
Remember me
For several decades, corticosteroids have been widely used in the management of active vitiligo due to their potent anti inflammatory and immunosuppressive properties. At the molecular level, these agents broadly inhibit inflammatory signaling through genomic and non-genomic mechanisms, including suppression of transcription factors such as NFκB and AP1, inhibition of eicosanoid synthesis, and induction of anti inflammatory mediators that attenuate innate and adaptive immune activation [139]. These effects result in reduced cytokine production and transient attenuation of T-cell activity within the skin. Clinically, topical and systemic corticosteroids are employed to stabilize disease activity and, in selected cases, induce partial repigmentation, with systemic regimens such as oral mini pulse protocols reserved for rapidly progressive disease [140].
However, despite effectively suppressing inflammation, corticosteroids do not specifically target key pathogenic circuits underlying vitiligo. In particular, they fail to selectively disrupt the IFN-γ/JAK/STAT axis and its downstream induction of CXCL9 and CXCL10, which are central to the recruitment and retention of CXCR3⁺ autoreactive CD8⁺ T cells in the epidermis [141,142,143]. Moreover, these agents do not eliminate or functionally reprogram TRM cells, which persist in the skin and retain the capacity to rapidly reinitiate cytotoxic responses upon treatment withdrawal. As a result, corticosteroid therapy is frequently associated with disease relapse, reflecting suppression of immune activity rather than restoration of immune tolerance or resolution of pathogenic memory responses [144, 145].
Calcineurin inhibitors, including tacrolimus and pimecrolimus, act through a more targeted mechanism by blocking calcineurin-dependent dephosphorylation of NFAT, thereby inhibiting transcription of T cell-derived cytokines. These agents are commonly used as topical therapies, particularly for sensitive anatomical areas, and play an important role in maintenance strategies due to their favorable safety profile [146, 147]. This results in reduced T-cell activation and cytokine production, particularly within the CD4⁺ compartment. Clinically, these agents are widely used as topical therapies, especially in sensitive areas, and demonstrate efficacy in inducing repigmentation, particularly when combined with phototherapy [75,76,77,78,79, 148, 149].
Nevertheless, similar to corticosteroids, calcineurin inhibitors do not adequately interfere specifically with the recruitment of autoreactive CD8⁺ T cells or the survival signals sustaining TRM populations, such as IL-15 trans-presentation within the epidermal niche [108, 150]. Consequently, their effects are largely limited to modulation of active inflammation, without promoting durable immune reprogramming or preventing disease recurrence [151].
Within this broadly immunosuppressive framework, additional pharmacological agents have been explored as adjunctive therapies. Topical 5-fluorouracil when combined with lasers or microneedling appears superior efficacy in controlling disease progression and inducing repigmentation, particularly in acral areas and over bony prominences (e.g., elbows and knees) [152,153,154,155]. Similarly, methotrexate has been reported to improve clinical outcomes and repigmentation when used in combination with oral mini-pulse dexamethasone in cases of advanced and unstable vitiligo [156, 157]. In addition, low doses of oral methotrexate have been shown to prevent progression and allow for better and faster repigmentation in focal vitiligo lesions compared to phototherapy alone [158]. Mechanistically, methotrexate inhibits folate-dependent metabolic pathways and exerts anti-inflammatory effects partly through increased adenosine signaling; however, its impact on pathogenic T-cell subsets and resident immune memory in vitiligo remains insufficiently characterized in primary experimental studies [159]. While such approaches may improve disease control in specific contexts, they predominantly rely on generalized immune suppression.
Rapamycin represents a further example of a repurposed immunomodulatory agent with pleiotropic effects. By inhibiting mTOR signaling, rapamycin can modulate T-cell differentiation and promote autophagy, while also enhancing melanocyte function through upregulation of microphthalmia-associated transcription factor (MITF) and melanogenic enzymes [5, 160]. Based on these findings, topical rapamycin is currently under clinical investigation for vitiligo (NCT05342519). Nonetheless, its therapeutic rationale remains centered on immune and metabolic modulation rather than induction of sustained immune resolution.
