
Remember me


Patellofemoral malalignment in the transverse plane can lead to increased contact forces between the patella and the femoral trochlea during knee extension and flexion, which can result in accelerated articular cartilage loss and OA. In most cases, there are greater laterally directed forces on the patella, leading to lateral patellar maltracking, lateral patellar facet overload, and lateral-predominant chondral loss. Patellofemoral maltracking is generally multifactorial, often occurring through a combination of osteoarticular factors, such as trochlear dysplasia, and soft tissue conditions, such as a strong, laterally directed force by the vastus lateralis muscle, or medial patellar retinacular insufficiency. Associated imaging findings include lateral patellar tilt, lateral patellar subluxation, or a combination of both.
Patellar tiltPatellar tilt represents a laterally directed rotational torque on the patella in the axial plane that results from lateral patellar retinacular stiffness and/or medial patellar ligamentous insufficiency. Abnormal lateral patellar tilt without subluxation is a defining feature of excessive lateral pressure syndrome, which is a common cause of anterior knee pain [15]. Patellar tilt is commonly measured by one of two angles, the lateral patellofemoral angle or the lateral patellar inclination angle, and it is best quantitatively assessed on either axial patellofemoral radiographs or axial MRI.
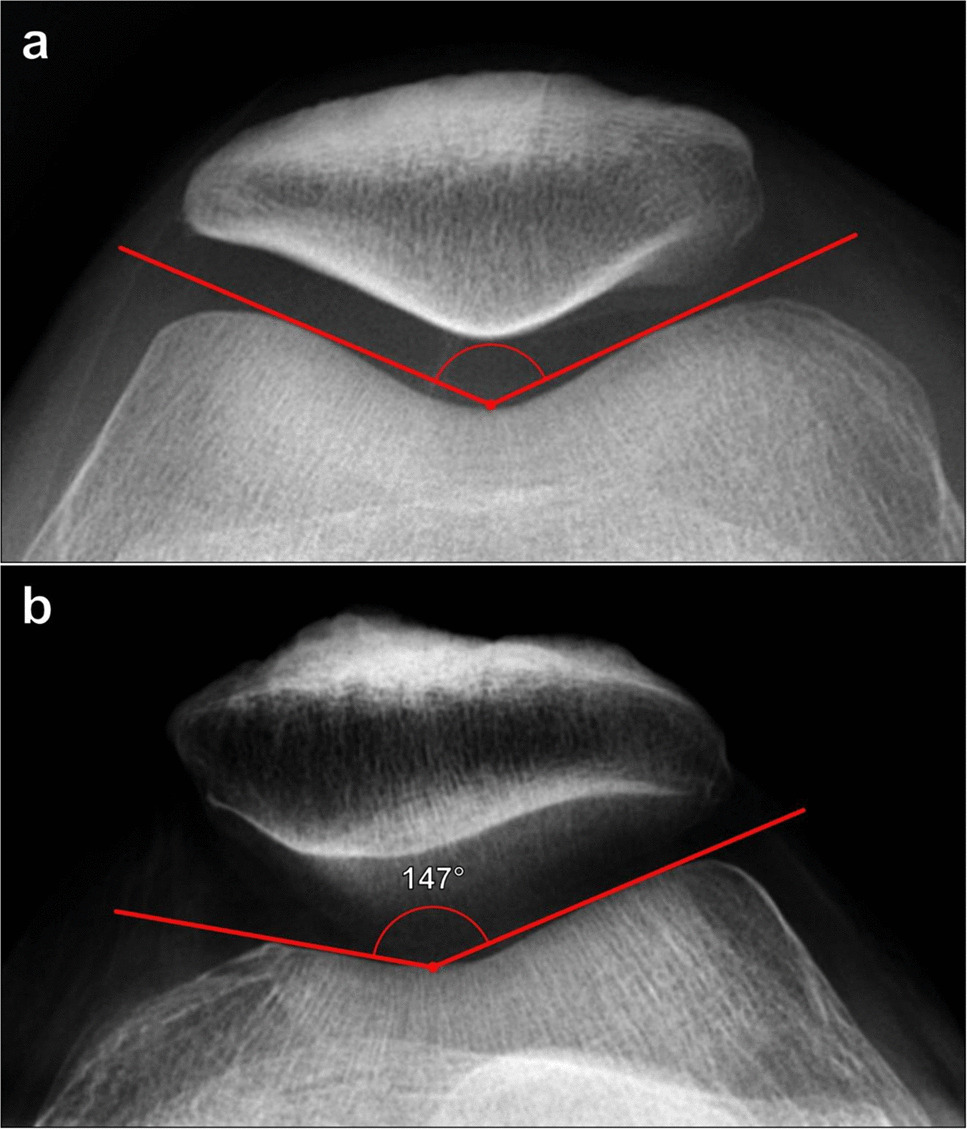
Lateral patellofemoral angle (of Laurin)This angle is formed from two lines on axial knee radiographs (Fig. 8). Initially, it was described on the skyline view but is more commonly currently performed on a Merchant view. The first line connects the anterior margins of the femoral condyles, while the second line extends from the patellar median ridge along the lateral patellar facet [16]. The angle should open laterally (indicated by a value > 0°) and typically measures ≥ 8° [17]. A measurement of < 8°, including negative values, which indicate the angle opens medially, is considered abnormal [15, 16]. The lateral patellofemoral angle can also be measured as described above on cross-sectional imaging at the level of the mid patella. Grelsamer et al. and Wittstein et al. described measurements of the lateral patellofemoral angle in which the femoral condylar line is drawn tangent to the posterior femoral condyles rather than the anterior femoral condyles [17, 18], which are more similar to the physical examination.
Fig. 8
