The following sections discuss common neurologic diseases which may present first to a urology clinic with LUTS, potentially before the neurologic condition is diagnosed, or even suspected. The Urologist should be particularly aware of multiple sclerosis (MS) and related neuro-inflammatory disorders, multiple system atrophy (MSA), Parkinson’s disease (PD), normal pressure hydrocephalus (NPH), dementia, structural spinal cord lesions [6], and small fiber neuropathy (SFN) [9] as the potential for LUTS to precede or call attention to other neurological symptoms is significant.
Central Neurologic DisordersMultiple Sclerosis and Related Neuroinflammatory Disorders
Multiple Sclerosis (MS), Neuromyelitis Optica Spectrum Disorder (NMOSD), and Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease (MOGAD) are neuroinflammatory disorders characterized by immune-mediated axonal damage throughout the CNS. All can cause transverse myelitis with spinal cord inflammation and axonal injury. The average age of onset is similar for these disorders, with mean ages of 20–30, 40.3, and 30 years respectively, and typical time from symptom onset to diagnosis is 1–2 years [10,11,12,13,14,15]. Patients can experience both storage and voiding symptoms depending on the location of the lesion.
MS primarily affects the brain (demyelinating plaques) and optic nerves, but transverse myelitis of the spinal cord occurs in 25%. Nearly 90% of patients with MS experience LUTS; they typically worsen with disease duration and spinal cord involvement and have been reported to appear up to 8 years after diagnosis [7, 16]. Patients most commonly experience storage symptoms such as urinary urgency (62–65%), frequency (50%), urge incontinence (45%), and nocturia (35%) [17, 18], but voiding symptoms (incomplete emptying, straining, weak stream) can be present secondary to detrusor external sphincter dyssynergia (DESD) or detrusor underactivity (DO) depending on the level of spinal cord involvement. Incomplete emptying can lead to recurrent urinary tract infection (UTI) [16, 19, 20]. Both voiding and storage symptoms are reported in up to 50% [7]. Erectile dysfunction (53%) and bowel dysfunction (40%) can be present early in disease [21]. Due to the inflammatory nature, history may include an abrupt onset of symptoms with subsequent improvement. Neurological symptoms may include monocular vision loss, blurred or double vision, sensory loss, weakness, ataxia, sensory loss of the face, arm, legs, pins and needles, gait disturbance, and weakness.
NMOSD is a debilitating group of syndromes associated with aquaporin-4 immunoglobulin G antibodies (AQP4-IgG) affecting the optic nerve, brainstem, and spinal cord. Patients may present with optic neuritis, myelitis, unexplained and intractable hiccups, and nausea [22]. NMOSD causes transverse myelitis more often than MS and involves more longitudinal extension within the spinal cord, leading to storage and voiding symptoms in 78–83% of patients [7]. Urinary retention is the most common symptom in this group [23]. Urodynamics demonstrates DO and DESD in over one third of cases [24].
MOGAD affects myelin oligodendrocyte glycoproteins (MOG) on myelin sheaths. Patients may present similarly to MS and NMOSD with optic neuritis and transverse myelitis but may also have acute disseminated encephalomyelitis (ADEM) and inflammatory demyelinating lesions anywhere in the CNS [25]. Diagnosis of MOGAD is by MOG antibody, which can be negative early in disease, as can MRI. Patients may experience urinary retention as an early sign of MOGAD [26] as the conus is particularly susceptible to injury in this condition. Overall LUT dysfunction is present in 28–59% of patients and whereas often the motor dysfunction improves, the urinary symptoms can remain [27].
Urodynamic findings in neuroinflammatory disease depend on the level affected (Table 1, Supplemental Table 1a-d). Higher level lesions of the neuroaxis would result in detrusor overactivity (DO) with or without DESD (Table 1, Supplemental Table 1a-b), decreased capacity, and over time possible decreased compliance (due to chronic mechanical stress and intermittent ischemia, which activate cellular repair and fibrosis pathways). Any level of the CNS is possible in all three, for example MOGAD is known for impacting the conus, which would lead to atonic bladder. In MS, as disease progresses, it is well known that urodynamic tracings change. Prompt urodynamic testing is recommended in the case of change in symptoms, and interval studies should be undertaken in concerning patterns such as poor compliance or vesicoureteral reflux [28].
