Aging, male sex, and comorbidity with RLS have consistently been identified as independent risk factors for PLMS in community-based studies [18, 19]. Our previous analyses found that although the prevalence of PLMS was higher among men, no statistically significant differences were observed between the sexes. However, we did confirm that the prevalence of PLMS increases with advancing age, and we observed that African ancestry was associated with a reduced risk of PLMS [20].
Building on these findings, the current study further extends our understanding by investigating the association between PLMS prevalence and biochemical markers, offering valuable insights into this complex relationship within the São Paulo population. Some studies have reported an association between ferritin concentrations - a blood protein that stores and releases iron - and PLMS during sleep, but the results remain inconsistent [8, 21]. Notably, low-normal ferritin concentrations (< 50 ng/mL) have been shown to correlate with severe RLS symptoms, emphasizing iron’s potential role in the pathophysiology of these sleep-related movement disorders [22]. In the current study, higher hemoglobin levels were associated with a lower risk of developing PLMS in the EPISONO 2007 sample, with each 1 g/dL increase in hemoglobin corresponding to a reduced likelihood of the condition. When the analysis was stratified by sex, this protective effect was observed only in men. However, in the EPISONO 2018 evaluation, no protective effect was found in the general population or within either sex group. Iron, as a critical component of hemoglobin, facilitates oxygen transport and supports dopaminergic function by serving as a cofactor for tyrosine hydroxylase, the enzyme responsible for dopamine synthesis [15, 23]. Iron deficiency can impair this process, resulting in reduced dopamine production and altered neurotransmission [24], especially within the basal ganglia, a brain region central to motor control. In conditions, such as RLS and PLMS, iron deficiency is often associated with disrupted dopaminergic pathways, which contribute to the characteristic symptoms of these disorders [15, 25].
Studies in both children and adults with sickle cell disease (SCD) have reported an increased rate of PLM during sleep. Mutations linked to SCD produce an abnormal beta-globin subunit, leading to the formation of Hemoglobin S. When deoxygenated, Hemoglobin S causes red blood cells to assume a rigid, sickle shape, which can obstruct the microvasculature and result in ischemia, producing the typical clinical manifestations [26]. In addition to ischemia, oxidative stress and inflammation are closely linked to the pathophysiology of SCD and its related complications [27]. Interestingly, these same features—ischemia, oxidative stress, and inflammation—are associated with elevated Hcy concentrations [28], another risk factor for PLMS identified in this study for the first time.
In the 2007 EPISONO study, a 1 µmol/L increase in Hcy was linked to a 1.09-fold increase in the odds of PLMS in the overall sample. When analyzed by sex, this elevated risk was significant only in men, corresponding to an 8% increase in risk per unit increase in Hcy. Conversely, in the 2018 EPISONO study, Hcy concentrations did not show a statistically significant association with PLMS risk in the overall sample (p = 0.07). However, in sex-specific analyses, each 1 µmol/L rise in Hcy was associated with a 6% increase in PLMS risk among men. Increased Hcy concentrations did not appear to be associated with cobalamin deficiency, as no significant alterations in cobalamin concentrations were observed in either the 2007 or 2018 editions of the EPISONO study. Statistical analyses were controlled for folic acid, another cofactor related to Hcy metabolism [12]. The higher Hcy concentrations observed in men are consistent with previous reports showing elevated levels across age groups, supporting the existence of intrinsic sex-related differences in homocysteine metabolism [29]. Xu and colleagues proposed a plausible biological explanation related to creatine metabolism, as men generally have greater muscle mass, leading to increased demands for creatine synthesis [30]. This process consumes methyl groups derived from S-adenosylmethionine and generates S-adenosylhomocysteine, the immediate precursor of homocysteine [12], which may partially explain the higher circulating Hcy concentrations observed in men.
