In Pediatric En Bloc Kidney Transplantation (N = 6)
Selected baseline characteristics and kidney graft outcomes for each patient appear in Table 1. The first successful transplant of pediatric en bloc kidneys with donor bladder inclusion was performed in early 2006 in a 12-month-old female recipient with a congenitally very small bladder; donor age was 2 years (see Table 1). Due to poor bladder capacity of the recipient, approximately 90% of the entire donor bladder was transplanted en bloc with the 2 donor kidneys and ureters [8]. Long-term functional outcomes were recently published [11], and the 17-year follow-up of this patient included an evaluation of entire-bladder function at 17 1/2 years of age. The patient has remained free of urinary tract infections throughout the follow-up period. Cystoscopy demonstrated a viable transplanted bladder with a well-perfused mucosa. Over time, the native bladder expanded, now forming more than half of the total bladder wall. Urodynamic assessment revealed preserved bladder compliance (43 mL/cm H₂O) and maintained native bladder contractility. However, prolonged voiding time and post-void residual urine were observed, findings consistent with detrusor underactivity. No vesicoureteral reflux across the donor ureterovesical junctions was identified. The recipient was advised to continue timed and double voiding to ensure complete bladder emptying. In conclusion, pediatric en bloc kidney transplantation incorporating a bladder patch that includes the entire trigone represents a feasible and durable surgical option for kidney transplant recipients with severely reduced bladder capacity, offering sustained function and low complication rates during long-term follow-up [11].
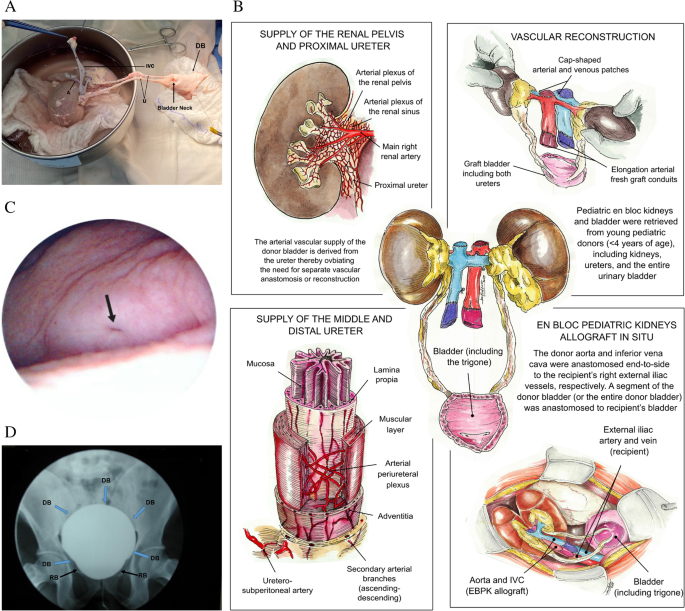
Table 1 Selected baseline characteristics and kidney graft outcomes for each patientWe also reported the first successful transplant of pediatric en bloc kidneys with donor bladder inclusion in an adult (45-year-old) male recipient; donor age was 13 months [9]. This recipient had been on long-term hemodialysis and presented with a small, contracted bladder secondary to long-standing anuria. The donor bladder was included here to avoid performing bilateral ureteroneocystotomies of extremely small pediatric ureters as well as to augment the recipient’s native bladder, with approximately 90% of the entire donor bladder being transplanted en bloc with the 2 donor kidneys and ureters. Cystoscopy evaluations at 3mo and 18mo post-transplant demonstrated a viable and well-vascularized bladder segment with normal donor mucosa and no evidence of ischemia (Fig. 1C). Cystography revealed no vesicoureteral reflux (Fig. 1D). The transplanted bladder segment initially received perfusion through the donor ureteral vasculature, later developing neovascularization from the recipient (native) bladder. This technique not only eliminates the need for performing complex bilateral ureteroneocystostomies but also allows for augmentation of bladder capacity, providing a promising surgical alternative in selected patients with a very small, contracted bladder or in need of bladder augmentation [9]. The third patient who received pediatric en bloc kidneys with donor bladder inclusion was a 28-year-old female recipient with ESKD due to systemic lupus erythematosus (SLE) who had been on hemodialysis for approximately 6 years; donor age was 2 years. Pre-operatively, the recipient was noted to have a small, contracted bladder; thus, approximately 90% of the donor bladder was included to achieve urinary tract reconstruction. At 12mo post-transplant, cystoscopy and biopsy of the donor bladder demonstrated no histological evidence of rejection - only some mild mucosal edema was observed. Unfortunately, the patient died with a functioning graft at 14mo post-transplant due to sepsis with a 12mo serum creatinine of 0.87 mg/dL.