Overall, these classical, adjunctive, and repurposed therapies underscore the conceptual limitations of strategies focused predominantly on broad immune suppression. Although they may stabilize disease activity and enhance repigmentation in selected clinical scenarios, they do not consistently support durable melanocyte regeneration or restore immune tolerance including the specific dampening of IFN-γ-dependent inflammatory amplification, IL-15-mediated maintenance of TRM cells, and the persistence of pathogenic memory T-cell populations. As a result, these approaches rarely achieve durable immune tolerance or long-term disease remission.
This recognition has driven a shift toward therapeutic approaches that more directly engage disease specific mechanisms and aim to promote long-term immune regulation together with functional recovery of the melanocyte compartment. Within this evolving therapeutic landscape, ultraviolet (UV) based phototherapy (described in detail latter in this review) occupies a distinctive position. Unlike purely immunosuppressive interventions, phototherapy exerts simultaneous effects on immune modulation and melanocyte activation, thereby representing a transitional strategy that links control of pathogenic immune responses with stimulation of cutaneous regeneration.
Targeted Immunomodulation and Cytokine-driven TherapiesJAK Inhibitors and TYK2 InhibitorsTargeted immunotherapies based on small molecules and monoclonal antibodies have progressively advanced from preclinical investigation to early and late phase clinical trials in vitiligo. Many of these agents were initially developed for other autoimmune or inflammatory diseases and were subsequently repurposed based on shared pathogenic mechanisms. In vitiligo, this therapeutic transition has been driven by the identification of cytokine-dependent signaling networks that sustain autoreactive T-cell responses within the skin, particularly those centered on IFN-γ and IL-15 signaling axes. Among them, inhibitors of JAK and tyrosine kinase 2 (TYK2) have received particular attention due to their capacity to modulate cytokine driven signaling pathways central to vitiligo pathogenesis [161, 162].
JAK inhibitors directly target these pathogenic circuits by interfering with multiple members of the JAK family (JAK1, JAK2, and/or JAK3), which are critical mediators of cytokine receptor-associated signaling pathways. As a result, they broadly attenuate downstream STAT-dependent transcriptional programs. For instance, binding of IFN-γ to its receptor complex triggers activation of JAK1 and JAK2, leading to phosphorylation of STAT1 and subsequent induction of CXCL9 and CXCL10, which are key chemokines in the recruitment and epidermal localization of CXCR3⁺ autoreactive CD8⁺ T cells, thereby sustaining a feed-forward inflammatory loop within vitiligo lesions [99, 163]. In parallel, TYK2 inhibition may act upstream by modulating CD4⁺ T-cell polarization, indirectly reducing IFN-γ production and downstream chemokine expression. This selective modulation may attenuate pathogenic immune activation while preserving other JAK-dependent physiological pathways, potentially translating into improved safety profiles [164].
This mechanistic rationale is strongly supported by clinical evidence. Ruxolitinib (Opzelura™), a topical JAK1/2 inhibitor, is the first targeted therapy approved for nonsegmental vitiligo (adults and children 12 years of age and older). Treatment significantly improved facial and total body repigmentation in adolescents and adults with non-segmental vitiligo, as measured by validated VASI endpoints [80], in addition to a favorable safety profile, limited to mild local adverse events and no new systemic signs [81]. In parallel, systemic JAK inhibition with oral ritlecitinib (JAK3/TEC inhibitor) induced clinically significant repigmentation, along with reductions in pro-inflammatory biomarkers at the transcriptional and protein levels, which correlated with increased markers associated with melanocytes. Notably, therapeutic response appears to depend on disease activity, with faster repigmentation in stable lesions and delayed responses in active disease requiring prior immunological control [165,166,167]. Consistently, oral upadacitinib (selective JAK1 inhibitor) also demonstrated significant and sustained improvements in facial and total body repigmentation in a phase II randomized trial [168].
Other agents currently under investigation include topical ivarmacitinib (NCT 04774809), topical cerdulatinib (NCT 04103060), oral baricitinib (NCT 04822584; NCT 05950542), oral povorcitinib (NCT 06113471; NCT 06113445), oral deucravacitinib (NCT 06327321), oral zasocitinib (NCT 07108283), and oral tofacitinib in combination with phototherapy (NCT 07044141).