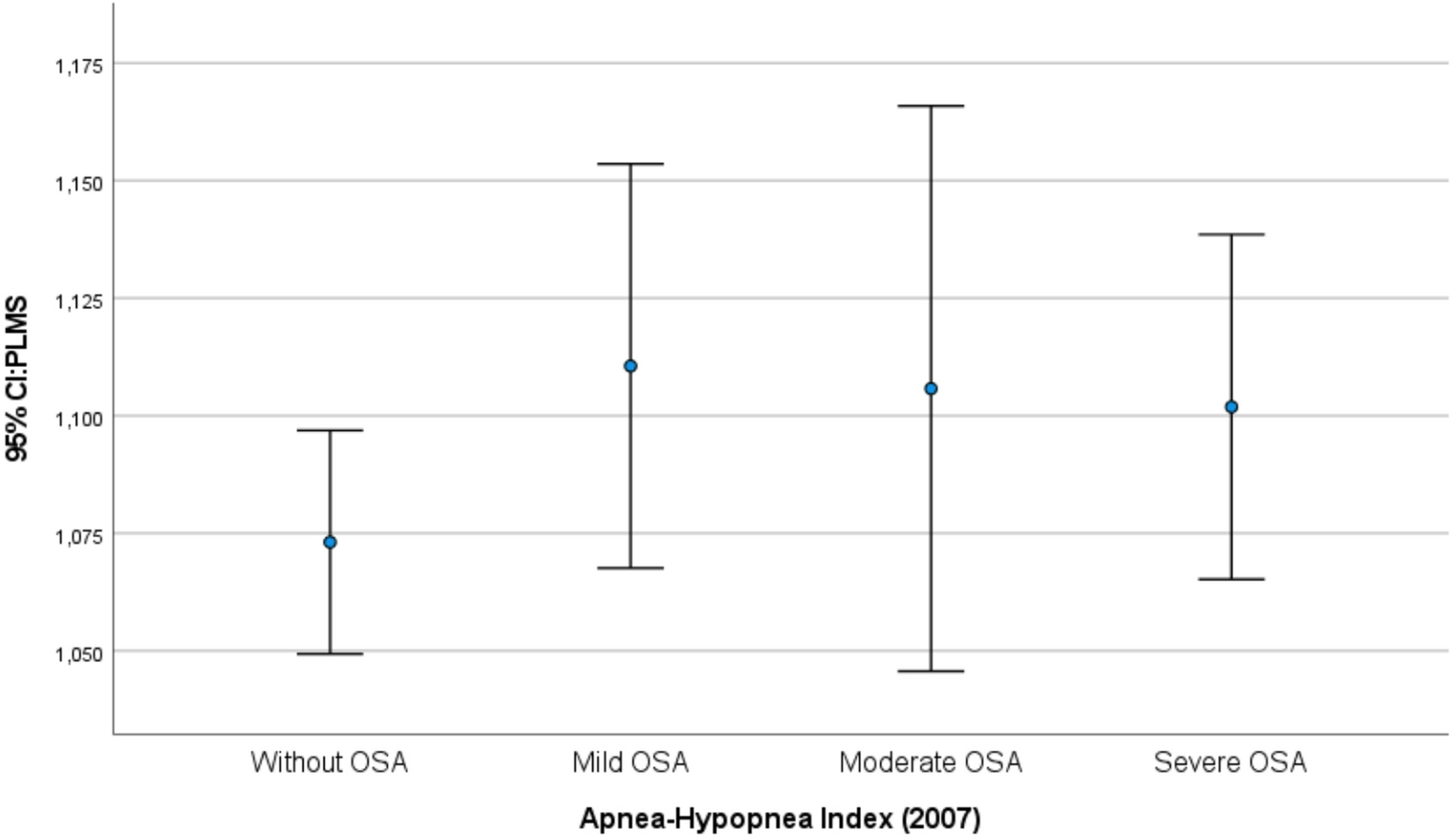
The potential mechanisms linking elevated Hcy concentrations to an increased risk of PLMS may involve oxidative stress, endothelial dysfunction, and neuroinflammation [31–33,32,] [–. Endothelial damage driven by oxidative stress and reduced nitric oxide bioavailability associated with elevated Hcy [33], may impair neuromuscular control [34] and thereby contribute to the development of PLMS. This overlap could also involve dysregulation of neurotransmitter systems. Reinforcing the possibility of shared pathophysiological mechanisms between PLMS and RLS, elevated Hcy concentrations—although with conflicting results—have been associated with RLS [11]. Previously, we found that Hcy was a predictor of increased AHI; individuals with plasma Hcy concentrations ≥ 15 µmol/L experienced an average AHI increase of 7.43 compared with those whose concentrations were < 10 µmol/L [35]. When evaluating the distribution of PLMS across the severity levels of sleep-disordered breathing, no significant differences were observed in either the 2007 or 2018 samples. Together, these findings suggest that Hcy may act as a common pathophysiological factor across different sleep disorders, potentially exacerbating conditions such as OSA and PLMS.
One of the main strengths of this study is its use of data from two EPISONO editions, conducted 11 years apart, in a large, population-based sample representative of São Paulo. The inclusion of sex-specific biochemical analyses and the investigation of novel biomarkers such as Hcy and hemoglobin significantly enriched the findings. However, this study has limitations, including the absence of a clinical evaluation to rule out other conditions related to PLMS, such as RLS, as well as the lack of an assessment for daytime impairment—both essential components for a PLMD diagnosis, which were not addressed in this research. Furthermore, when transforming cross-sectional studies into a historical series, changes in the scoring system are a possible consequence, as methodological advancements and adjustments in techniques and equipment are expected over time. However, in the current study, the analyses were performed independently, minimizing potential biases associated with these changes.
In conclusion, the findings from this study enhance our understanding of the biochemical and demographic factors associated with PLMS. Elevated Hcy concentrations were identified as a significant risk factor for the development of PLMS, potentially through mechanisms involving oxidative stress and neuroinflammation. Sex-specific biochemical alterations, particularly in men, further emphasize the need for additional research into underlying mechanisms. Additionally, hemoglobin emerged as a protective factor, possibly due to its role in supporting iron-related dopaminergic function. Considering time as a potential driver of changes in social and health policies, separately analyzing data from EPISONO 2007 and 2018 preserves the integrity of each sample and enables a robust evaluation of factors contributing to PLMS prevalence and its associated mechanisms. These insights provide a foundation for future research aimed at unraveling the mechanisms underlying PLMS and informing targeted intervention strategies.

Comments (0)