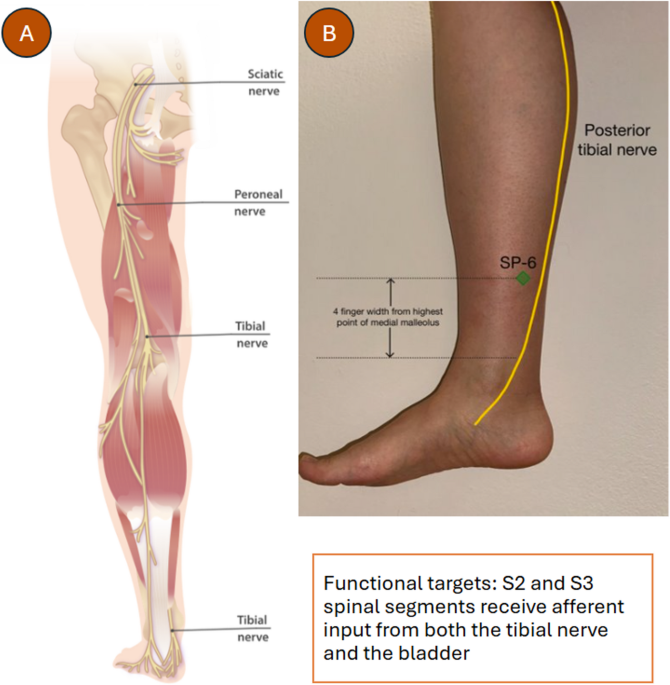
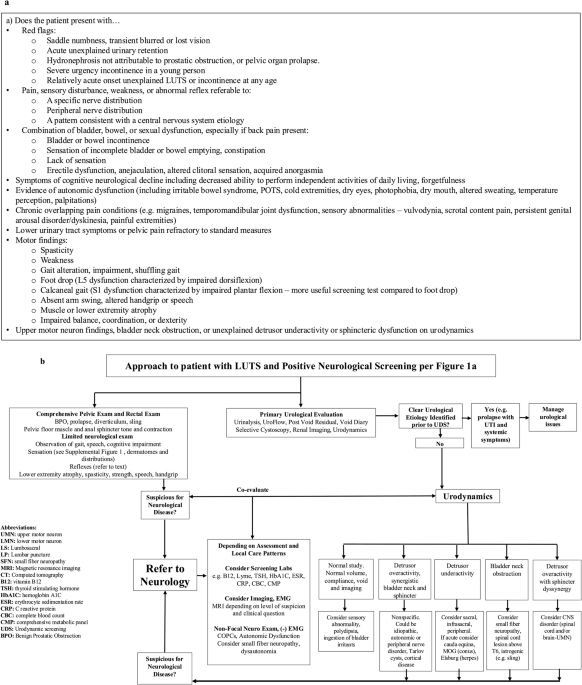
Table 1 Categorization of neurological conditions by level of impact on central and peripheral nervous system. Lower urinary tract symptoms and expected urodynamic findings by level. Peripheral nerve image: courtesy https://nigms.nih.gov/image-gallery/3263 and Stephen Dalton, University of GeorgiaParkinsonian Disorders
Whereas LUTS are highly prevalent in PD, affecting between 27 and 85% of patients [7, 29,30,31], it is rare to see Parkinson’s as OND presenting with LUTS. Motor symptoms are typically present at diagnosis (tremor, rigidity, bradykinesia, postural instability) occurring at a mean age of 55–65 years old [32]. Parkinson’s disease is linked to MSA, Dementia with Lewy Bodies (DLB) and pure autonomic failure (PAF) in that they are all synucleinopathies – misfolded alpha-synuclein is abnormally deposited in cellular locations and patterns that lead to the distinct disorders. In Parkinson’s disease, degeneration of subcortical and cortical regions leads to disruption of dopamine D1-mediated GABAergic direct pathways, which is thought to contribute to impaired bladder control, reduced inhibition of the micturition reflex, and overactive bladder symptoms [7, 30]. The most common symptom PD patients experience is nocturia, followed by urinary urgency and increased frequency. Though symptoms may be present early in the disease course, they are exacerbated by disease progression. UTI is a debilitating and common complicating of LUT dysfunction in PD patients, most often in the setting of incomplete emptying [33].