IFN-γ / CXCL10 / CXCR3 AxisKinase inhibition strategies primarily attenuate upstream cytokine signaling. Nevertheless, effective disease control in vitiligo also requires direct interference with downstream effector mechanisms responsible for immune cell recruitment and melanocyte damage within the skin microenvironment. As described before, IFN-γ signaling induces CXCL10 expression and promotes CXCR3 dependent trafficking of cytotoxic T cells to the skin, thereby sustaining cutaneous inflammation [99, 163]. Importantly, IFN-γ signaling not only regulates immune cell trafficking but also reinforces effector function within the skin. In murine models of vitiligo, IFN-γ has been shown to be essential for the accumulation of autoreactive CD8⁺ T cells in lesional skin, and its neutralization prevents disease progression and reduces T-cell infiltration [103]. Furthermore, CXCR3 expression on CD8⁺ T cells is critical not only for their recruitment but also for their retention and positioning within the epidermis, where melanocytes reside. Disruption of the CXCL10-CXCR3 axis significantly impairs T-cell trafficking and attenuates depigmentation in experimental models, underscoring its role as a non-redundant pathway in disease maintenance [99, 163].
Systemic IFN-γ blockade is constrained by its critical role in antimicrobial defense and tumor immunosurveillance. To address this limitation, a bispecific antibody was engineered to neutralize IFN-γ while anchoring to keratinocytes via desmoglein binding, thereby restricting its activity to the epidermal compartment. This spatially targeted approach enables localized inhibition of IFN-γ signaling, resulting in decreased production of CXCL9 and CXCL10. In a murine model of vitiligo, this strategy effectively limited CD8⁺ T-cell accumulation in the skin and led to significant disease improvement [169]. While these findings support localized immunomodulation, the extent to which systemic immune functions are preserved remains to be fully determined [169].
Consistent with the central role of this pathway, genetic and pharmacological studies have demonstrated that CXCL10 is a non-redundant mediator of disease progression. Rashighi et al. demonstrated that Cxcl10 deficient mice, as well as mice treated with CXCL10 neutralizing antibodies, exhibited significantly reduced depigmentation and diminished accumulation of autoreactive CD8⁺ T cells in the skin. Notably, CXCL10 blockade in established lesions promoted partial repigmentation, indicating that this chemokine contributes not only to disease initiation but also to its maintenance [163]. Subsequent work from the same group further refined this concept by demonstrating that direct depletion of CXCR3⁺ T cells induces more durable perifollicular repigmentation compared with chemokine neutralization alone. Mechanistically, this approach eliminates autoreactive effector cells rather than solely impairing their migration, thereby disrupting both ongoing tissue damage and the reservoir of pathogenic T cells capable of reinitiating disease [170].
Together, these findings establish the IFN-γ-CXCL10-CXCR3 pathway as a central effector axis linking cytokine signaling to T-cell recruitment, epidermal positioning, and melanocyte destruction in vitiligo. However, the persistence and recurrence of disease activity cannot be fully explained by immune cell recruitment alone. Increasing evidence indicates that long-lived tissue-TRM cells persist within the skin and retain the capacity to rapidly reinitiate cytotoxic responses upon antigen re-exposure, even in the absence of continuous recruitment from the circulation [97].
These observations suggest that effective therapeutic strategies must not only disrupt inflammatory recruitment pathways but also target the mechanisms that sustain local immune memory and pathogenic persistence over time.
IL-15 and Tissue TRM CellsFurther studies expanded this concept by identifying IL-15 as a critical regulator of the survival, metabolic fitness, and effector function of epidermal CD8⁺ TRM cells. In vitiligo lesions, keratinocytes express IL-15 receptor alpha (IL-15Rα/CD215), enabling the trans-presentation of IL-15 to neighboring CD122⁺ (IL-2/15Rβ) TRM cells. This process facilitates the formation of a high-affinity receptor complex that activates JAK1 and JAK3, leading to STAT5 phosphorylation and transcriptional programs that promote T-cell survival, proliferation, and sustained effector function [150]. Through this mechanism, TRM cells are maintained as a long-lived, self-sustaining population within the epidermal niche. Functionally, these cells localize to the dermoepidermal junction, where they continuously or intermittently produce IFN-γ, thereby reinforcing local chemokine production and maintaining a pro-inflammatory microenvironment even in the absence of ongoing recruitment from the circulation. This establishes a localized immune memory circuit that contributes to disease persistence and rapid relapse following treatment discontinuation [97]. Consistent with this pathogenic role, experimental blockade of IL-15 signaling has been shown to selectively disrupt TRM cell maintenance. In murine model of vitiligo, antibody-mediated targeting of CD122 resulted in depletion of epidermal CD8⁺ TRM cells, reduced IFN-γ production, and induced durable repigmentation, even after cessation of therapy [108].