Measurement of lateral patellofemoral angle on Merchant radiograph of the knee. a The angle is measured between a line (A, blue line) drawn connecting the anterior margins of the femoral condyles and a line (B, red line) extending from the patellar median ridge along the posterior margin of the lateral facet. The angle should open laterally, and values < 8° or medially opening angles indicate abnormal lateral patellar tilt. b In a 25-year-old female patient with anterior knee pain, the angle measures −2°, indicating a medially opening angle and lateral patellar tilting
Patellar inclination angle/patellar tilt angleThe second measurement used to determine excessive lateral patellar tilt is the patellar inclination/patellar tilt angle, which is measured on a Merchant knee radiograph (Fig. 9). The angle is formed by one line connecting the anterior margins of the femoral condyles and a second line connecting the medial edge of the medial patellar facet and the lateral edge of the lateral patellar facet. More greatly positive angles indicate progressive medial opening of the angle. The reported normal cutoff value has been variable. The vast majority of normal knees have a patellar tilt angle of < 15°, and initially, a patellar tilt angle of > 20° on radiography was considered abnormal [5]. However, more recently, values > 7°–10° have been utilized as cutoffs to detect excessive lateral patellar tilt.
Fig. 9
Measurement of the patellar inclination/patellar tilt angle on Merchant radiograph of the knee. a The angle is formed between a line (A, blue line) connecting the anterior margins of the femoral condyles and a line (B, red line) between the medial margin of the medial patellar facet and the lateral margin of the lateral patellar facet. A patellar tilt angle of > 7°–10° on radiography is considered abnormal, while an angle of > 10° on CT or MRI is considered abnormal. b In the same patient for Fig. 8a, the patellar tilt angle measures 18°, indicating excessive lateral patellar tilting
The patellar inclination/patellar tilt angle can also be estimated on cross-sectional imaging by using a line connecting the posterior femoral condylar margins and a line connecting the medial and lateral patellar borders at the mid patella where the patella is widest, which helps to improve measurement standardization [18]. Grelsamer et al. described the MRI patellar inclination/patellar tilt angle, with an upper limit of normal of 10°; several asymptomatic patients demonstrated angles of around 10°, so utilizing this cutoff captures essentially all cases of abnormal patellar tilt but would also include patients for whom the measurement does not correlate to clinically significant findings [18]. Thus, utilizing a higher cutoff for the patellar tilt angle on cross-sectional imaging may help to better distinguish normal knees from those with clinically relevant abnormal patellar tilt.