The most common urodynamic findings early in PD include DO and low PVR due to loss of inhibition of the basal ganglia on the PAG. In late PD, bladder underactivity and high PVR occur mainly secondary to PMC dysfunction, as well as impaired autonomic (parasympathetic) input. Dysfunction of the external sphincter (pseudodyssynergia, Supplemental Table 2a) is now thought to play a more minor role but can show as a dilated prostatic urethra during voiding [7, 34,35,36,37]. Normal to poor bladder compliance (due to repeated involuntary contractions over time with cyclic ischemia and fibrosis) can be seen.
In contrast to PD, MSA is more likely to present with LUTS, with symptom onset at mean ages of 55–60 years old and time to diagnosis typically around 3 years [38, 39]. If affects 8 per 100,000 over age 40 and impacts genders equally. MSA is a devastating and progressive neurodegenerative disorder in which α-synuclein deposits impact the oligodendroglial cells, disrupting myelination and neuronal support. This affects central autonomic centers (brainstem, PMC, and PAG), spinal autonomic neurons, and sometimes peripheral autonomic fibers. Patients present with parkinsonism, cerebellar ataxia, slurred speech, sleep problems, upper motor neuron (UMN) pyramidal signs [40, 41], hypotension, cardiovascular dysfunction [42]. LUTS (urinary urgency with or without incontinence, nocturia, hesitancy, urinary retention) are common at presentation, are observed in 90% of cases overall [41, 43]. LUTS have been reported to precede motor symptoms by an average of 2.8 years in 20%In 20%, LUTS have been reported to precede motor symptoms by an average of 2.8 years [40, 41, 44]. For many men, erectile dysfunction is an early feature. Urinary retention can be a presenting feature [40]. In retrospect, 40% of men with MSA who presented with LUTS were misdiagnosed with BPH and had a poor outcome after prostate surgery [45].
Urodynamic findings of an open bladder neck during filling (Supplemental Table 2d) is present in 53% of patients with MSA and in none with PD [46] and is the most suspicious urodynamic finding. An open prostatic urethra may be seen during voiding. Detrusor overactivity (33–100%) and uninhibited external sphincter relaxation (33%) are similar to PD [46,47,48]. DESD is present in 47%. Detrusor underactivity is seen in in 71% of women and 63% of men with MSA (underactivity can be present in Parkinson’s but is less common [46]). Elevated post void residuals are present more commonly early in MSA versus PD and worsen over time. Impaired bladder sensation and poor compliance can also occur [34, 48], as variable findings can be seen depending on the stage of disease. Detrusor underactivity and external sphincter electromyography (EMG) abnormalities (degeneration of Onuf’s nucleus) suggest later stage and/or spinal involvement [47].
Dementias – NPH and other Dementias
The most common reported symptom in dementia is incontinence due to DO, which occurs secondary to decreased inhibition of the PMC (and therefore of the bulbospinal reticulospinal micturition reflex) [49]. LUTS are most common in patients with Lewy Body Dementias (DLB) and vascular dementias (80–90%) compared to frontotemporal and Alzheimer’s dementia (25–40%) [49] due to impact on regulation of the PMC.
In DLB, α-synuclein deposition is primarily neuronal (Lewy bodies and neurites) and affects cortex, limbic structures, basal ganglia, and brainstem/autonomic centers. Symptoms include early dementia, parkinsonism, autonomic dysfunction, and LUTS with mean age of onset at 68 years old and mean age of diagnosis at 72 years [50]. It presents similarly to PD, with additional psychiatric symptoms and memory impairment preceding the motor symptoms. LUTS typically present later in the disease with the most reported symptoms being nocturia and urgency urinary incontinence [7, 51, 52]. Urodynamics show DO with minimal PVR [51]. Additional findings in dementia patients can include decreased compliance and reported instances of decreased sphincter relaxation, likely due to impaired coordination of the PMC and basal ganglia control [37].