Building on these findings, early-phase clinical studies are now evaluating therapeutic strategies targeting the IL-15 axis in patients with vitiligo. A Phase 1b trial is assessing the safety and tolerability of the anti-IL-15 monoclonal antibody TEV-53408 (NCT06625177). In parallel, AMG 714, an anti-IL-15 monoclonal antibody, has been investigated in a Phase 2 clinical study, including in combination with narrowband UVB phototherapy (NCT04338581). Additionally, FB102, an anti-CD122 monoclonal antibody designed to block IL-2 and IL-15 receptor signaling, is currently being evaluated in a randomized, double-blind, placebo-controlled Phase 1 trial in patients with non-segmental vitiligo (NCT06905873).
Altogether, these strategies aim to disrupt a non-redundant survival pathway for pathogenic TRM cells, thereby targeting a key mechanism underlying disease persistence. In contrast to therapies that primarily inhibit immune activation or cellular recruitment, IL-15-directed interventions seek to eliminate or destabilize the local reservoir of autoreactive memory T cells within the skin.
However, within the broader conceptual framework in which vitiligo persistence is sustained by coordinated interactions between tissue-resident and systemic immune memory compartments, targeting TRM cells alone may be insufficient to achieve durable disease control. Current therapies, including JAK inhibitors, primarily suppress cytokine signaling pathways such as IFN-γ-JAK-STAT, effectively reducing inflammation and promoting repigmentation, but do not fully eliminate autoreactive memory T-cell populations that may persist across compartments [80].
Similarly, although IL-15 blockade can disrupt TRM maintenance and induce durable repigmentation in experimental models, these approaches may not fully address circulating or systemic memory populations, which can re-seed the skin and contribute to disease recurrence. This highlights that vitiligo is sustained not only by local immune circuits but by a distributed memory network that prevents a longstanding immunological control of the responses. Therefore, durable disease control in vitiligo will likely require therapeutic strategies capable of targeting both local and systemic immune memory, as well as promoting antigen-specific immune tolerance. This may include combination approaches integrating cytokine blockade, memory-cell modulation, and regenerative therapies aimed at restoring melanocyte homeostasis.
In parallel, complementary therapeutic strategies continue to target broader IFN-driven inflammatory programs that contribute to immune amplification and disease propagation, highlighting the need for integrated approaches that simultaneously address immune activation, memory, and tissue repair.
Type I IFN BlockadeType I IFN, including IFN-α and IFN-β, have emerged as important upstream regulators of innate and adaptive immune activation in vitiligo. These cytokines are primarily produced by pDCs in response to cellular stress and damage-associated molecular patterns released by melanocytes and keratinocytes. Upon binding to the type I IFN receptor (IFNAR1/IFNAR2), IFN-I activates JAK1 and TYK2, leading to phosphorylation of STAT1 and STAT2 and induction of IFN-stimulated genes (ISGs), which amplify inflammatory signaling and promote antigen presentation.
In the context of vitiligo, experimental evidence indicates that activation of pDCs and subsequent IFN-α production enhance antigen presentation and promote the activation and effector differentiation of melanocyte-reactive CD8⁺ T cells. In addition, type I IFN signaling increases MHC class I expression and sensitizes keratinocytes and immune cells to inflammatory stimuli, thereby facilitating the amplification of IFN-γ–dependent cytotoxic responses within the skin [29, 171].
Anifrolumab is a fully human monoclonal antibody that targets the IFNAR1 subunit, thereby blocking signaling induced by all type I IFN. This inhibition prevents activation of the JAK1-TYK2-STAT1/STAT2 pathway and reduces the transcription of IFN-stimulated genes involved in immune activation and inflammation. Clinically, anifrolumab has been approved by the United States Food and Drug Administration and the European Medicines Agency for the treatment of moderate to severe systemic lupus erythematosus, a disease strongly driven by type I IFN signaling [172].
