Study design and population
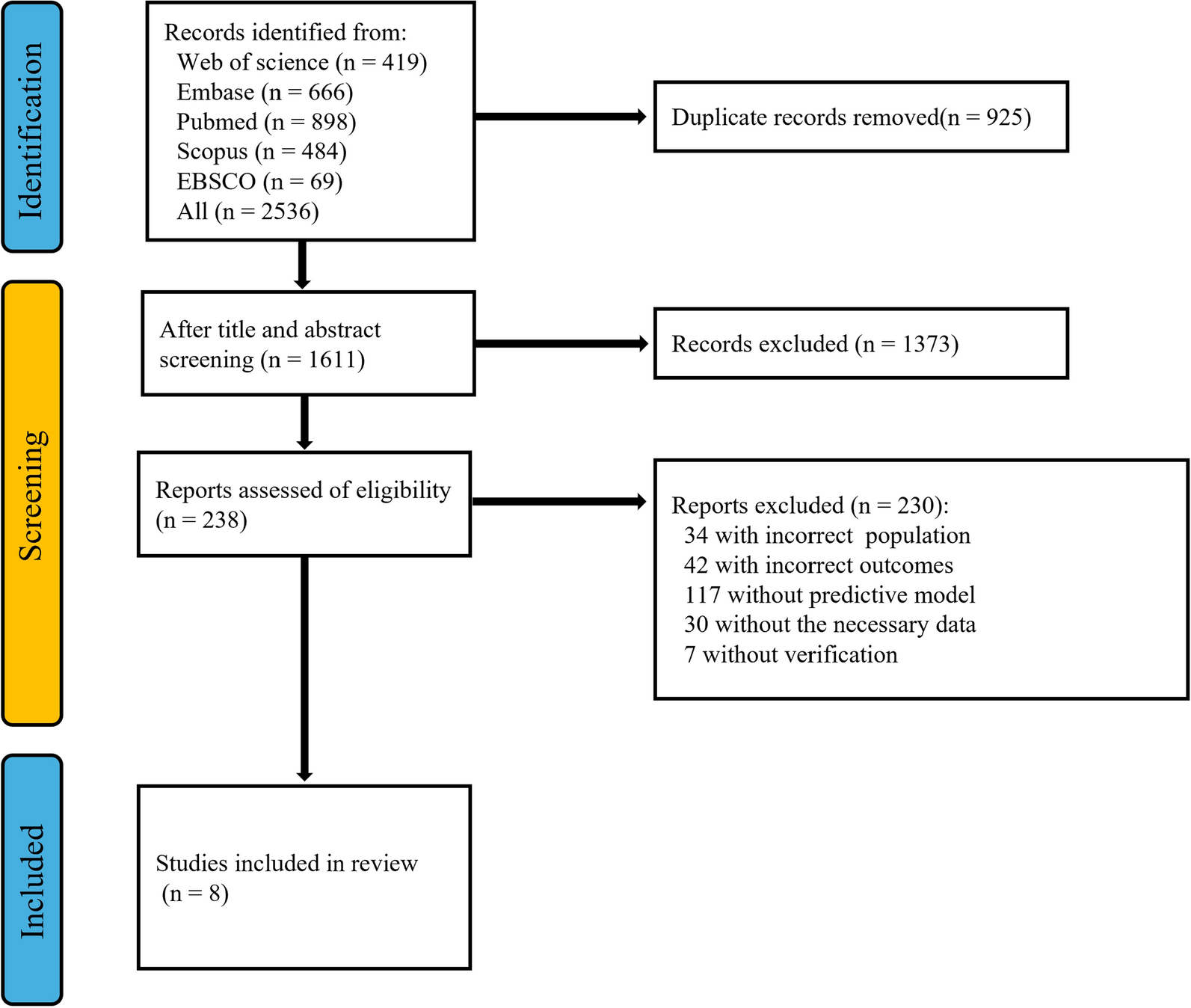
This single-center retrospective study included critically ill, adult (> 18 years old) patients hospitalized at the tertiary intensive care unit (ICU) of the University Hospital Zurich, Switzerland, an academic teaching hospital. The local ICU provides care for patients from all medical and surgical fields. All patients undergoing extracorporeal membrane oxygenation (ECMO) support and intravenous teicoplanin treatment were eligible for study inclusion from 1.1.2010 to 19.07.2023. Patients were included irrespective of the admitting diagnosis and independent of the ECMO configuration (veno-venous, veno-arterial or others with, e.g., multiple cannulation sites). Patients aged < 18 years were excluded. Other exclusion criteria were documented verbal or written refusal to participate in this study. Patients were also excluded if teicoplanin was not administered for any portion of the ECMO treatment period (e.g., if given only before or after the ECMO treatment period) or if no trough levels were obtained during ECMO support.