Vascular dementia is a broad term involving a broad spectrum of vascular cognitive impairment, including stroke, commonly occurring in individuals above 65 years old [53]. However, it most often is used to refer to small vessel ischemic damage affecting subcortical white matter. This is a more subtle form of vascular disease that can lead to frontal subcortical disinhibition of the PMC, leading to urgency, increased frequency, and urgency incontinence before significant cognitive decline, with worsening symptoms as white matter changes increase [54, 55]. Urodynamic studies are mixed, showing DO [55] or even underactivity with decreased sphincter contractability and relaxation correlating with the severity of ischemia [37, 56].
Normal pressure hydrocephalus (NPH) is a mechanistically distinct form of dementia presenting with a triad of gait disturbances, cognitive impairment, and urgency urinary incontinence, primarily occurring in individuals after age 60 [57]. Enlargement of the brain ventricles occurs despite a relatively normal cerebrospinal fluid pressure, compressing nearby frontal and periventricular white matter tracts, decreasing cortical inhibition to the PAG and PMC. One study found that the most common and bothersome LUTS in patients with new-onset NPH were nocturia and urgency incontinence [58]. Urinary urgency has been demonstrated to be an earlier manifestation with incontinence developing as the disease progresses [58, 59]. UDS findings show predominantly DO, with some instances of bladder outlet obstruction, and detrusor underactivity in a very small percentage of patients [58, 60].
Cerebrovascular Disease
While vascular dementia and cerebral small vessel disease produce lower urinary tract symptoms through chronic suprapontine disinhibition, cerebrovascular disease from focal infarction represents a distinct mechanism in which LUT dysfunction varies according to lesion acuity, laterality, and involvement of descending motor pathways - severity and location of the UMN damage [37]. Risk of cerebrovascular disease begins in middle age, increasing to peak risk around 70 years of age [61].
Spinal Canal Stenosis
Whereas acute spinal cord injury is unlikely to present as OND with LUTS, “spinal stenosis” involves chronic narrowing of the spinal canal compressing the cord or nerve roots secondary to degenerative changes or spondylolisthesis. Degenerative changes commonly present around the mean age of 64–65 years old [62]. Compression of the spinal cord may produce neurological deficits below the level of lesion, including gait disturbance, sensory changes, and LUTS. The most common sites of stenosis are the cervical and lumbar spine. Patients may present with extremity pain and/or paresthesia, and LUTS typical of the applicable spinal cord level (specifically underactivity, incomplete bladder emptying, overflow incontinence and frequent UTIs below S2, and hesitancy, urgency incontinence, nocturia at higher levels [63]). Back pain can be absent if only central compression occurs.
Cauda equina syndrome is most commonly recognized as an acute presentation characterized by saddle anesthesia, poor detrusor contraction, external urethral sphincter laxity, loss of anal tone, and stress or overflow incontinence due to compression of the cauda equina, the bundle of lumbar and sacral nerve roots (typically L2-S5), but can also be chronic in the setting of spinal stenosis or slow growing spinal tumors. Urodynamic testing for stenosis at this level shows increased bladder capacity and PVR, preserved or increased compliance, and low flow rate [63, 64], and higher levels would be expected to match the spinal cord level, as shown in Supplemental Table 1c. As spinal stenosis occurs typically in older individuals, anatomic factors such as prostatic obstruction or pelvic organ prolapse may play a role.
Craniocervical Junction Disorders (Chiari Malformation, Craniocervical Instability)
Disorders of the craniocervical junction, including Chiari malformation and craniocervical instability, impact the level between the pons and the spinal cord, best classified as infrapontine lesions, involving the lower brainstem (medulla), cervicomedullary junction, and upper cervical spinal cord. They may impair brainstem and upper cervical cord control of urination, leading to LUT and autonomic symptoms that can precede overt neurologic diagnosis. Cervicomedullary compression interferes with descending inhibitory control over the PMC leading to DO on urodynamic testing. The reticulospinal pathways from the PMC to Onuf’s nucleus are preserved, at least early, and in the absence of significant cervical myelopathy or syringomyelia, DESD is absent [3, 65]. Symptoms worsen particularly with Valsalva, exertion, sustained upright posture, or neck movement (e.g. looking up) and are accompanied by headache, neck pain, dysphagia, upper‑extremity paresthesias, or other autonomic features. Routine brain or spine MRI may be normal, necessitating targeted posterior fossa or dynamic craniocervical imaging when suspicion remains high.
