
Remember me
Among the 88 consecutive patients treated with GKRS during the study period, 60 were diagnosed before 18 years of age and 28 at 18 years or older. Based on the age at the time of Gamma Knife radiosurgery (GKRS), 50 patients received treatment during childhood and 38 during adulthood.
Patients were classified into pediatric (< 18 years) and adult (≥ 18 years) groups based on age at diagnosis. All subgroup analyses, including survival analyses, were performed according to this classification. Patient characteristics by diagnostic age are presented in Table 1.
The median age at GKRS was 15 years (range, 3–55), with a median of 11 years (3–29) in the pediatric group and 28 years (20–55) in the adult group. Across the cohort, 56 patients (63.6%) had undergone subtotal resection (STR), 21 (23.9%) gross total resection (GTR), and 11 (12.5%) biopsies. GKRS was performed as a salvage treatment in 70% of cases.
Table 1 Baseline characteristics according to age at diagnosisDetails of GKRSGKRS was delivered in a single fraction in all cohort. The median treatment volume was 2.7 cm³ (range, 1–9.3), the median prescribed dose was 12 Gy (8–15), the median prescription isodose line was 50% (40–60), and the median maximum dose was 24 Gy (16–44). Treatment parameters by age group are summarized in Table 2.
Table 2 Details of treatment parametersSurvival OutcomesAmong the 88 treated patients, recurrence patterns were evaluated in 84 patients with available follow-up data, median follow-up was 36 (6-207) months. Of these, 57 were pediatric and 27 were adults. Following GKRS, the cumulative incidence of recurrence was 15.5%, with recurrence observed in 5.2% of patients at 1 year and 11.6% at 2 years. In the pediatric cohort, the 1-year and 2-year recurrence rates were 5.8% and 10.8%, respectively, whereas in the adult cohort, the recurrence rates were 4.0% and 13.1% (P = 0.802). All patients were alive at the time of the last follow-up. In the overall cohort, the median progression-free survival (PFS) was not reached; the 5-year and 10-year PFS rates were 83.6% and 71.2%, respectively (Figure 1A). In the pediatric subgroup, the 5- and 10-year PFS rates were 84.7% and 66.7%, whereas in the adult subgroup, they were 81.7% and 81.7%, respectively (Figure 1B).
Fig. 1
Kaplan–Meier progression-free survival (PFS) curves following Gamma Knife radiosurgery. (A) In the overall cohort, (B) Pediatric and adult subgroups
Univariate regression analysis was performed to identify predictors of recurrence following GKRS, including age, neurological deficit, treatment volume, initial surgical approach, indication for GKRS, tumor type, tumor location, and history of prior radiotherapy (RT) or chemotherapy (CT) in the entire cohort as well as in the pediatric and adult subgroups. Detailed results of the univariate and multivariate analyses are presented in Table 3.
Table 3 Univariate and Multivariate Analysis OutcomesIn the entire cohort, pre-GKRS neurological deficit and prior RT were identified as significant factors in the univariate analysis, whereas tumor location and prior CT showed borderline significance. All of these variables were included in the multivariate model. Multivariate analysis demonstrated that a history of prior RT was the only independent predictor of recurrence after GKRS. In the pediatric subgroup, multivariate analysis revealed that cystic/mixed tumor morphology and prior RT were associated with an increased risk of recurrence. In contrast, no variable reached statistical significance as a predictor of recurrence in the adult subgroup.
In the overall cohort, the median PFS was 24 months in patients who had received prior radiotherapy (RT), whereas the median PFS was not reached in those without prior RT. The 1-year recurrence rates were 22.2% and 2.9%, and the 2-year recurrence rates were 53.3% and 6.6% in patients with and without prior RT, respectively (Fig. 2).
Fig. 2
Kaplan–Meier progression-free survival (PFS) curves for the entire cohort, stratified by history of prior radiotherapy
In the pediatric subgroup, the PFS curves stratified by prior RT status and by tumor type are presented in Fig. 3. Among patients who had received prior RT, the 1- and 2-year recurrence incidences were 28.6% and 64.3%, whereas in those without prior RT, the recurrence incidence during the first two years was 2.2%. For patients with cystic/mixed tumor morphology, the 1- and 2-year recurrence incidences were 11.1% and 15.5%, while in those with solid tumors, the recurrence incidence in the first two years was 4.5%.
Fig. 3
Kaplan–Meier progression-free survival (PFS) curves for the pediatric subgroup: (A) comparison based on prior radiotherapy status; (B) comparison according to tumor morphology (solid vs. cystic/mixed)
Prophylactic corticosteroids were administered at the time of GKRS. All patients were discharged on the same day following treatment. No acute treatment-related complications were observed during the first three months of follow-up. No patients required surgical intervention or hospitalization for treatment-related adverse effects.
