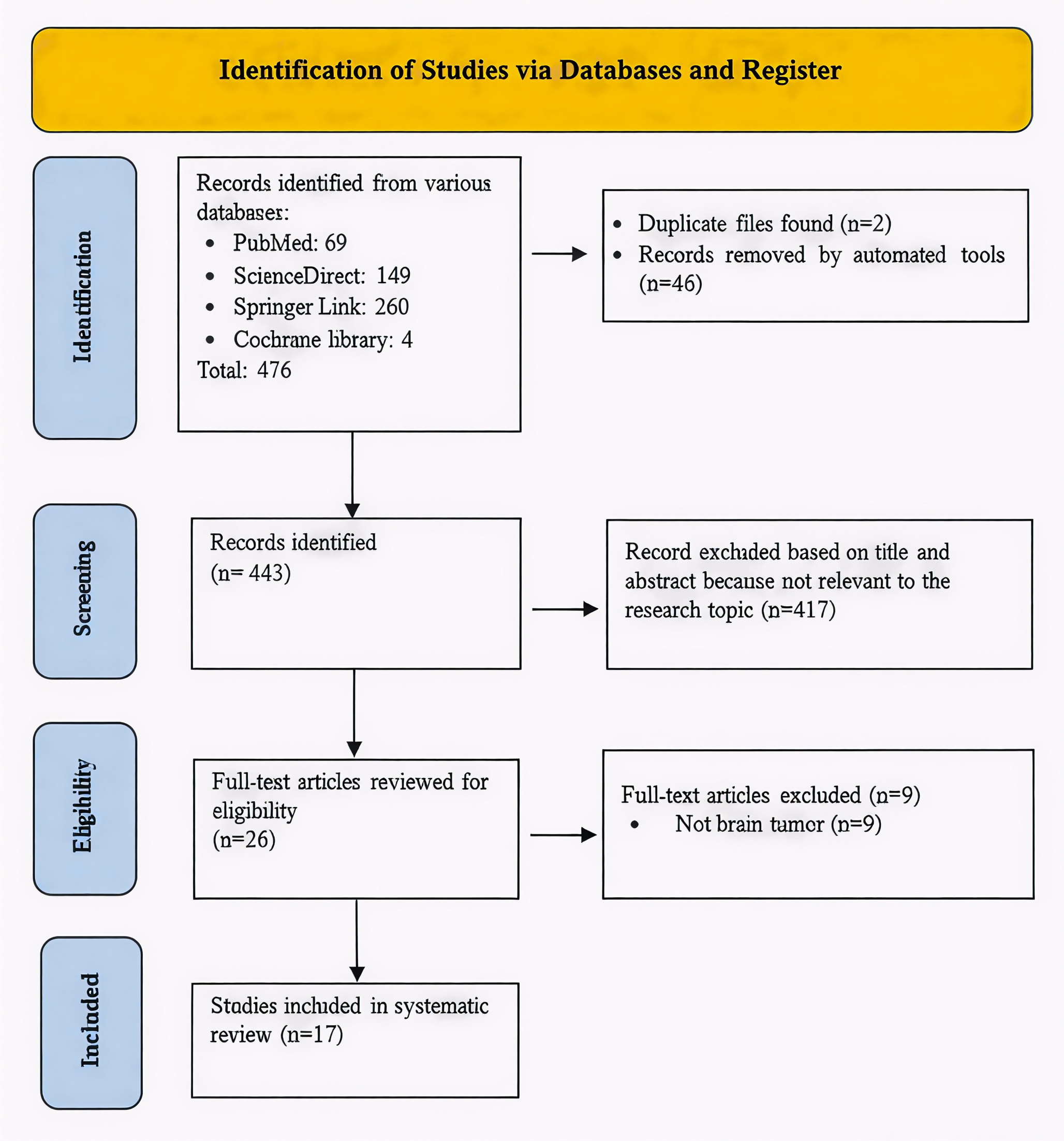
A total of 17 articles with 2,066 patients met the inclusion criteria. The study selection process is illustrated in Fig. 1. Study and patient characteristics are presented in Table 1.
Risk of biasThe analysis included 3 randomized controlled trials (RCTs). Two studies were evaluated as having a low risk of bias, with the number of low-risk points being at least equal to the number of unclear points, while one study had an overall unclear risk of bias. Table 2 summarizes the risk of bias assessment for the included randomized studies.