Patellar subluxationPatellar subluxation reflects a linear translation of the patella with respect to the femoral trochlea in the axial plane rather than rotational malalignment. It is best assessed on axial radiographs with the knee flexed between 30° and 45°. Similar to patellar tilt, this commonly occurs laterally due to disproportionate tightness of static lateral stabilizers and greater force by dynamic lateral stabilizers, such as the vastus lateralis muscle. The relative position of the patella compared with the femoral trochlea can be assessed by either angular measurements, such as the congruence angle, or linear measurements, like lateral patellar displacement distance, and angular and linear measurements offer complementary information.
Congruence angleThe congruence angle, initially described by Merchant et al., evaluates the relationship between the patellar median ridge and the deepest part of the trochlear groove. It is measured on an axial view of the knee, either a Merchant radiograph or on cross-sectional imaging at the mid-patellar level (Fig. 10). To measure the congruence angle, initially, the trochlear sulcus angle is measured as previously described. A line bisecting the trochlear sulcus angle is drawn, and the congruence angle is formed between this line and a second line extending anteriorly from the deepest part of the trochlear sulcus (the apex of the sulcus angle) through the crest of the patellar median ridge. If the crest of the patellar median ridge is lateral to the trochlear sulcus, the angle is positive, and if the patellar median ridge is medial to the trochlear sulcus, the angle is negative. The congruence angle is considered abnormal, indicating lateral subluxation of the patella, if it measures > 16° [19].
Fig. 10
Measurement of the congruence angle on Merchant radiograph of the knee. The angle is formed between a line (A) bisecting the trochlear sulcus angle and a line (B) through the crest of the patellar median ridge
Lateral patellar displacementLateral patellar displacement measures the linear distance in the axial plane between the medial margins of the patella and medial trochlear facet (Fig. 11). On the Merchant knee radiograph, a line connecting the anterior margins of the femoral condyles should be drawn. Two lines are then drawn perpendicular to the anterior condylar line: one line along the medial border of the patella and the other through the anterior margin of the medial femoral condyle [16].
Fig. 11
Measurement of lateral patellar displacement on Merchant radiograph of the knee. Lines are drawn perpendicular to the anterior condylar line (A, blue line) at the apex of the medial femoral condyle (B) and along the medial margin of the patella (C). The distance between these lines is the lateral patellar displacement. The most commonly reported normal value is < 5 mm
This measurement can also be assessed on cross-sectional imaging. However, it requires the creation of reference lines on multiple axial images. The initial transverse reference line is taken by forming a line connecting the posterior margins of the femoral condyles. Then, as previously described, two lines perpendicular to the posterior femoral condylar line are drawn: a line intersecting the anterior margin of the medial femoral condyle and a line extending along the medial patellar margin. The patellar displacement is the distance between the two perpendicular lines. The published normal values range from ≤ 2 to < 7 mm, and many authors cite a normal cutoff of < 5 mm. CT and MRI offer better reproducibility due to standardized slice orientation; however, there may be slight differences in measured values between axial radiographs, which are performed with the knee in mild flexion, and cross-sectional imaging, which is commonly performed with the knee extended.
