Recurrence is a major concern for patients with RIAs undergoing coil embolization. This recurrence may also be influenced by the type of coil used. In this study, we found no significant differences in the rates of recurrence, retreatment, or favorable outcomes between the BPC and HEC groups during the 12-month follow-up period after coil embolization for an RIA.
After endovascular coil embolization for RIAs, 11% of patients required retreatment and 2.1% experienced rebleeding [13]. In particular, the incidence of rerupture was higher in cases of residual aneurysm with contrast filling along the aneurysm wall than in cases of simple neck recanalization [14]. However, recurrence can precede rupture, even in aneurysms initially considered completely occluded [13]. Therefore, in RIAs, efforts to reduce recurrence are essential to minimize the risk of rebleeding and to decrease the potential procedural complications associated with retreatment. To prevent the recurrence of coil aneurysms, bioactive coils such as first-generation HECs, Matrix, and Cerecyte were introduced with the aim of increasing durability by promoting stable thrombus formation and facilitating neoendothelialization. However, previous RCTs have failed to demonstrate the efficacy of these early-generation bioactive coils over BPCs [5, 15, 16]. Nevertheless, a study on HECs revealed a trend toward reduced major recurrence compared with BPCs, thereby generating interest in the use of HECs. However, first-generation HECs have limitations due to the large amount of hydrogel used, which results in increased coil stiffness and time constraints for placement. To overcome these limitations, second-generation HECs were developed. In two previous RCTs using second-generation HECs, the HEC group exhibited better outcomes than the BPC group [6, 8]. However, both studies included a combined population of UIAs and RIAs, with the majority of patients having UIAs; moreover, one study specifically reported that the effect of second-generation HEC seemed more pronounced in UIAs [8]. Furthermore, although patients with UIAs and those with RIAs were combined in the analysis, a recently published RCT also reported no significant difference in the recanalization rate between the BPC and HEC groups [7]. Because the results regarding the efficacy of HECs remain inconsistent and since they are based on a combined population of UIAs and RIAs, there are limitations in directly applying these findings to the treatment of RIAs. In this study, which focused exclusively on RIAs, no difference in the rate of any recurrence was observed between the BPC and HEC groups. This finding may be attributed to the higher rate of recurrence among RIAs than among UIAs, suggesting that the tendency for recurrence is similar regardless of the type of coil used. Another possible explanation is that the criteria used to define the HEC group in this study might have influenced the results. A study that used a threshold of 90% for HECs reported a significantly lower recurrence rate in the HEC group [6], whereas a study using a 50% threshold reported no significant difference [7]. In the present study, the HEC group was defined as cases in which HEC coils accounted for more than 50% of the total coils used rather than cases in which HECs were used exclusively. Owing to this classification approach, the range and median proportion of mixed use of BPC in the HEC group in this study may have influenced the evaluation of the efficacy of pure HEC and may have contributed to the absence of a significant difference in recurrence rates between the two groups. Another possible reason is that, despite extending the study period by seven months, the originally planned sample size of 118 patients was not achieved because of supply issues at participating centers and a low enrollment rate among eligible patients. This might have led to the reduced statistical power in this study. In fact, given the observed effect size and the existing sample size in this study, a post hoc power analysis demonstrated an estimated power of approximately 42%, suggesting that the study may have been underpowered. However, as one of the prospective RCTs specifically targeting RIAs, this study directly compares second-generation HEC with BPC, and its negative results have important reference value for clinical decision-making in this specific population. If validated in a large-scale trial focusing on RIAs in the future, these results could influence clinical practice guidelines.
In terms of the relationship between the maximum aneurysm size and the risk of recurrence, according to a previous study, HECs appear to be effective in preventing the recurrence of medium-sized aneurysms (range 3–14 mm) regardless of their rupture status, aneurysm neck size and procedural angiographic occlusion [6]. However, in a study involving aneurysms measuring 7–20 mm, the recurrence prevention effect of HECs was not demonstrated [7]. In this study, the treated RIAs were medium-sized, with an average diameter of 6.1 mm (range, 2.0-12.4); however, there was no difference in recurrence rates between the BPC and HEC groups. This result suggests that in RIAs, regardless of size, the choice of coil may not influence the risk of recurrence.
As in previous studies [6, 7], there was no significant difference in favorable clinical outcomes between the two groups in this study. The type of coil was found to have no significant effect on clinical outcomes. Although no specific selection criteria were applied other than the presence of an RIA, the majority of the enrolled patients exhibited relatively good clinical status. This may be attributable to our healthcare environment, where patients experiencing acute neurological symptoms are able to access emergency medical services or present directly to the emergency department without significant delay. Therefore, our cohort may have included a lower proportion of poor-grade subarachnoid hemorrhage (SAH) patients. If the study had included a greater number of poor-grade SAH patients, the overall clinical outcomes could be different. This potential limitation should be considered when interpreting the generalizability of our findings. In some studies using first-generation HECs, HEC has been reported to be related to aseptic meningitis and delayed hydrocephalus [17, 18]. We analyzed the rate of VP shunt operation during the follow-up period, and there was no significant difference between the 2 groups. Unlike first-generation HECs, which contain more hydrogel, second-generation HECs are not significantly associated with the occurrence of hydrocephalus.
