
Remember me


In the following section, we delineate the main clinical entities that exemplify ON in elite athletes. The overview is restricted to the most prevalent anatomical sites and lesion patterns, which represent the entities most commonly encountered in clinical practice. This list is furthermore summarized in Table 1.
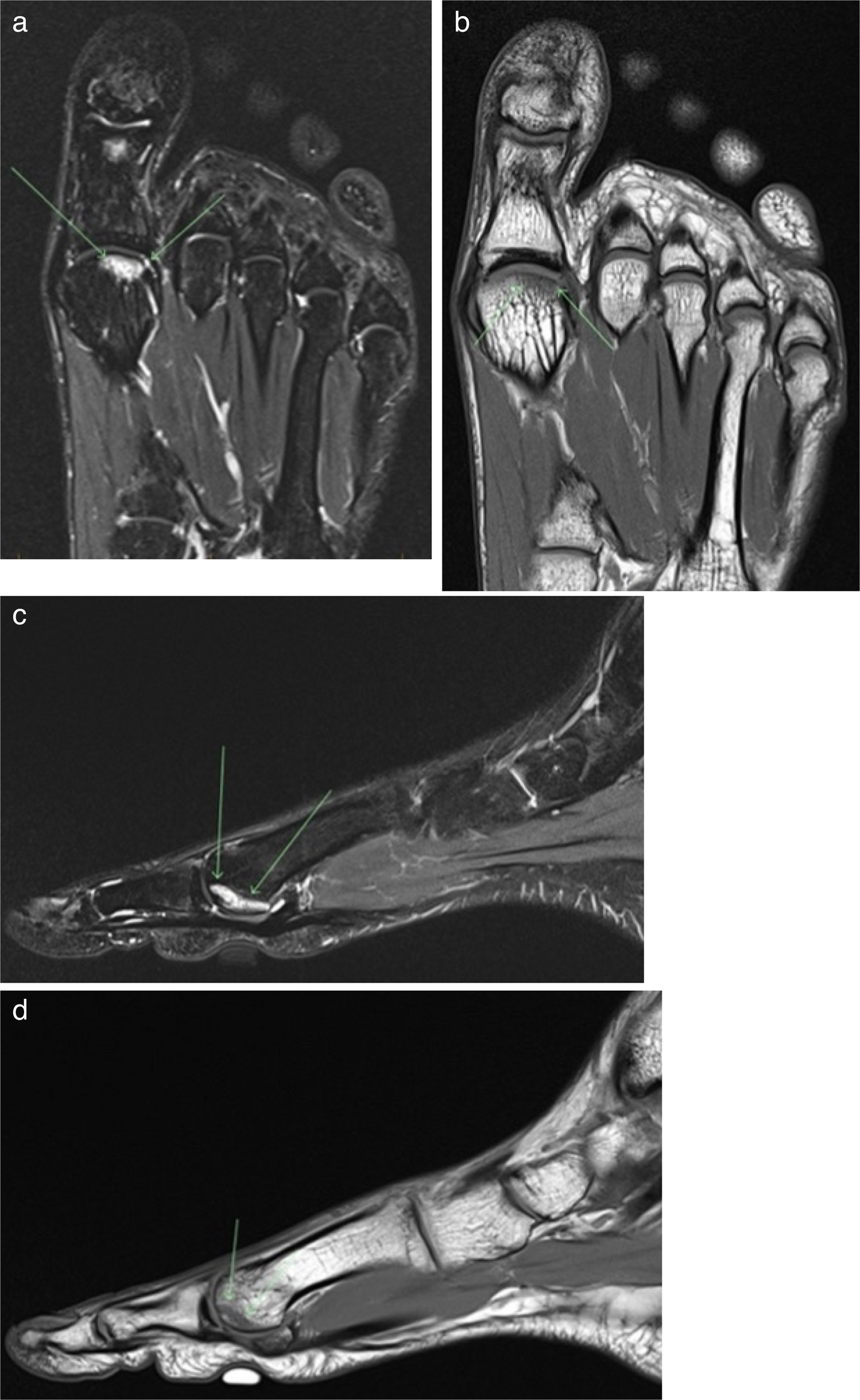
Table 1 Site-specific manifestations of osteonecrosis and related stress/insufficiency lesions in elite athletes. The table distinguishes primary epiphyseal osteonecrosis (e.g., femoral head, talus, humeral head, and carpal bones), subchondral insufficiency fractures with secondary osteonecrosis (knee: medial femoral condyle, SIFK) and metaphyseal/diaphyseal medullary bone infarcts. Radiological findings for the knee row refer to subchondral insufficiency fracture of the knee (SIFK) with secondary osteonecrosis, whereas the final row describes medullary bone infarcts rather than epiphyseal ONFreiberg’s diseaseFreiberg’s disease, or Freiberg infraction, is a form of ON that most commonly affects the second metatarsal head in young, adolescent female athletes. Athletes most at risk are adolescent girls and young women involved in running, jumping, and dance-based sports where repetitive forefoot loading and a relatively long second metatarsal increase local stress on the metatarsal head [27, 29, 30]. It serves as a well-documented example of how repetitive mechanical stress can lead to bone ischemia. The two primary etiological theories are repetitive microtrauma and vascular compromise. The traumatic theory posits that constant, high-impact activities like running, jumping, and dancing cause multiple tiny fractures to the metatarsal’s growth plate, which in turn impairs blood flow to the bone head. The vascular theory suggests that anatomical variations, such as an abnormally long second metatarsal, may make the bone more susceptible to microvascular damage (Fig. 1a–d). Clinically, patients present with an insidious onset of a dull, aching pain in the forefoot that worsens over time and is most pronounced during weight-bearing activities. It may also be accompanied by a sensation of “walking on a stone” [27, 29].