Across the three included RCTs, most domains—randomization process, missing outcome data, and selection of reported results—were rated as low risk of bias. Some uncertainties were noted, specifically regarding the effect of assignment to intervention and adherence (unclear in 2/3 studies) and outcome measurement (unclear in 1/3 studies). Overall, the RCTs demonstrated generally low risk of bias.
Fig. 1
PRISMA flow diagram illustrating the study selection process for inclusion in the systematic review
A total of 14 non-randomized and cohort studies were included in the analysis. NOS scores for these studies ranged from 6 to 7, indicating high quality. Detailed NOS scoring for each study is provided in Table 3.
All included non-randomized studies were rated as zero for item S4, reflecting uncertainty regarding confirmation that outcomes were not present at baseline. Furthermore, four of fourteen studies received a zero score for item O3, indicating inadequate or unclear follow-up. Overall, these issues represent the most common potential sources of bias among the non-RCTs included in this analysis.
Table 1 The list of publications included in this meta-analysisTELD vs. IELDAdverse effectsStudies where the occurrence of adverse effects was zero were excluded from the analysis. Seven studies with a total of 864 patients (TELD = 428, IELD = 436) were combined to evaluate the complication rate for the two surgical techniques. No significant effect was observed (OR = 1.02, 95% CI [0.65; 1.60], p = 0.94, I² = 0.0%, 95% CI [0.0%; 70.81%], Figure S1), with moderate-quality supporting evidence. No asymmetry was observed in the funnel plot (Figure S2).
Two subgroup analyses were performed for the complication rate. The subgroup analysis based on study design showed no significant effect, regardless of design (Figure S3). For both groups, and especially in the nonRCT group (5 of 7 studies, TELD = 359, IELD = 365), heterogeneity was considerable. Regarding operative levels, the OR of complications for L5/S1 surgeries (5 of 7 studies, TELD = 239, IELD = 267) was insignificantly lower for IELD (Figure S4). For the extensive group (2 of 7 studies, TELD = 189, IELD = 169), the source of heterogeneity remained unclear. Based on these results, the outcome of this meta-analysis demonstrates moderate-quality evidence.
Three studies with 444 patients (TELD = 233, IELD = 211) were pooled to evaluate the rate of reoperations/revisions for the two surgical techniques. No significant effect was observed (OR = 0.88, 95% CI [0.32; 2.43], p = 0.08, I² = 0.0%, 95% CI [0.0%; 89.60%], Figure S5). No asymmetry was observed in the funnel plot (Figure S6). A substantial level of heterogeneity was detected. The quality of this evidence is low.
Operative parametersTwelve studies with 1,320 patients (TELD = 696, IELD = 624) provided data on operative time. IELD procedures were insignificantly shorter (MD = 7.85, 95% CI [-1.72; 17.42], p = 0.11, I² = 97.39%, 95% CI [96.51%; 98.05%], Figure S7). No asymmetric funnel plot was observed (Figure S8). We identified notable heterogeneity across studies.
Table 2 Risk of bias assessment for RCTsTable 3 Newcastle-Ottawa Scale (NOS) study assessmentThe subgroup analysis based on study design showed that, regardless of study design, procedure time was shorter in IELD, although the difference was not statistically significant (Figure S9). This analysis included 3 RCTs (TELD = 119, IELD = 119) and 9 non-RCTs (TELD = 577, IELD = 505). Heterogeneity was considerable in both subgroups. Overall, these findings indicate that the evidence regarding procedure time is of low quality.
Six studies with 531 patients (TELD = 273, IELD = 258) reported data for fluoroscopy shots. The number of fluoroscopy shots was significantly lower in the TELD group (MD = 7.31, 95% CI [5.39; 9.23], p< 0.0001, I² = 98.51%, 95% CI [97.86%; 98.96%], Figure S10). The asymmetry of the funnel plot was not observed (Figure S11). All studies reported an outcome in favor of IELD.
The subgroup analysis based on the study design showed that, independently of the levels operated, the effect was significant for IELD (Figure S12). This analysis included 4 studies involving L5/S1 procedures (TELD = 188, IELD = 164) and 2 involving extensive-level procedures (TELD = 85, IELD = 94). While the overall effect demonstrated statistical significance, caution is warranted in interpreting the results due to the high level of heterogeneity, which may affect the reliability of the general findings. Based on these results, the outcome of this meta-analysis demonstrates low quality.