Patellar heightThe patellar height represents the distance between the patella and the tibial tuberosity. The patella serves as a fulcrum for the extensor mechanism and can affect the force generated by the quadriceps musculature during knee extension. There is an optimal patellar height that allows the patella to engage the femoral trochlea throughout its range of motion and to generate maximal power without resulting in pathology, including patellofemoral OA. Patella alta occurs when the patellar height is increased, which can lead to patellofemoral instability and maltracking, while patella baja occurs when the patellar tendon is shortened, which can lead to decreased force generation during extension and decreased range of motion. There are several commonly used methods to determine patellar height, which are subsequently described. In practice, these methods are largely equivalent and may be more common based on regional preferences. These indices are assessed on true lateral knee radiographs with the knee in 30° of flexion to allow consistency and reproducibility, and they are not interchangeable. Additionally, sagittal MRI through the intercondylar region and patellar tendon can be used to assess patellar height and may provide results similar to radiography. However, because the knee is usually imaged in terminal extension on MRI, which can result in patellar tendon laxity, caution should be used to ensure the patellar tendon is taut before measuring these indices [20].
Insall–Salvati indexThis is the most commonly used method for measuring patellar height. Because it does not depend on the degree of knee flexion, it is thought to measure the relative length of the patellar tendon the most accurately [21]. Measured on lateral knee radiographs, the Insall–Salvati ratio compares the length of the patellar tendon along its deep border from the patellar attachment to the tendon insertion on the tibial tuberosity and the maximal patellar length (Fig. 12). The patellar tendon length is divided by the patellar length, and the normal range of values is 0.8–1.3. Calculated values > 1.3 indicate patella alta, while those < 0.8 indicate patella baja [22]. On MRI, different thresholds are used, with normal ranging from 0.74 to 1.5 [23].
Fig. 12
Measurement of the Insall–Salvati index on lateral knee radiograph. a The ratio is calculated as the maximal patellar tendon length (B, red line) divided by the maximal patellar length (A, blue line). The range of normal values is 0.8–1.3. A measured ratio of > 1.3 reflects patella alta, while a ratio < 0.8 indicates patella baja. b Patella alta in a 37-year-old female with anterior knee pain. The Insall–Salvati index measures 1.4, which is mildly increased
It should be noted that this method of assessing patellar height is very sensitive to patellar and tibial tuberosity morphology. The lower pole of the patella can often be developmentally elongated even though the articular surface remains relatively unchanged, or Osgood–Schlatter disease may result in abnormal morphology of the tibial tuberosity. Additionally, this line does not change after tibial tuberosity distalization. In these cases, different measurement techniques may be required.
Modified Insall–SalvatiIn the case of abnormal patellar morphology, the modified Insall–Salvati ratio, also known as the Grelsamer–Meadows index, may be used (Fig. 13). Measured on lateral knee radiographs, the ratio compares the distance from the inferior margin of the patellar articular surface to the patellar tendon insertion on the tibial tuberosity and the length of the patellar articular surface. Normally, this measures 1.2–2.0, and a ratio of > 2.0 reflects patella alta [24]. In practice, the original and modified Insall–Salvati methods are largely equivalent.
Fig. 13
Measurement of the modified Insall–Salvati index on lateral knee radiograph. a The ratio is calculated as the distance from the inferior margin of the patellar articular surface to the patellar tendon insertion on the tibial tuberosity (B, red line) divided by the length of the patellar articular surface (A, blue line). A modified Insall–Salvati index should measure ≤ 1.2, and a ratio > 2 indicates patella alta. b Patella alta in the same patient as in Fig. 12b. The modified Insall–Salvati index measures 2.3, which is increased
Caton–Deschamps indexThis is thought to be the most accurate diagnostic method for evaluating patellar height because it relies on readily identifiable anatomic landmarks, is not affected by the degree of knee flexion or radiograph quality, and can still be used after distalization of the tibial tubercle [25]. On a lateral radiograph of the knee, the patellar height is measured between the inferior margin of the patellar articular surface and the anterior margin of the tibial articular surface, while the patellar length is measured from the superior to the inferior margin of the patellar articular surface (Fig. 14). The index is the patellar height divided by the patellar articular surface length and normally equals 1. A Caton–Deschamps index of > 1.3 indicates patella alta, while a value of < 0.6 indicates patella baja [26]. This index can be measured on a sagittal MRI or CT reformatted imaging of the knee through the central patellofemoral joint; if the radiologist knows the referring clinician needs to assess patellar height prior to image acquisition, the study should be performed with the knee flexed to about 30° to standardize the measurement technique.