Fig. 1
MRI images of a Metatarsal 1 head osteonecrosis. a T2 coronal image of a centrally localized Metatarsal 1 head osteonecrosis. b T1 coronal image of a centrally localized Metatarsal 1 head osteonecrosis. c T2 sagittal image of a plantarly localized Metatarsal 1 head osteonecrosis. d T1 sagittal image of a plantarly localized Metatarsal 1 head osteonecrosis
Management begins with conservative measures, which include rest, activity modification, the use of custom orthotics to redistribute pressure, and immobilization. With early diagnosis and treatment, the prognosis for a favorable outcome and a return to sport is high [30].
Osteonecrosis of the talusAvascular necrosis of the talus (Fig. 2a–d) is another rare but significant condition in the athletic population, often caused by a previous ankle fracture or dislocation. These injuries can disrupt the talus’s precarious blood supply, leading to bone necrosis. Athletes at risk are those participating in sports that expose the ankle to high axial loads and forced extremes of dorsiflexion and plantarflexion, such as basketball, football/soccer, trail running, and gymnastics, and those sustaining high-energy ankle trauma [28, 31]. Clinically, it presents as deep ankle pain that worsens with activity. Management depends on disease stage. Early, precollapse disease may be managed with restricted weight-bearing, bracing, and analgesia; joint-preserving procedures such as core decompression or vascularized bone grafting may be considered. Once talar collapse occurs, surgical options shift to joint-sacrificing procedures, including arthrodesis or total talus replacement [28, 32].