Five studies with 751 patients (TELD = 400, IELD = 351) provided data on blood loss. The blood loss for IELD was insignificantly lower than that of TELD (MD = 1.00, 95% CI [-0.72; 2.72], p = 0.26, I² = 60.53%, 95% CI [0.0%; 85.21%], Figure S13). The asymmetry of the funnel plot was not observed (Figure S14). The analysis revealed moderate heterogeneity. The subgroup analysis based on the operative levels (L5/S1: 2 studies; TELD = 144, IELD = 168; extensive: 2 studies; TELD = 151, IELD = 164), and L4/L5: 1 study TELD = 105, IELD = 19) showed that, for the extensive group, the effect was significant for IELD (Figure S15). Based on these results, the outcome of this meta-analysis demonstrates moderate quality.
Three studies with 182 patients (TELD = 94, IELD = 84) provided data on radiation dose. The dose for IELD was insignificantly lower than that of TELD (MD = 0.21, 95% CI [-0.09; 0.51], p = 0.18, I² = 98.62%, 95% CI [97.61%; 99.20%], Figure S16). The asymmetry of the funnel plot was not observed (Figure S17). The analysis indicated a high degree of heterogeneity. Based on these results, the outcome of this meta-analysis demonstrates low quality.
Postoperative bed and hospital staySix studies with 666 patients (TELD = 312, IELD = 354) reported data on postoperative bed stay. The duration of bed occupancy after the procedure was not dependent on the procedure itself, although there was a slight preference for TELD (MD = -0.04, 95% CI [-0.09; 0.02], p = 0.15, I² = 90.03%, 95% CI [81.00%; 94.76%], Figure S18). Funnel plot analysis showed no asymmetry (Figure S19).
The subgroup analysis based on the study design showed that a significantly shorter postoperative bed stay was present for RCT studies (Figure S20). This analysis included 3 RCTs (TELD = 119, IELD = 119) and 3 non-RCTs (TELD = 193, IELD = 235). For both groups, there was evidence of pronounced heterogeneity. Although the overall effect for one subgroup demonstrated statistical significance, caution is warranted in interpreting the results due to the high level of heterogeneity, which may affect the reliability of the general findings. The second subgroup analysis based on the operated levels showed that, for the extensive group, the effect was not significant and both groups exhibited high heterogeneity (Figure S21). This analysis included 2 studies involving extensive-level procedures (TELD = 106, IELD = 130) and 4 studies involving L5/S1 procedures (TELD = 206, IELD = 224). Based on these results, the outcome of this meta-analysis demonstrates low quality.
Nine studies including 1,030 patients (TELD = 508, IELD = 522) reported data on total hospital stay. Hospital stay was slightly shorter in the TELD group, although the difference was not statistically significant (MD = − 0.04, 95% CI [− 0.17; 0.09], p = 0.54, I² = 25.04%, 95% CI [0.0%; 64.81%], Figure S22). Funnel plot analysis showed symmetry (Figure S23). The level of heterogeneity was low.
The subgroup analysis based on the study design (2 RCTs: TELD = 80, IELD = 78; 7 nonRCTS: TELD = 428, IELD = 444) showed that a significantly shorter hospital stay was present for RCT studies (Figure S24). For both groups, the heterogeneity was considerable. The second subgroup analysis based on the operated levels L5/S1: 5 studies; TELD = 262, IELD = 284; extensive: 3 studies; TELD = 192, IELD = 216), and L4/L5: 1 study TELD = 54, IELD = 22) showed that, for both the L5/S1 and extensive groups, the effect was not significant (Figure S25). The effects for the subgroups were opposite, with procedures on the L5/S1 levels favoring TELD, while favor for IELD was reported for extensive levels. Based on these results, the outcome of this meta-analysis demonstrates moderate quality.
Clinical evaluationFour studies with 445 patients (TELD = 214, IELD = 231) presented data for VAS back pain score (VAS LBP). The effect for VAS LBP value was significant for TELD (MD = -0.10, 95% CI [-0.15; -0.05], p < 0.0001, I² = 0.0%, 95% CI [0.0%; 84.69%], Figure S26). The asymmetry of the funnel plot was not observed (Figure S27). A high degree of heterogeneity was observed.