The study was conducted according to the principles of the Helsinki Declaration and was approved by the competent local Ethics committee (Cantonal Ethics Commission Zurich, BASEC Number 2023-01379).
Data collection
Data were collected with the use of two in-hospital electronic medical records databases, the KISIM (Cistec AG, Zurich, Switzerland) and the Patient Data Management System (PDMS) MetaVision (iMDsoft, Dusseldorf, Germany). Collected data included baseline demographic data (including age, gender and body mass index), comorbidities (including cardiovascular conditions, pulmonary diseases, renal insufficiency) and immunosuppression (including patients with prior organ transplantation), ICU admitting diagnoses, and the indication for teicoplanin treatment (empiric vs. targeted). Moreover, ICU treatment modalities and scores (e.g., organ support and scores such as the Sequential Organ Failure Assessment Score SOFA and the Simplified Acute Physiology Score SAPS II) and patient outcomes (including ICU length of stay and survival) were gathered. Teicoplanin trough levels and dosages over time were obtained from the medical records (see below).
Teicoplanin prescribing policy and assessment
In our hospital, intravenous teicoplanin is normally administered for empiric or targeted coverage of Gram-positive microorganisms. The standard loading dose is 400 mg infused at 0 h, 12 h and 24 h. Thereafter, 400 mg are administered every 24 h. Measurement of teicoplanin trough levels (TCtrough) is recommended prior to the fifth dose and this also applies to dose adjustments. In case of renal impairment, TCtrough levels are recommended to be measured prior to the second dose, in order to detect potential overdosing early. If the estimated glomerular filtration rate (eGFR) is subnormal, teicoplanin starting dosage is adjusted (eGFR 40–60 ml/min: 200 mg/24 h, eGFR < 40 ml/min: 100 mg/24 h).
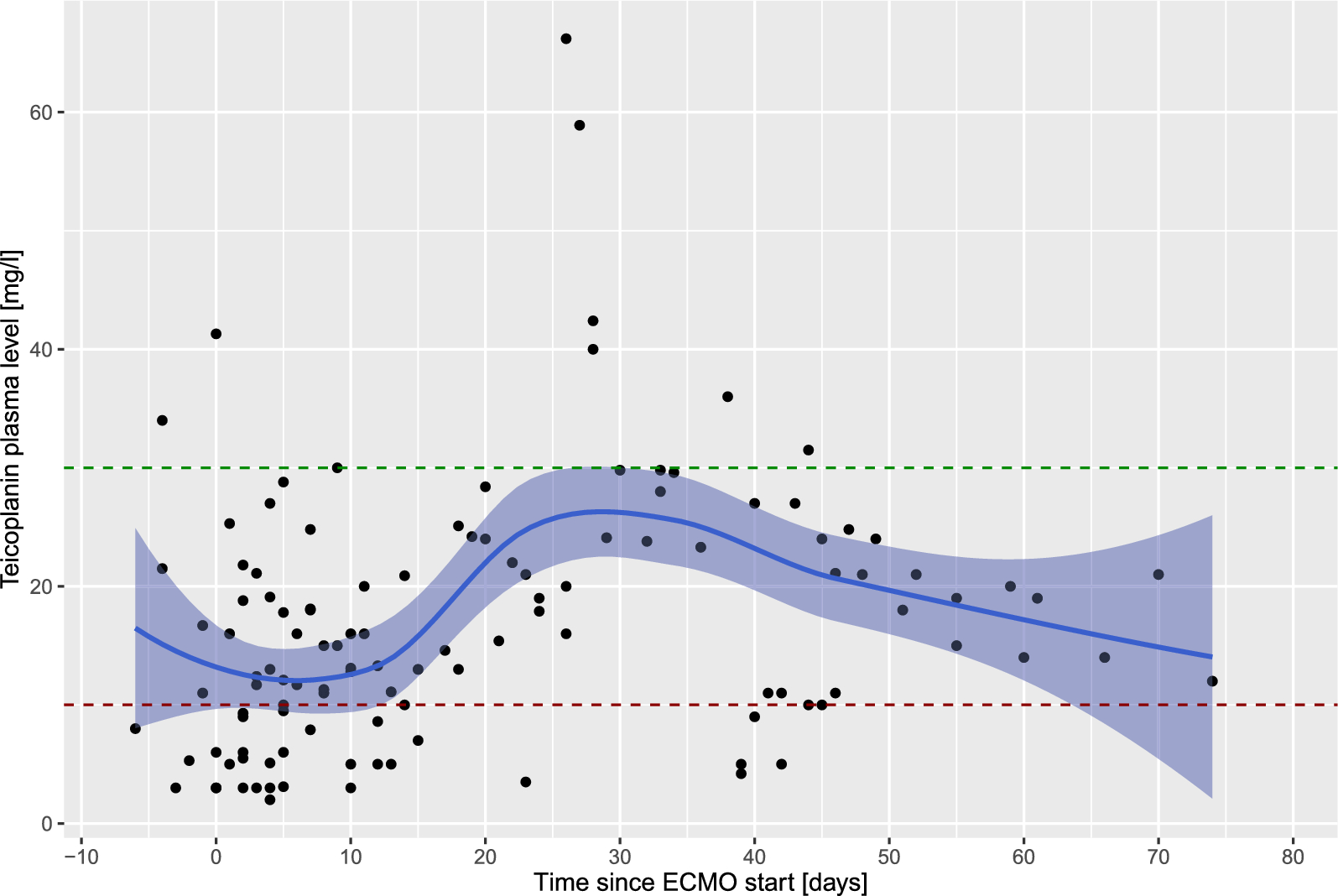
In case the patient is undergoing continuous renal replacement therapy, 200–400 mg teicoplanin every 24 h are recommended. In general, TCtrough of 10–30 mg/l are targeted. TCtrough < 10 mg/l are considered insufficient [13], whereas TCtrough > 30 mg/l are considered toxic. In case TCtrough are not within the target ranges, dose adaptations can be prescribed by the clinicians in charge. In case a measured TCtrough is toxic (i.e., > 30 mg/l), no more teicoplanin is administered, however TCtrough are measured on a daily basis. As soon as the teicoplanin levels return to the normal range (i.e., 10–30 mg/l), teicoplanin is reinstituted in a lower dose according to the clinicians in charge. In case TCtrough are subnormal (i.e., < 10 mg/l), the dose is increased according to the clinicians in charge taking pharmacokinetic considerations and renal function (or replacement therapy) into account. After increasing the dose, subsequent teicoplanin levels are again measured prior to the fifth dose or prior to the second dose in case of renal impairment, respectively.