Hence, based on the involvement of type I IFN in vitiligo pathophysiology, a clinical study is currently evaluating the efficacy and tolerability of anifrolumab infusions in combination with NB UVB phototherapy in patients with progressive disease (NCT05917561). The rationale for this approach lies in the potential to interfere with early innate immune activation and antigen presentation, thereby limiting the priming and expansion of autoreactive T cells that subsequently sustain IFN-γ-mediated tissue damage.
Beyond cytokine-directed interventions, additional therapeutic strategies have focused on restoring immune tolerance by modulating inhibitory pathways that regulate pathogenic T-cell activity.
Immune Checkpoint ModulationFrom a complementary perspective aimed at restraining pathogenic T cell activity through inhibitory immune checkpoints, modulation of the PD-1/PD-L1 axis has emerged as a biologically relevant strategy to restore immune tolerance in vitiligo. In experimental model of vitiligo, enhancement of PD-1 signaling has been shown to suppress pathogenic immune responses. Miao et al. demonstrated that systemic administration of a PD-L1 fusion protein in the Pmel-1 mouse model resulted in a significant reduction in depigmentation, with approximately 58% improvement compared with untreated controls. Mechanistically, this effect was associated with a marked expansion of Tregs in both skin and lymphoid organs, alongside a substantial reduction in effector T cells, indicating a shift toward a more regulated immune state [6]. These findings are consistent with the broader role of PD-1 signaling in promoting T-cell exhaustion and functional restraint, particularly within chronically inflamed tissues. In the skin, engagement of the PD-1/PD-L1 axis may limit the cytotoxic activity of CD8⁺ T cells and modulate the balance between effector and regulatory compartments, thereby counteracting the IFN-γ-driven inflammatory circuits that sustain melanocyte destruction.
Despite this strong preclinical rationale [173,174,175,176], there are currently no clinical studies evaluating PD-1/PD-L1 agonist strategies in patients with vitiligo. Moreover, therapeutic enhancement of checkpoint signaling raises important safety considerations. Systemic or even localized immunosuppression may impair host defense against infections and tumor surveillance, particularly in the skin, which serves as a critical barrier tissue. In addition, excessive inhibition of T-cell activity could potentially interfere with normal immune surveillance mechanisms or lead to unintended alterations in tissue-resident immune populations, including regulatory and memory T-cell subsets. Another key limitation lies in the incomplete understanding of how PD-1 modulation affects TRM cells, which are central to disease persistence. While PD-1 signaling may restrain effector function, it is unclear whether it can effectively eliminate or reprogram pathogenic TRM populations, raising the possibility that checkpoint-based therapies may suppress inflammation without achieving durable immune resolution.Taken together, these observations indicate that although immune checkpoint modulation represents a biologically plausible strategy to restore peripheral tolerance in vitiligo, its clinical translation requires careful evaluation of efficacy, specificity, and safety. Future studies should aim to define whether targeted or tissue-restricted approaches can harness the immunoregulatory potential of checkpoint pathways while minimizing systemic immunosuppressive risks.
Together, these observations establish immune checkpoint pathways as critical regulators of immune balance in vitiligo, linking defective inhibitory signaling to sustained autoreactive T-cell activity. While still underexplored therapeutically, strategies aimed at enhancing checkpoint signaling may offer a means to restore immune tolerance and counteract the failure of durable immune control that characterizes the disease.
In parallel with efforts to reestablish immune regulation through cytokine-targeted therapies and checkpoint engagement, additional innovative pharmacological approaches are necessary to fully address the underlying metabolic dysfunction that sustains immune activation and melanocyte vulnerability.
Immunometabolic Therapeutic Strategies: Targeting Oxidative Stress and Metabolic ReprogrammingSelective Immunomodulators With Metabolic EffectsEmerging therapeutic strategies in vitiligo increasingly recognize that immune dysregulation is tightly coupled to metabolic dysfunction. Rather than acting solely on cytokine signaling, these approaches aim to modulate immunometabolic pathways that govern redox balance, mitochondrial integrity, and inflammatory activation, thereby addressing both melanocyte vulnerability and immune persistence.