Fig. 2
MRI images of a medial talar osteonecrosis. a T2 axial image of a medial talar osteonecrosis affecting almost the whole anteroposterior medial talar head area. b T2 sagittal image of a medial talar osteonecrosis affecting almost the whole anteroposterior medial talar head area. c T2 coronal image of a medial talar osteonecrosis affecting almost the whole medial talar head area. d T1 coronal image of a medial talar osteonecrosis affecting almost the whole medial talar head area
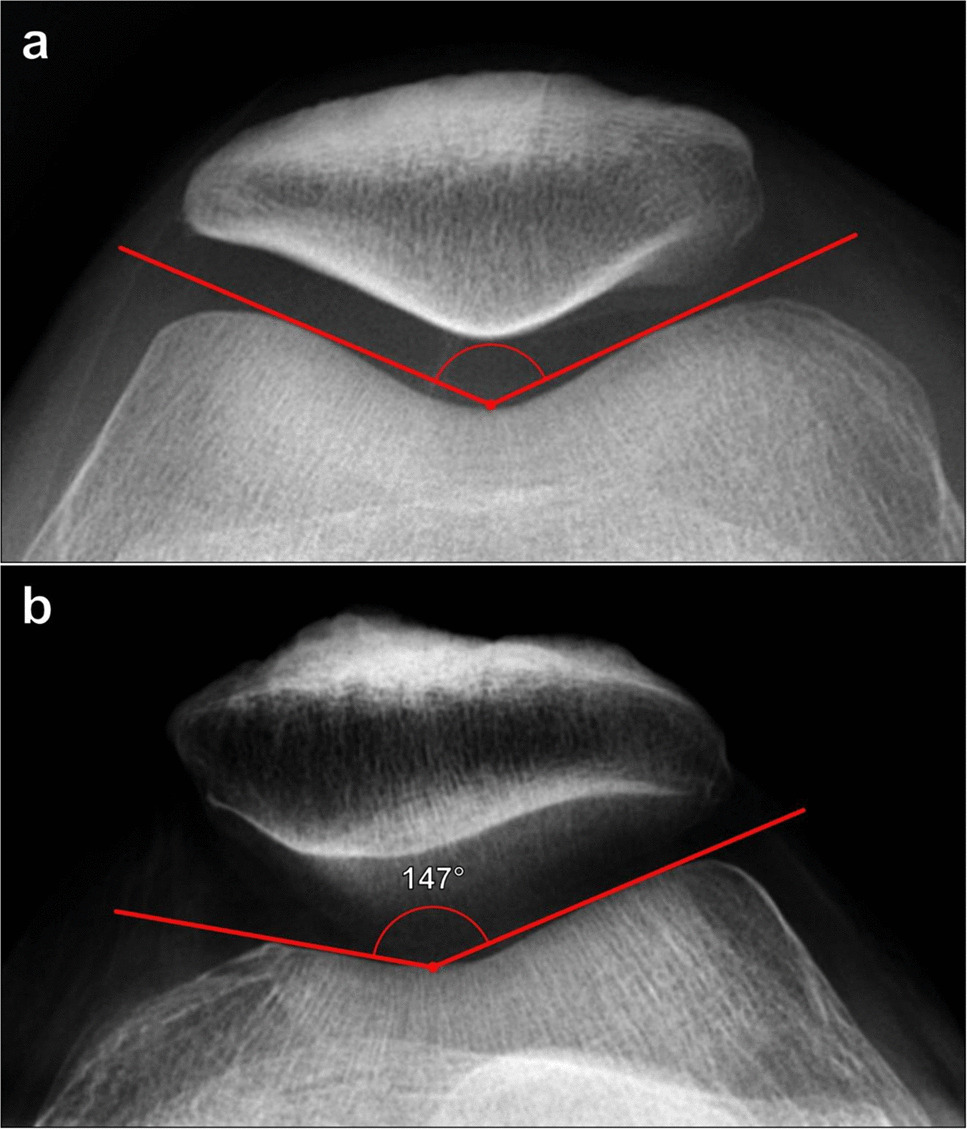
Osteonecrosis of the kneeIn elite and high-demand athletes, osteonecrotic-appearing lesions of the knee are rare but clinically significant, because they typically involve the load-bearing portion of the femoral condyle and can rapidly jeopardize joint function and sports participation [33]. What was formerly known as “spontaneous osteonecrosis of the knee” (SONK) was historically considered a primary, idiopathic ischemic necrosis, most commonly of the medial femoral condyle, with abrupt onset of pain typically in older women [6]. However, the understanding of knee ON has undergone a major paradigm shift: SONK is now regarded as part of the spectrum of subchondral insufficiency fracture of the knee (SIFK), with ON as a secondary phenomenon rather than the primary event [6, 34, 35].
Histological work provided the key turning point. Analysis of surgical specimens demonstrated a subchondral insufficiency fracture with reparative changes and only secondary ON within the overlying fragment, indicating that fracture, rather than primary vascular necrosis, is the initiating lesion [6, 36]. Subsequent radiologic and clinical series have confirmed that most lesions previously labeled SONK sit on the spectrum of SIFK in osteopenic or otherwise weakened bone. The Society of Skeletal Radiology (SSR) now explicitly recommends that the term SONK be abandoned as an etiologic label and replaced by SIFK with or without secondary ON, recognizing SONK as a misnomer for an advanced SIFK lesion [2].