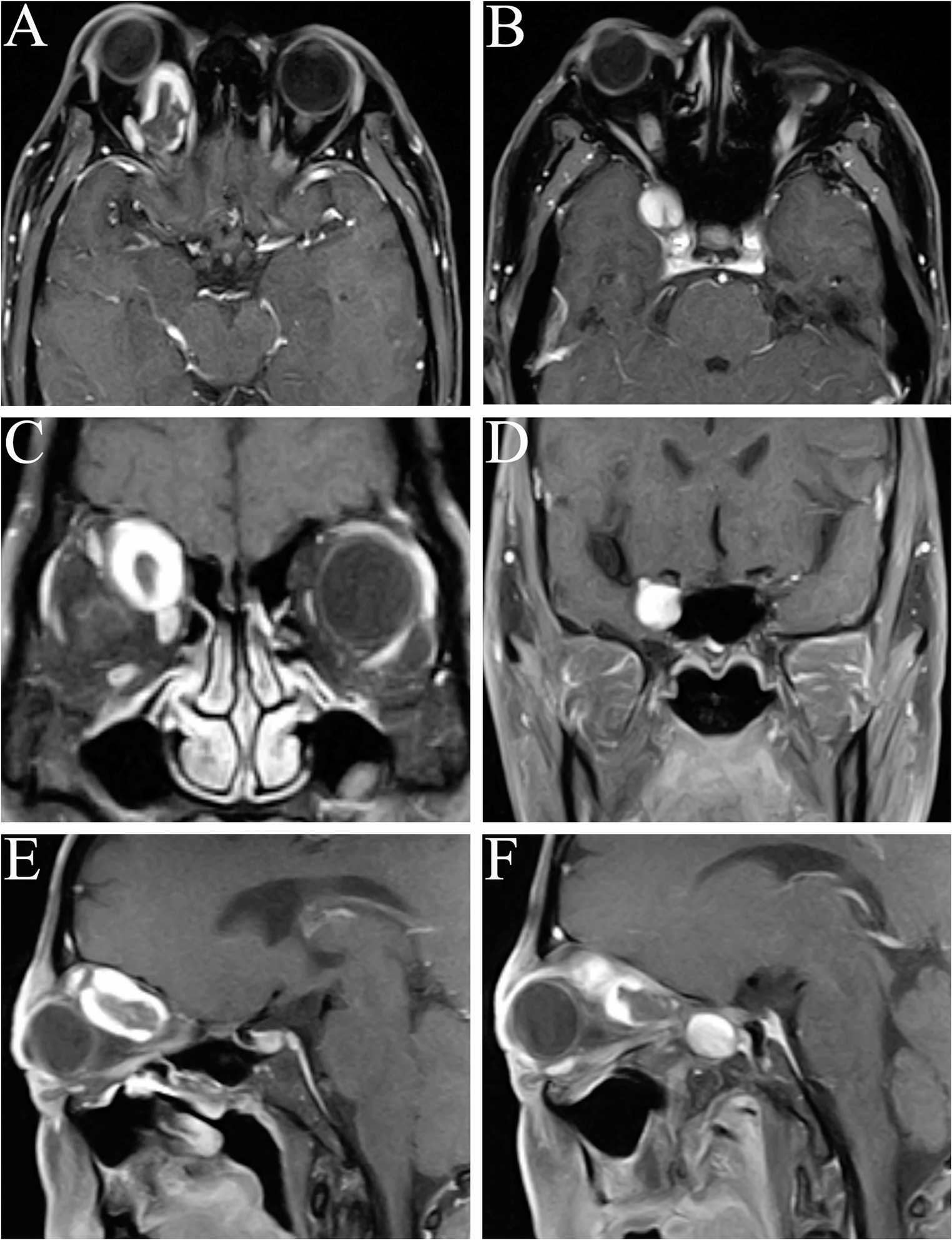
Radiological outcomesDuring median follow-up, 31 patients (36.9%) had no evidence of disease (CR) (Fig. 4), 15 patients (17.9%) showed partial response, 25 patients (29.8%) had stable disease, and 13 patients (15.5%) demonstrated progression in entire cohort. In the pediatric subgroup, 29 patients achieved CR, 8 had a partial response, 11 had stable disease, and 9 showed progression. In the adult group, 2 patients achieved CR, 7 had a partial response, 14 had stable disease, and 4 demonstrated disease progression.
Fig. 4
Gamma Knife radiosurgery dose planning and serial MRI follow-up of pilocytic astrocytoma
These findings are consistent with the largest multicenter retrospective series published by Murphy et al. which analyzed 141 patients treated between 1990 and 2016, the 5- and 10-year PFS rates were reported as 74% and 69.7%, respectively [9]. The median age at GKRS in that cohort was 14 years. In the univariate analysis, age < 18 years, tumor volume < 4.5 cm³, and absence of prior RT or chemotherapy were identified as positive prognostic factors, whereas in the multivariate analysis, only prior RT remained a negative prognostic factor for PFS. Patients without prior radiotherapy demonstrated significantly better PFS rates at 1, 3, 5, and 10 years (92.3%, 85.7%, 78.8%, and 73.8%, respectively) compared to those who had undergone prior radiotherapy (76.2%, 54.4%, 48.4%, and 48.4%, respectively; p = 0.001). Similarly, in our study, prior RT was also identified as the only significant prognostic factor in the multivariate analysis. Among patients without a history of radiotherapy, the 1-, 3-, 5-, and 10-year PFS rates were 97.1%, 91.4%, 88%, and 72.6%, respectively, whereas in those who had received prior RT, the corresponding rates were 77.8%, 46.7%, 46.7%, and 23.3%. These findings are consistent with those reported in the largest multicenter series. It should be noted that the multicenter cohort reported by Murphy et al. likely includes patients from institutions previously represented in earlier single-center publications, including the cohorts described by Kano et al. Therefore, partial overlap between these datasets may exist. These studies are cited to provide historical and contextual comparison rather than to imply entirely independent patient populations.