Fig. 14
Measurement of the Caton–Deschamps index on lateral knee radiograph with the knee in 30° of flexion. a The ratio is calculated as the distance from the inferior margin of the patellar articular surface to the anterior margin of the tibial articular surface (B, red line) divided by the length of the patellar articular surface (A, blue line). A Caton–Deschamps index of > 1.3 indicates patella alta, while a value < 0.6 reflects patella baja. b Patella alta in the same patient as in Fig. 12b. The Caton–Deschamps index measures 1.4, which is increased
Less commonly used methods to measure patellar height Blackburne–PeelDescribed in detail in Fig. 15 [27, 28], the Blackburne–Peel ratio is rarely utilized in determining patellar height. Like the previously described methods, it is also assessed on lateral knee radiographs with 30° of knee flexion, although it can also be adapted to sagittal CT reformatted images and MRI. The normal range is 0.5–1.0. This method offers higher interobserver reliability than the Insall–Salvati index, particularly in cases with tibial tuberosity abnormalities, such as traction enthesophytes, or following knee arthroplasty [29].
Fig. 15
Measurement of the Blackburne–Peel ratio on lateral knee radiograph with the knee in 30° of flexion. a First, the length of the patellar articular surface is measured (A). Then, a horizontal line is drawn along the tibial plateau articular surface (C). Finally, a line (B) is made from the inferior border of the patellar articular surface extending and perpendicular to line C. The ratio is calculated as B/A. A normal value is 0.5–1.0, while values > 1.0 suggest patella alta. Limitations of this method include variations in inclination of the tibial plateau and projection angles which produce measurement inaccuracies. This measurement is not commonly used clinically since it shows greater interobserver variability than the other measurements. b Borderline patella alta in the same patient as in Fig. 12b. The Blackburne–Peel index measures 1.0, which is top normal. However, the other three indices clearly suggest patella alta in this patient
Patellotrochlear indexUnlike the above-described methods of patellar height measurement which utilize bony landmarks, the patellotrochlear index measures the actual articular congruence between the patella and distal femur. It is measured on sagittal MRI at the level of the maximal patellar cartilage thickness and calculated as the ratio of the trochlear cartilage overlap to the total length of the patellar cartilage. A ratio of < 0.12–0.28 indicates patella alta, while a ratio > 0.5–0.8 is compatible with patella baja. Proper sagittal slice selection is important to reduce interobserver variability (Fig. 16) [30, 31].
Fig. 16
Measurement of the patellotrochlear index (PTI) on sagittal MR image. Measurement should be performed on the midline sagittal MR section through the patella with the thickest articular cartilage and maximal length of the patellar bone. The ratio is calculated as the length of the trochlear cartilage which overlaps the patellar cartilage (B, red line) divided by the total length of the patellar cartilage (A, blue line). The average ratio is 0.32 with ratios < 0.12–0.28 indicating patella alta. Patella baja was originally defined as a PTI > 0.50; however, newer studies suggest a cutoff of > 0.80
Anterior tibial subluxationAnterior knee instability, usually related to anterior cruciate ligament (ACL) insufficiency, is generally determined clinically rather than on imaging. However, in the setting of more pronounced instability, anterior tibial subluxation with respect to the distal femur can be seen on MRI, which is also known as the MRI anterior drawer sign. To measure the degree of anterior tibial subluxation, a sagittal MR image through the mid-lateral compartment of the knee is used, where the measurement has the highest diagnostic accuracy. Two vertical plumb lines are drawn, one from the posterior lateral femoral condyle subchondral bone plate and the other from the posterior cortex of the lateral tibial plateau (Fig. 17). The measurement has the highest diagnostic accuracy at the lateral femoral condylar level. Typically, the distance between the two lines measures ≤ 5 mm, with greater values associated with ACL tear or laxity [32, 33]; a study by Vahey et al. found anterior subluxation of > 7 mm was highly specific for detecting ACL tears and recommended this as the threshold to determine anterior tibial subluxation [33]. This measurement can also be helpful in serial knee MRI examinations, such as after ACL reconstruction, to determine whether there is progressive anterior instability and graft insufficiency [34].