The continued use of the term “spontaneous” in some clinical literature represents a critical disconnect between contemporary research and common clinical practice. This reclassification transforms the perception of the condition from a random, unpreventable vascular catastrophe to a biomechanically driven insufficiency fracture occurring in bone with reduced strength and adverse load distribution, often in the setting of low BMD, varus alignment, or meniscal root tears [20]. Athletes most at risk are older endurance or pivoting athletes with varus-aligned knees or medial meniscus root tears and extrusion [37].
In the athletic setting, this entity should therefore be approached primarily as a stress injury of subchondral bone. Athletes typically report a sudden onset of localized medial knee pain, often after an apparently innocuous training session, game, or change in load [33, 34]. Clinical examination usually reveals focal joint-line tenderness and pain on weight-bearing, while plain radiographs may initially be normal or show only subtle subchondral changes [34, 35]. MRI is the modality of choice, demonstrating a subchondral hypointense band with surrounding bone marrow edema in the affected condyle and allowing early distinction from other causes of knee pain in athletes [6, 34].
This conceptual shift has profound implications for diagnosis and treatment, directing the focus toward addressing underlying bone health and mechanical stressors rather than treating a primary vascular event. For older athletes, recognizing a painful medial femoral condyle lesion as SIFK with secondary ON, rather than idiopathic SONK, shifts management toward early load modification, correction of mechanical risk factors, and optimization of bone health, with the aim of preventing progression to collapse and joint-replacing surgery [20]. For elite athletes in particular, early recognition is critical. If training and competition loads are not appropriately reduced, these lesions can progress to subchondral collapse and secondary osteoarthritis, outcomes that often necessitate joint-preserving surgery or arthroplasty and may be incompatible with continued high-level sport [33, 35]. A high index of suspicion, timely MRI, prompt off-loading, structured rehabilitation, and targeted correction of underlying biomechanical and skeletal risk factors are therefore essential components of management in this population.
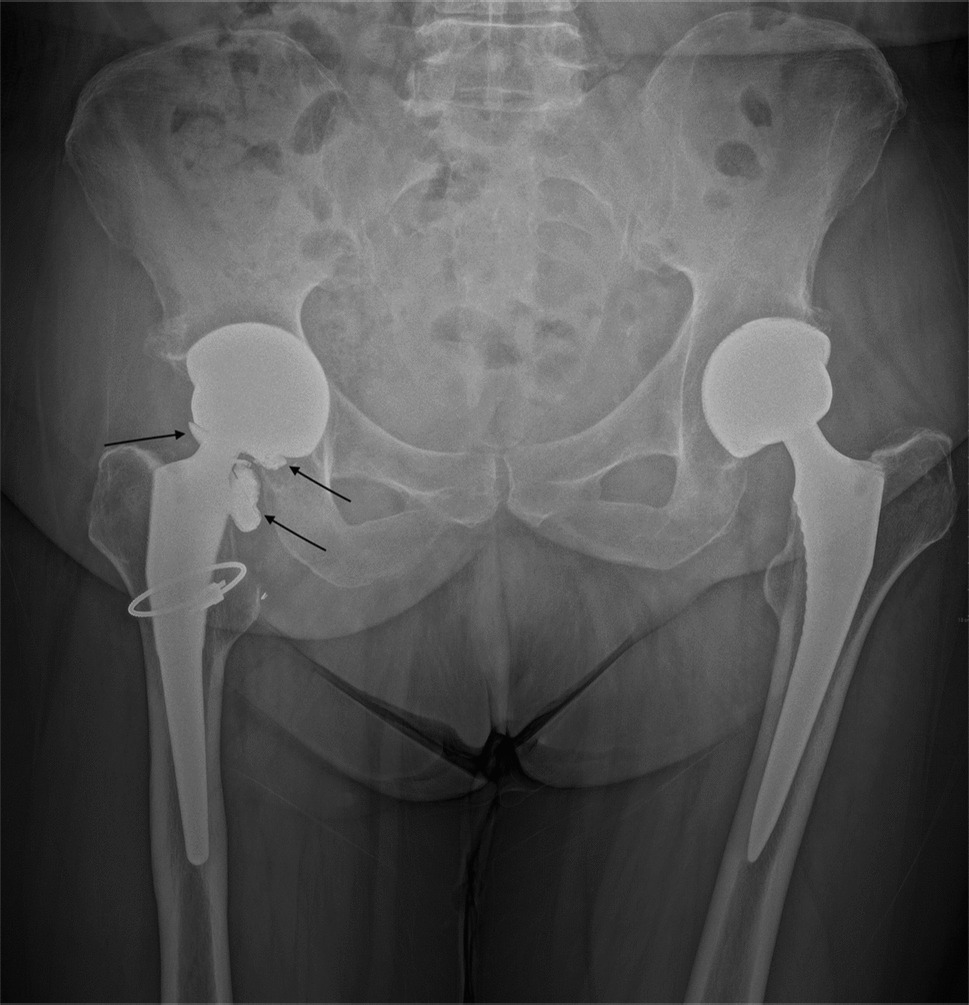
Osteonecrosis of the femoral headOsteonecrosis of the femoral head (ONFH) is the most common and clinically significant form of this disease, accounting for over 35% of all cases [38]. ONFH in the general population is most frequently associated with traumatic dislocation, fracture, long-term systemic corticosteroid use, or dyslipidemias [8, 10, 12, 38]. In the athletic context, both acute traumatic injury and chronic mechanical stress contribute to risk. Athletes at greatest risk include those in collision and high-speed sports (e.g., rugby, American football, ice hockey, and alpine skiing) where hip dislocation or proximal femoral fractures may occur, as well as athletes requiring prolonged high-dose corticosteroid therapy for inflammatory or autoimmune conditions [17, 21, 38].