In coil manipulation, second-generation HECs were designed to be as user friendly as BPCs due to the insertion of a hydrogel in a filament form inside the BPC, leading to delayed gel expansion. Additionally, 1-mm-diameter HECs were added to improve the ease of handling of HECs. Although previous studies have described improvements in coil handling, these claims were not substantiated by formal evaluation of the operator’s subjective experience. In this study, we assessed the perceived ease of coil manipulation among operators and found that HECs were still considered more difficult to handle than BPCs (6.3 vs. 8.6). Although baseline characteristics were similar between the two groups, stent-assisted coiling was more frequent in the HEC group, which may reflect the relatively greater difficulty in manipulating HECs during the procedure. The findings that BPCs were perceived as easier to manipulate is clinically meaningful. Improved handling may shorten the learning curve, particularly for less-experienced surgeons, and may reduce repeated adjustments during deployment, potentially leading to shorter procedural times. This aspect may have practical implications in the setting of RIAs, where time pressure and psychological stress are substantial, and procedural simplicity may help mitigate surgeon burden and enhance procedural stability. However, although the assessment of coil manipulation was performed by neurointerventionists with more than five years of experience, it was based on the surgeons’ subjective perceptions rather than objective quantitative metrics. In addition, blinding to the type of coil was not feasible, which may have introduced potential bias in the evaluation.
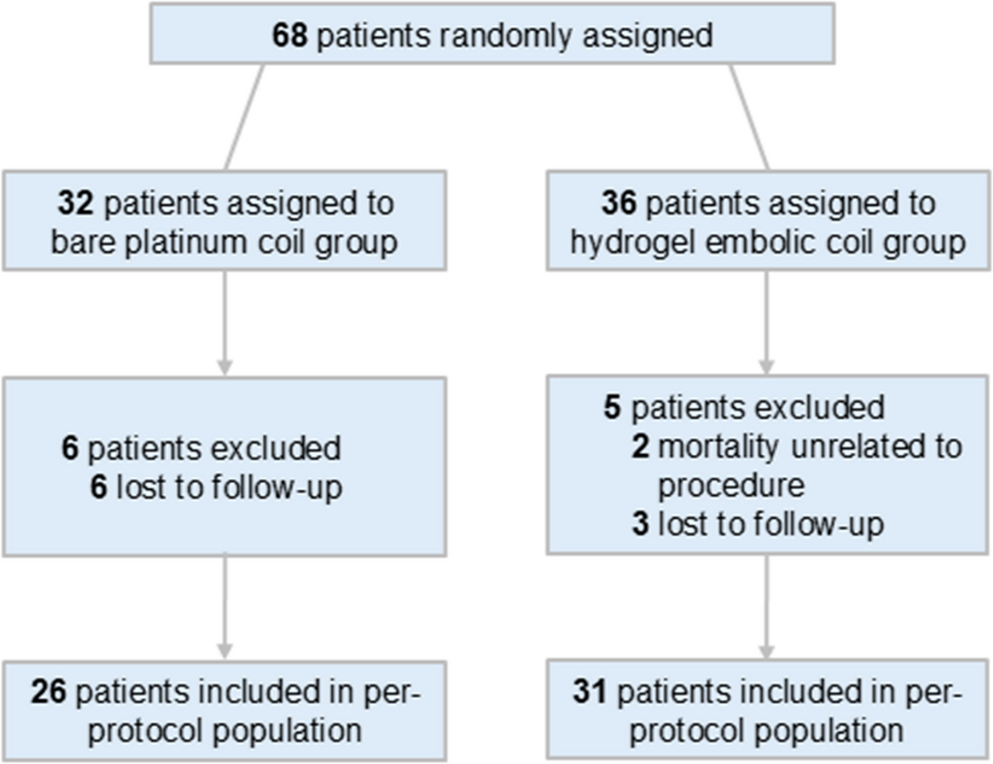
This study has several limitations. First, although the multivariate analysis revealed that HEC had no effect on preventing recurrence in patients with an RIA, the main limitation of this study is that it is underpowered (64%) because of an insufficient sample size, having reached only 57.6% of the planned sample size for the reasons discussed earlier. Owing to the insufficient sample size and limited statistical power, the possibility of a false-negative result cannot be excluded. Although a true difference between the HEC and BPC groups may exist, the present study may have failed to detect such a difference. Therefore, the findings should be interpreted with caution. Additional studies with larger sample sizes are needed to validate the study results. Second, to ensure procedural convenience and safety, the HEC group was not defined as a group treated with 100% HEC, which may have limited the ability to comprehensively assess the true effect of HEC. Third, the primary and secondary outcomes of this study were self-assessed by the treating investigators. The radiological outcomes were not assessed by an independent, blinded core laboratory, and the clinical outcomes were not evaluated by an independent clinical events committee. Therefore, the possibility of potential bias in outcome assessment cannot be ruled out. Finally, the 12-month follow-up period is relatively short compared with other studies, thus limiting the ability to assess long-term outcomes on the basis of the results of this study.

Comments (0)