Fig. 17
Measurement of anterior tibial subluxation on sagittal MR images. a Measurement should be performed on the sagittal MR section through the lateral compartment at the level of the mid-lateral femoral condyle where the diagnostic accuracy is the highest. A plumb line is drawn along the posterior lateral femoral condyle subchondral bone (A, blue line), and a second plumb line is drawn along the posterior lateral tibial plateau cortex (B, red line). The distance between the two lines (C, yellow line) is the degree of tibial subluxation. The value normally measures ≤ 5 mm, and any measurement > 7 mm is consistent with anterior tibial subluxation. b Sagittal proton-density weighted nonfat-suppressed image of the mid-lateral compartment in a 24-year-old male patient with a basketball injury demonstrates anterior tibial subluxation measuring 8–9 mm, consistent with anterior cruciate ligament insufficiency
Tibial tuberosity-trochlear groove distanceWhen the tibial tuberosity is more laterally positioned with respect to the trochlear groove, it may exaggerate lateral patellofemoral forces, increasing the risk for patellofemoral maltracking and accelerated patellofemoral cartilage degeneration. The tibial tuberosity-trochlear groove (TT-TG) distance measures the degree of tibial tuberosity lateral displacement relative to the trochlea and is an important measurement for preoperative planning in patellofemoral realignment; the larger the TT-TG distance, the greater the degree of correction required to reduce lateral forces on the patella. Factors that may contribute to an increased TT-TG distance include femoral anteversion and external tibial torsion [5].
The TT-TG distance is measured on axial cross-sectional images of the knee (Fig. 18). First, a line is drawn tangent to the posterior femoral condyles. Subsequently, two lines are drawn perpendicular to the posterior condylar line: a line through the deepest part of the trochlear sulcus and a line through the most anterior portion of the tibial tuberosity. The distance between line B and line C is the TT-TG distance [5].
Fig. 18
Measurement of the tibial tuberosity-trochlear groove (TT-TG) distance shown schematically and on clinical images. a Diagram depicting the method of assessing the TT-TG distance by superimposing an axial image of the knee through the femoral trochlea located approximately 3 cm above the femorotibial joint line and an axial image through the tibial tuberosity. First, a line connecting the posterior femoral condyles is drawn (solid red line). Then, a perpendicular line to the posterior bicondylar line is drawn on the femoral trochlear image through the deepest part of the trochlear sulcus (orange line). Next, a second line perpendicular to the bifemoral condylar line (yellow line) is drawn on the tibial tuberosity image to the apex of the tibial tuberosity, and the TT-TG distance is the distance between the orange and yellow lines (dashed red line). b On superimposed axial CT images of a 35-year-old male patient, A, solid red line, represents the posterior bicondylar line; B, orange line, is perpendicular to (A) and extends through the deepest part of the trochlear sulcus; and C, yellow line, is the perpendicular line extending through the tibial tuberosity. The TT-TG distance (dashed red line) measures 14 mm. The TT-TG distance normally measures < 15 mm. Values between 15 and 20 mm are considered borderline, while a TT-TG > 20 mm is abnormal
A normal TT-TG distance is < 15 mm, while a TT-TG > 20 mm is abnormal [5]. Values between 15 and 20 mm are considered borderline increased and should be interpreted in combination with additional imaging findings and clinical symptoms. Of note, CT is the gold standard for TT-TG assessment. Although the TT-TG distance can be measured on MRI, the values obtained when using MRI have been shown to underestimate the TT-TG distance by approximately 4 mm when compared to CT [35]. The difference may be due to a few factors, including slight knee flexion on MRI compared to full knee extension on CT, and the inclusion of soft tissue structures, such as articular cartilage and the patellar tendon insertion when making measurements on MRI.