In addition to these established etiologies, secondary osteonecrosis may develop in association with subchondral insufficiency fracture (SIF) of the femoral head, a mechanism increasingly recognized in highly trained athletes exposed to repetitive high joint loads or abrupt changes in training intensity. Unlike primary ischemic ONFH, SIF represents mechanical failure of the subchondral bone that can secondarily compromise local blood supply, leading to rapid structural collapse [39]. Although traditionally described in older populations, SIF may be underdiagnosed in elite athletes, where continued loading accelerates progression and imaging findings may overlap with traumatic or idiopathic AVN.
Hip-related career-ending injuries often begin with a traumatic hip dislocation sustained during a tackle, underscoring the potentially catastrophic nature of high-energy injuries. Even when promptly reduced, vascular disruption may already have occurred, precipitating ON. For elite athletes, advanced ON and subsequent arthroplasty are generally incompatible with continued participation in high-impact or collision sports. Regardless of whether ONFH arises from trauma, systemic risk factors, or secondary necrosis following SIF, femoral head collapse results in debilitating arthritis, often necessitating total hip replacement and precluding return to high-level athletics [8, 12, 17, 39,40,41,42].
Osteonecrosis of the shoulderON of the humeral head is most commonly associated with proximal humerus fractures and glenohumeral dislocations, systemic corticosteroid therapy and, less frequently, alcohol abuse or hemoglobinopathies [43, 44]. Athletes at particular risk include overhead and throwing athletes (e.g., baseball pitchers, swimmers, volleyball, and tennis players) exposed to repetitive high-load shoulder motion and contact or collision athletes (e.g., rugby, American football, and ice hockey) who sustain glenohumeral dislocations and complex proximal humeral fractures [44]. The clinical presentation is typically a deep, aching pain and can lead to a significant loss of shoulder function. Early stage disease may mimic rotator cuff pathology, making diagnosis challenging. For early stage ON, nonoperative treatment is preferred: activity modification, physical therapy, analgesia, and restricted loading. Joint-preserving surgical options such as core decompression, arthroscopic debridement, and bone grafting may also be considered in persisting or progressing symptoms. In the presence of articular collapse, shoulder arthroplasty is indicated [43, 44].
Osteonecrosis of the carpal bonesAmong the carpal bones, the lunate and scaphoid are the most clinically relevant sites of ON in elite athletes. In this population, both primary lunate ON (Kienböck’s disease) and scaphoid ON may be encountered, either as a complication of fracture or, more rarely, as an idiopathic entity.