Kano et al. reported outcomes of SRS for both pediatric and adult patients with pilocytic astrocytoma by analyzing these two cohorts separately [4, 8]. In their pediatric series of 50 patients who underwent SRS, the progression-free survival (PFS) rates for the entire cohort were 91.7%, 82.8%, and 70.8% at 1, 3, and 5 years, respectively [8]. In this study, univariate analysis demonstrated that newly diagnosed or residual tumor (p = 0.049), solid tumor morphology (p < 0.0001), tumor volume < 8 cc (p = 0.001), and absence of brainstem involvement (p = 0.009) were associated with improved PFS. Although prior RT (p = 0.175) did not show a significant effect on PFS, multivariate analysis results were not available. In comparison, in the pediatric subgroup of our series, the 1-, 3-, and 5-year PFS rates were 94.2%, 89.2%, and 84.7%, respectively. Furthermore, based on our multivariate analysis—which provided stronger statistical evidence—we found that absence of prior RT and solid tumor morphology were both significantly associated with improved PFS in pediatric patients.
Prior radiotherapy may represent an adverse prognostic factor for progression-free survival for several reasons. Patients who have previously received radiotherapy often have gross residual disease or recurrent tumors, indicating a more advanced disease course; consequently, Gamma Knife radiosurgery in these cases is frequently applied at a later stage, such as a second recurrence, which may be associated with inferior outcomes compared with treatment at first recurrence. In addition, prior irradiation may select for radioresistant tumor cell populations, further reducing the effectiveness of subsequent radiosurgical treatment. From a technical standpoint, when GKRS is delivered as a second course of radiation, prescription doses may be deliberately reduced to limit cumulative radiation toxicity, potentially compromising local tumor control.
In Kano et al.’s retrospective adult cohort, which included 14 patients, the 1-, 3-, and 5-year PFS rates were 83.9%, 31.5%, and 31.5%, respectively [4]. Although prior surgery was associated with improved PFS, no other significant prognostic factors were identified In our study, among 27 adults with available follow-up data, the 1-, 3-, and 5-year PFS rates were 96.4%, 81.7%, and 81.7%, respectively. In univariate analysis, neurological deficit, age, and brainstem location approached statistical significance; however, none remained significant in multivariate analysis. The adult subgroup analysis may be underpowered due to the limited number of patients and progression events, and these findings should therefore be interpreted with caution. Additionally, differences in baseline tumor characteristics may partly account for the observed variation in outcomes between studies. Notably, the proportion of patients with solid tumor morphology was 35.7% in the study by Kano et al., compared with 55.5% in our series. This difference in tumor morphology distribution may have contributed to differences in PFS; however, given the limited sample size, definitive conclusions cannot be drawn.
More recently, Wei et al. reported a 2023 retrospective analysis of 44 patients who underwent SRS for infratentorial pilocytic astrocytoma [11]. PFS rates were 95.4%, 79.0%, and 61.4% at 1, 5, and 10 years, respectively. In our study, 70.4% of patients had infratentorial tumors, and our corresponding PFS rates of 94.8%, 83.6%, and 59.3% were highly comparable to their findings, further supporting the effectiveness of GKRS in this subgroup.
Despite representing one of the largest single-center series in the literature, this study has several inherent limitations. The median follow-up duration of 36 months may not be sufficient to fully capture very late recurrences or delayed treatment-related effects, particularly in a predominantly pediatric and young adult population. Longer follow-up is therefore necessary to better define durable tumor control and long-term safety outcomes. The retrospective design limits the completeness and uniformity of long-term clinical and neurological outcome assessment. Although no acute treatment-related toxicity or symptomatic radionecrosis was observed, systematic long-term evaluation of neurocognitive and endocrine outcomes was not uniformly available in this cohort. Given the predominantly pediatric population, this represents an important limitation and highlights the need for prospective studies incorporating standardized functional outcome assessments. Given the exploratory nature of the subgroup analyses and the limited number of events, results should be interpreted cautiously, particularly in subgroup comparisons. Another limitation of this study is the lack of systematic molecular profiling according to current WHO classification standards, including BRAF fusion status. As many patients were treated before the routine incorporation of molecular diagnostics into standard practice, molecular subtype could not be evaluated as a prognostic or predictive factor. Future prospective studies integrating molecular characteristics with radiosurgical outcomes are warranted to better define biological predictors of treatment response. Nevertheless, the relatively large cohort size and the use of standardized survival methodology provide clinically meaningful data that contribute to the existing literature on Gamma Knife radiosurgery for pilocytic astrocytoma.
Comments (0)