ArthroplastyThe objective of total knee arthroplasty (TKA) is to restore normal anatomy, motion, and stability of the knee. The anterior flange of a correctly sized femoral component should be parallel to and flush against the distal femoral anterior cortex. Oversized components can cause excessive soft tissue tension and decreased range of motion, while undersized components can result in notching of the anterior femoral cortex, which predisposes to periprosthetic supracondylar femoral fracture [36]. The size of the tibial component should qualitatively match the size of the native plateau; an oversized component with overhang may irritate adjacent soft tissues, and undersizing increases the risk of subsidence [37].
Radiographic and cross-sectional assessmentThe minimum radiographic assessment includes properly positioned AP and true lateral radiographs of the knee with the X-ray beam centered at the joint line in order to avoid excessive rotation or joint flexion and avoid beam angle artifact, which can significantly distort angular measurements and obscure subtle signs of loosening or malalignment. Furthermore, baseline radiographs are important to detect early signs of prosthetic migration or wear that may only be visible on serial imaging studies.
When evaluating a classically aligned TKA on an AP radiograph (Fig. 19), the femoral component should be 7° ± 3° valgus to the femoral anatomic axis, and the tibial component should be 90° ± 3° to the tibial anatomic axis [36]. This allows for an overall 4°–7° valgus angulation of the knee using the anatomic axis of the femur and tibia. There has been recent increased interest in utilizing kinematic alignment techniques for TKA placement, in which the arthroplasty is placed with the goal of reestablishing the pre-arthritic alignment of the knee; in these cases, the radiographic alignment of the TKA may fall outside of these classic parameters [38].
Fig. 19
AP radiographic evaluation of a total knee arthroplasty. The tibial component articular surface (B, dashed orange line) is 90° relative to the tibial anatomic axis (A, blue line through the proximal tibia). The femoral component long axis (C, solid red line) is the perpendicular line to the femoral component articular surface (dashed red line). Relative to the femoral anatomic axis (D, yellow line through the distal femur), it should be 7° ± 3° valgus angulation, in a classic arthroplasty alignment. In this example, this angle measures 4°
On lateral knee radiographs (Fig. 20), the horizontal portion of the femoral component should be 90° relative to the anatomic axis of the femur [36]. The articular surface of the tibial component should be 90° relative to the tibial anatomic axis or slope posteriorly 3°–7°, and the post should be either central or posterior to the central tibial shaft [37]. The patellar height is measured along a line extending inferiorly from the inferior margin of the patellar component perpendicular to a line drawn along the tibial articular surface line and should be 10–30 mm [39].
Fig. 20
Lateral radiographic evaluation of a total knee arthroplasty. The tibial component articular surface (B) should be 90° relative to the tibial anatomic axis (A, solid yellow line) or slope posteriorly 3°–7°. The horizontal component of the femoral component (C, dashed red line) should be 90° relative to the femoral anatomic axis (D, solid red line). The patellar height (PH, green line) is measured perpendicular to a line tangent to the tibial articular surface (B, dashed yellow line) and is measured from this line to the inferior edge of the patellar component. The patellar height should measure 10–30 mm
Rotational alignment of the components is assessed on axial cross-sectional CT images (Figs. 21 and 22). The femoral component should be slightly internally rotated relative to the transcondylar axis. This is measured as the angle between a line drawn from the peak of the lateral epicondyle to the sulcus of the medial epicondyle (surgical femoral epicondylar axis) and a line connecting the posterior prosthetic medial and lateral condylar surfaces (Figs. 21a and 22a). Normal values are 0.3° ± 1.2° in women and 3.5° ± 1.2° in men [40]. The tibial component should be internally rotated approximately 18° ± 2.6° relative to the tibial tubercle. This is measured as the angle between a line bisecting the tibial tubercle through its center point and a line perpendicular to the posterior tibial component at the level of the polyethylene liner (Figs. 21b and 22b) [40].
Fig. 21
Comments (0)