Sacral LesionsSpinal Bifida
Spina bifida may cause disruption to the spinal cord and can be diagnosed prenatally, immediately upon delivery, or be missed, even into adulthood (spina bifida occulta) [66, 67]. It has a 12% prevalence radiographically but only 1/1000 of the population has neurological sequelae [68]. Patients can experience lower extremity paresthesia, weakness or spasticity, unexplained gait disturbance, lower extremity atrophy (may have different shoe sizes), back pain, hairy tuft, scoliosis, bowel dysfunction and LUTS [5]. It can be associated with tethered cord syndrome, in which case history may reveal onset of symptoms during teen years or other growth spurts. Urodynamic findings are varied, especially if tethered cord is identified, as the tension can lead to a mixed upper and lower motor neuron picture (normal, increased or reduced capacity, compliance, and detrusor activity with or without DESD depending on the extent of the tethered cord) [37]. Detrusor overactivity has been reported in 42% and poor compliance in 67% [69]. If only the sacral nerve roots are involved without tethering, detrusor underactivity with a compliant bladder would be expected.
Sacral Cysts
Tarlov perineural spinal cysts (TCs) are dilations that form within the sensory nerve root sleeves, where cerebral spinal fluid (CSF) extends distally and can accumulate. They are typically asymptomatic until the fourth to sixth decade of life [70]. They occur most often in the sacral spine where the nerve roots are under the highest hydrostatic pressure and lack enclosing vertebral foramina, and are more common in women and in those with connective tissue disorders. As CSF accumulates between the perineurium and endoneurium, it stretches traversing axons and displaces them laterally into cyst walls. Axons under pressure can fire spontaneously, triggering neuropathic symptoms, and ruptured axons cause distal Wallerian degeneration, denervating peripheral targets. They are present in 15% of individuals and thought to be symptomatic in 15% of cases, most commonly causing sacral dermatomal neuropathic pain (e.g. S2 pelvic dermatomal pain radiating to the inner calf), as well as bladder, bowel, and sexual dysfunction (e.g. persistent genital arousal disorder (PGAD)) [71]. Urinary symptoms are reported in more than 90% of patients, and sacral root injury has been objectively demonstrated in nearly 60% of patients through pelvic neurophysiology testing [72]. Urodynamic patterns can be mixed depending on location of the cyst along the nerve root. Urinary symptoms and objective sacral root injury is demonstrated in most patients with midline meningeal sacral cysts [73]. Sacral cysts are not consistently reported by radiologists [72] and therefore it is helpful to look oneself for cystic structures that are bright on magnetic resonance T2 imaging of the lumbosacral spine and pelvis.
Sacral Chordoma
Sacral Chordoma typically presents at a mean age of 62.7 years old [74] with local pain and progressive neurologic or pelvic symptoms due to a slow-growing tumor arising from notochord remnants in the sacrum. It can be worse with sitting, and radiate to the buttocks or posterior thighs. Involvement of the S2-S4 nerve roots can cause LUTS and radicular lower extremity pain or weakness. A palpable fullness may be appreciated on rectal exam. Due to its slow progression, time from symptom onset to diagnosis can be prolonged, with median time of 2 years [75]. Early diagnosis improves prognosis.
Infectious Sacral Radiculopathies (HSV, VZV)
HSV-2 can cause sacral radiculitis affecting the S2-S4 nerve roots (Elsberg syndrome), producing subacute or acute lower urinary tract symptoms [76]. Acute urinary retention or acute voiding dysfunction with pain can occur, as well as bowel or sexual dysfunction. Visible genital lesions are not always present. Herpes Zoster–related sacral radiculopathy can present prior to the rash and can be in association with dermatomal pain out of proportion to exam, typically presenting in older populations [

Comments (0)