The subgroup analysis based on the operative levels did not show an effect (Figure S28). The heterogeneity was considerable (L5/S1 level – 2 papers: TELD = 87, IELD = 93) or unknown (extensive group – 2 papers: TELD = 127, IELD = 138). Based on these results, the outcome of this meta-analysis demonstrates low quality.
The outcome of five studies comprising 525 patients (TELD = 253, IELD= 272) showed that the type of procedure had no impact on the VAS leg pain score at the follow-up (MD =-0.01, 95% CI [-0.07; 0.04], p = 0.64, I² = 0.0%, 95% CI [0.0%; 79.20%]) (Figure S29). The funnel plot was symmetrical (Figure S30). The source of heterogeneity was unknown.
The subgroup analysis based on the operative levels showed no significant effect (Figure S31). The results demonstrated substantial between-group heterogeneity (L5/S1 level) or unknown (extensive group). This analysis included 2 studies involving extensive-level procedures (TELD = 127, IELD = 138) and 3 studies involving L5/S1 procedures (TELD = 126, IELD = 134). Based on these results, the outcome of this meta-analysis demonstrates low quality.
Fourteen studies with 1,428 patients (TELD = 768, IELD = 660) were combined to evaluate the ODI score of the two surgical techniques. Patients who underwent IELD had insignificantly lower disability score values than those who underwent TELD (MD = 0.24, 95% CI [-0.40; 0.87], p = 0.46, I² = 45.87%, 95% CI [0.0%; 70.97%], Figure S32). The asymmetry of the funnel plot was not observed (Figure S33). There was evidence of moderate heterogeneity.
We performed three subgroup analyses for the ODI. Regarding the study design, the overall result was not significant, and the source of heterogeneity was moderate (Figure S34). This subgroup included 3 RCTs (TELD = 119, IELD = 119) and 11 non-RCTs (TELD = 649, IELD = 541). The overall effect after at least 24 months follow-up (3 papers; TELD = 134, IELD = 100) insignificantly favored IELD (Figure S35). However, heterogeneity was consistently observed in all subgroups (6 months – 6 studies: TELD = 314, IELD = 348; 12 months – 4 studies: TELD = 290, IELD = 182).
The subgroup analysis based on the operative levels showed a significant effect for the L4/L5 group (TELD = 54, IELD = 41) for two studies (Figure S36). Substantial heterogeneity was observed for the L5/S1 level (7 studies; TELD = 270, IELD = 278) and the extensive group (5 studies; TELD = 339, IELD = 341), whereas heterogeneity at the L4/L5 level could not be determined. Based on these results, the outcome of this meta-analysis demonstrates low-to-moderate quality. Seven studies with 709 patients (TELD = 356, IELD = 353) were pooled to evaluate VAS scores at the follow-up. The analysis showed that VAS was lower, although insignificant, for the IELD group (MD = 0.06, 95% CI [-0.10; 0.21], p = 0.47, I² = 21.23%, 95% CI [0.0%; 64.52%], Figure S37). The asymmetry of the funnel plot was not observed (Figure S38).
We performed three subgroup analyses for the VAS. Regarding the study design, results were opposite and the source of heterogeneity was unknown or moderate (Figure S39). This subgroup included 2 RCTs (TELD = 80, IELD = 78) and 5 non-RCTs (TELD = 276, IELD = 275). The same result was observed for the subgroups of different follow-ups (Figure S40). Outcomes were analyzed according to follow-up duration, categorized as ≥ 12 months (4 studies; TELD = 178, IELD = 142) or 6 months (3 studies; TELD = 178, IELD = 211). The levels of heterogeneity were evident for all subgroups.
The subgroup analysis based on the operative levels showed a significant effect for the L4/L5 group (one study; TELD = 54, IELD = 22) (Figure S41). The heterogeneity was considerable (L5/S1 level and extensive group) or unknown (L4/L5 level). This analysis included 2 studies involving extensive-level procedures (TELD = 109, IELD = 120) and 4 studies involving L5/S1 procedures (TELD = 193, IELD = 211) Based on these results, the outcome of this meta-analysis demonstrates moderate quality.
Comments (0)