The fourth recipient was a 47-year-old female with ESKD due to focal segmental glomerulosclerosis (FSGS) who had been maintained on hemodialysis for approximately 6 years; donor age was 10 months. Since in this case the recipient had reasonable bladder compliance, only 40%-50% of the donor bladder was included. At 12mo post-transplant, the patient’s serum creatinine remained stable at 0.8 mg/dL. Unfortunately, she later developed antibody-mediated rejection that was refractory to antirejection therapy, ultimately resulting in graft loss and return to dialysis. She is currently awaiting a second kidney transplant.
The fifth recipient was a 33-year-old male with ESKD secondary to biopsy-proven glomerulonephritis and on hemodialysis for approximately 3 years; donor age was 8 months. Since this recipient had reasonable bladder capacity, only 40%-50% of the donor bladder was included. At 5 years of post-transplant follow-up, serum creatinine was 0.62 mg/dL, and there were no voiding issues [12].
We recently performed our sixth pediatric en bloc kidney transplant incorporating a donor bladder segment. The recipient was a 45-year-old male with ESKD due to biopsy-proven FSGS who had been on peritoneal dialysis for approximately 1 ½ years; donor age was 3 years. Since this recipient had reasonable bladder capacity, only 40%-50% of the donor bladder was included. At 6mo post-transplant, the recipient’s serum creatinine was 1.1 mg/dL, with no evidence of urinary voiding complications.
In Simultaneous Pancreas and Pediatric En Bloc Kidney Transplantation (N = 2)
Sageshima et al. [13] reported two cases of adult female recipients (ages 32 and 35 years) undergoing simultaneous pancreas and pediatric en bloc kidney transplantation from very small donors (14- and 18-months-old) using a donor bladder segment in performing the ureteral/vesical reconstruction. Our technique involved procurement of the donor kidneys en bloc with both ureters and a segment of donor bladder (the bladder patch) such that no ureteroneocystostomies for very small donor ureters were required. Since both recipients had reasonable bladder capacity, only 40%-50% of the donor bladder was included in these 2 cases.
One of the takeaways of this report is the current underutilization of very small pediatric donors for combined pancreas-kidney transplantation because of concerns about insufficient islet cell mass, donor size, and what was previously thought as being technically complicated-to-perform urinary tract reconstruction. The use of a segment of donor bladder technique offers a surgical solution to the challenge of implanting very small ureters: using the donor bladder segment (with ureterovesical junctions intact), technical complexity and risk of urinary complications are greatly reduced.
At 2 years post-transplant, the first SPK recipient still had sustained euglycemia without requiring exogenous insulin, showing that even very small pediatric donors can provide sufficient islet mass for adult recipients when appropriately managed. The first SPK recipient then became insulin dependent by 3 year post-transplant, while the second SPK recipient became insulin dependent by 6mo post-transplant. In fact, the second SPK recipient developed pancreas graft failure (due to acute rejection/graft sclerosis) at 11mo post-transplant. Both patients continued dialysis independence through 3 year post-transplant, demonstrating that pediatric en bloc pediatric kidneys can grow and maintain normal renal function for an extended time post-transplant. However, the first SPK recipient developed kidney graft failure at 4.2 year post-transplant due to chronic allograft injury (following numerous acute rejection episodes), and the second SPK recipient died with a functioning kidney graft (likely due to a cardiovascular event) at 4.2 year post-transplant. The absence of any urinary tract complications in these 2 patients also validates the surgical concept of transplanting the donor bladder segment with an intact trigone, preserving the native ureterovesical junctions and effectively avoiding the risks inherent to performing multiple ureteral anastomoses in very small donor ureters [13]. This work demonstrates the feasibility of using very small pediatric donors for combined pancreas and kidney transplantation in adults, thereby expanding the donor pool.