Owing to lacking data, there is no specific in-house protocol for laboratory TCtrough assessments in patients undergoing ECMO support. In order to reflect real-world practice and to evaluate the potential impact of ECMO treatment on teicoplanin levels, TCtrough were assessed as available from the medical records, beginning up to one week before ECMO implantation (when available) and continuing throughout the ECMO treatment period.
Continuous renal replacement therapy
As a standard, the multiFiltrate CRRT device with AV1000 membranes (mFT, Fresenius Medical Care, Bad Homburg, Germany) is used in our institution. The standard configuration is continuous veno-venous hemofiltration with regional citrate anticoagulation. In case of documented citrate accumulation, we switch to heparin anticoagulation or continuous veno-venous hemodiafiltration without citrate administration, depending on the presumed bleeding risk of the patient. An initial dialysis dosage of 20–25 ml/kg/h and a blood flow:dialysate ratio of 1:20 is targeted, which both can be adapted according to the clinical circumstances such as acid–base conditions. In case fluid removal is intended, fluid is directly removed via the dialysis device according to the clinicians in charge.
Study outcomes
The primary outcome of this study was the proportion of patients with insufficient or toxic TCtrough during ECMO support. Secondary outcomes included the observed TCtrough and teicoplanin dosages over time during ECMO support and dependent on the presence of continuous renal replacement therapy (CRRT), as well as the occurrence of side effects (such as hemotoxicity, hepatotoxicity or skin changes) leading to discontinuation of teicoplanin treatment.
Statistical analysis
Data were expressed as median and interquartile ranges IQR (25th−75th percentile) for continuous variables or as absolute numbers and percentages for categorical variables, as appropriate.
TCtrough and teicoplanin dosages over time were modeled by means of a non-parametric local estimated polynomial regression with a tri-cubic weighting function and an alpha of 0.75, including the presence of CRRT. Statistical analysis was performed through a fully scripted data management pathway using the R environment for statistical computing version 4.2.1. A two-sided p < 0.05 was considered statistically significant.



Comments (0)