In elite athletes, Kienböck’s disease is best understood as ON of a high-demand lunate exposed to repetitive loading. Athletes at risk are those participating in sports with repetitive wrist loading and forceful extension, such as rowing, gymnastics, and racquet or ball sports, where repeated microtrauma is applied to a mechanically disadvantaged lunate [45]. Patients typically present with insidious dorsal wrist pain, loss of grip strength, and reduced range of motion that interferes with performance, and the diagnosis is often delayed because symptoms mimic tendinopathy or “sprain”; MRI is recommended when plain radiographs are normal or equivocal, both to confirm lunate ON and to stage disease [45].
Scaphoid ON in athletes is most commonly secondary to fracture, typically involving the proximal pole. Scaphoid fractures are the most frequent carpal fractures in sport and are classically sustained in fall-on-the-outstretched-hand mechanisms in sports with high fall risk or upper-limb impact (e.g., football, snow- and board-sports, gymnastics, and combat sports). The predominantly retrograde intraosseous blood supply to the proximal pole renders this segment particularly vulnerable to ischemia after displaced waist or proximal pole fractures, delayed diagnosis or persistent loading through an unrecognized nonunion [46]. In elite athletes, pressure to continue competing may further delay diagnosis and definitive stabilization, increasing the risk of nonunion and segmental ON. Clinically, athletes usually report radial-sided wrist pain aggravated by gripping, push-ups, or axial loading in extension and may present late with reduced range of motion and loss of power grip when a chronic nonunion with proximal pole collapse has already developed.
Idiopathic ON of the scaphoid, classically termed Preiser’s disease, is rare but important to recognize. It is defined as progressive necrosis of the scaphoid in the absence of a preceding fracture and is probably multifactorial, with anatomical or biomechanical variations, systemic risk factors, and repetitive microtrauma all proposed as contributors [47]. Patients present with insidious radial-sided wrist pain, stiffness, and diminished grip strength, and in athletes, this may initially be mislabeled as “tendinitis” or overuse. Radiographs may show diffuse sclerosis, cystic change, or fragmentation of the scaphoid; MRI is helpful for confirming the diagnosis, assessing disease stage and delineating the extent of viable bone [47]. While Preiser’s disease is not uniquely sports-related, high repetitive load and forced wrist extension may accelerate symptoms and structural deterioration in athletes whose scaphoid is already “at risk.”
Management of carpal ON in elite athletes remains stage-dependent but must be framed around preserving motion and grip in a professional wrist. Short periods of immobilization, temporary load modification and sport-specific technique adaptations may be reasonable in very early disease. For Kienböck’s disease and early posttraumatic scaphoid ON, joint-leveling procedures, revascularization techniques, and fixation with vascularized bone grafts are often favored in young high-demand patients to restore biology and mechanics and maximize the chance of maintaining a functional motion arc [45, 46]. In idiopathic Preiser’s disease, treatment ranges from immobilization and unloading in early stages to radial or capitate shortening osteotomy, vascularized grafting, or partial wrist fusion when collapse or carpal malalignment develops [47]. Case series in competitive athletes document successful return to multisport participation after joint-preserving procedures once pain has settled and strength has been restored, but salvage options for advanced collapse (proximal row carpectomy, limited or total wrist arthrodesis) are generally considered career-limiting for athletes whose sport relies on high-power wrist function [45].
Diaphyseal/metaphyseal medullary bone infarctsDiaphyseal and metaphyseal medullary BIs are ischemic lesions of the marrow cavity that share many of the same systemic risk factors as epiphyseal ON, including corticosteroid exposure, hemoglobinopathies, and dysbaric disease [3]. They are not strongly sport-specific but may be encountered in divers and caisson workers (including military and commercial divers) exposed to repeated decompression, in whom dysbaric osteonecrosis classically produces multiple metaphyseal infarcts, as well as in athletes requiring high cumulative doses of systemic steroids [48]. In contrast to epiphyseal lesions, most medullary infarcts have limited direct mechanical consequences for joint congruity because they do not primarily involve the subchondral plate; however, their presence in an athletic patient should prompt evaluation for systemic or environmental risk factors and may signal multifocal osteonecrosis elsewhere in the skeleton [3].
Comments (0)