In Pediatric En Bloc Simultaneous Liver-Kidney Transplantation (N = 2)
In the report by Kunzler de Oliveira Maia et al. [14], four pediatric recipients underwent combined organ transplantation using pediatric donor en bloc kidneys with donor bladder inclusion. One of these 4 patients was a 3-year-9-month-old male, with a history of autosomal dominant polycystic kidney disease (ADPKD) and congenital hepatic fibrosis. He began peritoneal dialysis at age 2 months and transitioned to hemodialysis at age 4 months. The recipient underwent pediatric en bloc simultaneous liver and kidney transplantation with donor bladder inclusion from a 4-month-old donor; thus, no ureteroneocystostomies for very small donor ureters were required. This recipient had a reasonably compliant bladder; thus, approximately 40%-50% of the donor bladder was included here. At 10 years post-transplant, this patient remains free of any urinary complications involving the donor bladder as well as being dialysis-free with excellent graft function.
The second recipient of a pediatric en bloc simultaneous liver and kidney transplantation with bladder inclusion was a 21-month-old female, not included in the Kunzler de Oliveira Maia et al. [14] report. Of note, this recipient’s bladder was small and contracted since birth (congenital); thus, approximately 90% of the donor bladder was included as part of performing bladder augmentation. At 6 years post-transplant, this patient remains free of any urinary complications involving the donor bladder as well as being dialysis-free with excellent graft function.
In Pediatric En Bloc Multivisceral Transplantation (N = 5)
Three of the 4 pediatric recipients reported by Kunzler de Oliveira Maia et al. [14] underwent pediatric en bloc multivisceral transplantation that included en bloc kidneys and a segment of donor bladder. In such complex settings, particularly in pediatric recipients, performing separate ureteral anastomoses for very small donor ureters carries a significant risk of developing either ischemia/necrosis (which would include urinary leakage) or ureteral stricture/obstruction (or both). Use of a donor bladder segment or the entire bladder with intact ureterovesical junctions offers a practical surgical solution, reducing technical complexity and minimizing the risk of urological complications. The donor bladder is then anastomosed directly to the recipient’s bladder, simplifying urinary drainage and preserving natural anti-reflux mechanisms.
Notably, the first patient (patient #2 in the Kunzler de Oliveira Maia et al. [14] report) was a 7-years old female; donor age was 3 years. This patient had a reasonably compliant bladder; thus, approximately 40%-50% of the donor bladder was included here. The second patient was a 12-month-old male; donor age was 6 months. This patient underwent a Mitrofanoff catheterizable stoma procedure 48 h after the multivisceral transplant, using a recipient bladder-based flap. Because this recipient congenitally had a hypoplastic bladder, nearly the entire donor bladder (roughly 90%) was used for urinary tract reconstruction. These first 2 patients were alive with functioning grafts at 12 year and 9 year post-transplant, respectively. The third patient was a 3 year and 7 month-old male who received multivisceral organs including kidneys and bladder from a 12-month-old donor. This patient had a reasonably compliant bladder; thus, approximately 40%-50% of the donor bladder was included here. Unfortunately, this patient died of sepsis at 2mo post-transplant with intestinal graft failure (due to severe acute rejection) but with a functioning kidney allograft and a serum creatinine (at 1mo post-transplant) of 0.29 mg/dL.
Two additional male pediatric patients aged 5-years and 8-years underwent a combined pediatric en bloc multivisceral, double kidney transplant with bladder inclusion. Donor ages were 20 months and 3 years, respectively. Since both patients had reasonably compliant bladders, only 40%-50% of the donor bladders were included, respectively. With follow-up beyond 4 years, one recipient demonstrated excellent graft function, having a serum creatinine level of 0.70 mg/dL at 4 years post-transplant. Unfortunately, the second patient developed irreversible coagulopathy and sepsis, leading to death at 2 days post-transplant.

Comments (0)