One of the central targets within this framework is oxidative stress. Pharmacological activation of the Nrf2-ARE pathway has been shown to restore antioxidant defenses and protect melanocytes from oxidative damage. For instance, Ma J. et al. demonstrated that baicalein enhances Nrf2 signaling, reduces intracellular reactive oxygen species, and prevents apoptosis in human vitiligo melanocytes [177]. However, these findings are currently limited to in vitro studies and preclinical models, with no clinical trials in patients with vitiligo to date. Similarly, Chang Y. et al. showed that simvastatin improves cellular resistance to oxidative stress [178]. However, although simvastatin is clinically approved for other indications, its use in vitiligo remains experimental and has not been validated in controlled clinical trials.
In addition to redox modulation, targeting mitochondrial dysfunction has emerged as a promising strategy. Recent studies have shown that inhibition of VDAC1 oligomerization reduces mitochondrial DNA release and attenuates activation of the cGAS–STING pathway, thereby limiting innate immune activation and inflammatory amplification in vitiligo [179]. These approaches remain at the preclinical stage and have not yet been translated into human studies.
Another important metabolic target is the inflammasome pathway. Tranilast, an inhibitor of NLRP3 inflammasome activation, has been shown to suppress IL-1β production and prevent inflammation-induced melanocyte dysfunction [38]. Importantly, this mechanistic effect has been described in preclinical and in vitro models, and there are currently no clinical trials evaluating tranilast specifically for vitiligo.
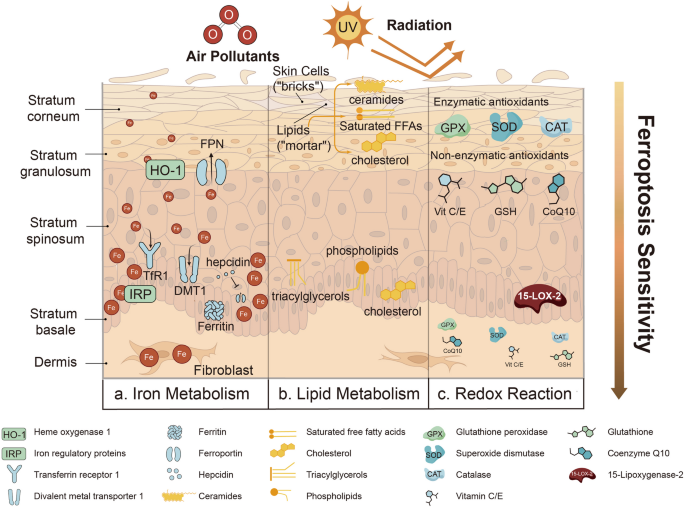
Ferroptosis has also been proposed as a novel therapeutic target. Alterations in iron metabolism and lipid peroxidation pathways contribute to melanocyte death in vitiligo, suggesting that ferroptosis inhibitors may provide cytoprotective effects and preserve the melanocyte pool [43]. However, therapeutic targeting of ferroptosis in vitiligo remains an emerging concept without clinical validation.
Within this immunometabolic framework, previously described agents can be reinterpreted as modulators of metabolic-immune interactions rather than solely immunosuppressive drugs. Lenalidomide, an immunomodulatory derivative of thalidomide, exemplifies this dual activity by modulating cytokine production and immune cell function. In a murine model of vitiligo, oral administration of lenalidomide for six weeks significantly reduced lesion development and suppressed key pro-inflammatory cytokines, including IFN-γ, tumor necrosis factor (TNF), and IL-6, while concomitantly increasing anti-inflammatory mediators such as IL-4 and IL-10. Notably, these effects occurred without significant changes in the CD4⁺/CD8⁺ T-cell ratio, suggesting functional reprogramming rather than depletion of immune subsets [180]. Despite these promising results, lenalidomide has not been evaluated in clinical trials for vitiligo and remains a preclinical or experimental candidate.
Another relevant class of immunometabolic modulators comprises phosphodiesterase 4 (PDE4) inhibitors, which exert anti-inflammatory effects by increasing intracellular cyclic adenosine monophosphate (cAMP) levels. Elevated cAMP activates protein kinase A (PKA), which can suppress pro-inflammatory signaling pathways, including NF-κB, leading to reduced cytokine production [
Comments (0)